
Home » Psychology (Page 4)
Category Archives: Psychology
Science Proves It: Fat-shaming Doesn’t Work
2250 words
Milo Yiannopoulos published an article yesterday saying that “fat-shaming works”. It’s clear that the few papers he cites he didn’t read correctly while disregarding the other studies stating the opposite saying “there is only one serious study”. There is a growing body of research that says otherwise.
He first claims that with the knowledge of what he is going to show will have you armed with the facts so that you can hurl all the insults you want at fat people and genuinely be helping them. This is objectively wrong.
In the study he’s citing, the researchers used a quantitative analysis using semi-structured interview data (which is used when subjects are seen only one time and are instructed by the researchers what the guidelines of the experiment will be in order to get the reliable, comparable, and quality data) on 40 adolescents who lost at least 10 pounds and maintained their weight loss for at least a year. This guideline came from Wing and Hill (2001) who say that maintaining a 10 percent weight loss for one year is successful maintenance. He claims that the abstract says that bullying by the peer group induces weight loss. Though, it’s clear that he didn’t read the abstract correctly because it says:
In contrast to existing literature, our findings suggest that primary motivating factors for adolescent weight loss may be intrinsic (e.g., desire for better health, desire to improve self-worth) rather than extrinsic. In addition, life transitions (e.g., transition to high school) were identified as substantial motivators for weight-related behavior change. Peer and parental encouragement and instrumental support were widely endorsed as central to success. The most commonly endorsed weight loss maintenance strategies included attending to dietary intake and physical activity levels, and making self-corrections when necessary.
Peer encouragement and instrumental support were two variables that are the keys to success in childhood weight loss maintenance, not fat-shaming as he claims.
The same study found that obese people were more likely to lose weight around “life transitions,” like starting high school. In other words, people start to worry about how others will see them, especially when they need to make a good first impression. Fear of social judgement is key. So keep judging them.
The study didn’t find that at all. In fact, it found the opposite.
According to a new study, while most teens’ weight loss attempts don’t work, the ones who do lose weight successfully, quite simply, do it for themselves, rather than to please their (bullying) peers or (over-pressuring) parents.
He then cites a paper from the UCLA stating that social pressure on the obese (fat-shaming) will lead to positive changes. Some of the pressures referenced are:
If you are overweight or obese, are you pleased with the way you look?
Are you happy that your added weight has made many ordinary activities, such as walking up a long flight of stairs, harder?
The average fat person would say no to the first two.
Are you pleased when your obese children are called “fatty” or otherwise teased at school?
Fair or not, do you know that many people look down upon those excessively overweight or obese, often in fact discriminating against them and making fun of them or calling them lazy and lacking in self-control?
Self-control has a genetic component.In a 30 year follow-up to the Marshmallow Experiment, those who lacked self-control during pre-school had a higher chance of becoming obese 30 years later. Analyzing self-reported heights and weights of those who participated in the follow-up (n=164, 57 percent women), the researchers found that the duration of the delay on the gratification task accounted for 4 percent of the variance in BMI between the subjects, which, according to the researchers, was responsible for a significant portion of the variation in the subjects. The researchers also found that each additional minute they delayed gratification that there was a .2 reduction in BMI.
Why? Because people change their health and dietary habits to mimic that of their friends and loved ones, especially if they spend lots of time around them. Peer pressure encourages people to look like the people they admire and whose company they enjoy. Unless there’s a more powerful source of social pressure (say, fat shaming) from the rest of society, of course.
Not even thinking of the genetic component. The increase in similarity relative to strangers is on the level of 4th cousins. Thus, since ‘dietary habits are mimicked by friends and family’, what’s really going on is genotypic matching and that, not socialization, is the cause for friends and family mimicking diets.
There is only one serious study, from University College London, that suggests fat-shaming doesn’t work, and it’s hopelessly flawed. Firstly, it’s based on survey data — relying on fat people to be honest about their weight and diets. Pardon the pun, but … fat chance!
Moreover, the study defines “weight discrimination” much like feminists define “misogyny,” extending it to a dubiously wide range of behaviours, including “being treated poorly in shops.” The study also takes survey answers from 50-year olds and tries to apply them to all adults. But in what world do 20-year-olds behave the same way as older people?
The paper he cites, Perceived Weight Discrimination and Changes in Weight, Waist Circumference, and Weight Status, does say what he claims. However, the researchers do say that due to having a sample of people aged 50 and older that it wasn’t applicable to younger populations (as well as other ethnicities, this sample being 97.9 percent white). (Which you can tell he did not read, and if he did he omitted this section.)
The researchers found that 5.1 percent of the participants reported being discriminated on the basis of their weight. They discovered that those who experienced weight discrimination were more likely to engage in behaviors that promoted weight gain, and were more likely to see an increase in weight and waist circumference. Also observed, was that weight discrimination was a factor in early onset obesity.
Present research indicates that in addition to poorer mental health outcomes, weight discrimination has implications for obesity. Rather than motivating people to lose weight, weight discrimination increases the risk for obesity. Sutin and Terraciano (2013) conclude that though fat shaming is thought to have a positive effect on weight loss and maintenance, it is, in reality, associated with maintenance of obesity. Also seen in this sample of over 6,000 people was that those who experienced weight discrimination were 2.5 times more likely to become obese in the next few years.Further, obese subjects were 3.2 times as likely to remain obese over the next few years.
Sutin et al (2014) also showed how weight discrimination can lead to “poor subjective health, greater disease burden, lower life satisfaction and greater loneliness at both assessments and with declines in health across the four years”.
Puhl and Heuer (2010) says that weight discrimination is not a tool for obesity prevention and that stigmatization of the obese leads to threatened health, the generation of health disparities and, most importantly, it interferes with effective treatments.
Tomiyama (2014) showed that any type of fat shaming leads to an increase in weight and caloric consumption.
Shvey, Puhl, and Brownell (2011) found in a sample of 73 overweight women, that those who watched a video in which weight discrimination occurred ate 3 times as many calories than those who did not see the video. The authors conclude that despite people claiming that weight discrimination works for weight loss, the results of the study showed that it leads to overeating, which directly challenges the (wrong) perception on weight discrimination being positive for weight loss.
Participants were from an older population, in which weight change and experiences of weight discrimination may differ relative to younger populations so findings cannot be assumed to generalize
Puhl and King (2013) show that weight discrimination and bullying during childhood can lead to “depression, anxiety, low self-esteem, body dissatisfaction, suicidal ideation, poor academic performance, lower physical activity, maladaptive eating behaviors, and avoidance of health care.”
I expect we’ll see more of these pseudo-studies, and not just because academics tend to be lefties. Like climate scientists before them, I suspect a substantial number of “fat researchers” will simply choose to follow the political winds, and the grant money that follows them, rather than seeking the truth.
He is denying the negative implications of fat-shaming, disregarding the ‘one study’ (or so he claims) that shows the opposite of what he cited (which he didn’t read fully). I also like how these studies are called ‘pseudo-studies’ when the conclusion that’s found is a conclusion he doesn’t like. Really objective journalism there.
The reverse is also true. Just being around attractive women raises a man’s testosterone.
The researchers say that talking with a beautiful woman for five minutes led to 14 percent increase in testosterone and a 48 percent increase in cortisol, the anti-stress hormone.
Of course, this has its grounds in evolution. When two people are attracted to each other, they begin to mimic each other’s movements and using the same body language unconsciously. The researchers he cited concluded that “women may release steroid hormones to facilitate courtship interactions with high-value men“. This, of course, has an evolutionary basis. Women seek the best mate that will be able to provide the most for them. Men and women who are more attractive are also more intelligent on average with the reverse holding true for fat people, who are uglier and less intelligent on average.
Though it would be to un-PC to conduct an experiment proving it, it stands to reason that looking at fat, ugly people depresses testosterone. This is certainly how any red-blooded man feels when looking at a hamplanet.
Depressed testosterone is associated with many negative health outcomes, and thus the mere presence of fat people is actively harming the population’s health — particularly men’s, since we’re more visual. We ban public smoking based on the minuscule effects of “passive” intake, so why aren’t the same lefty, public-health aware politicians clamouring for a ban on fat people being seen in public?
A study conducted on people’s hormonal response to the obese and overweight may indeed show a decrease in testosterone and cortisol. Though, these hormonal responses are temporary, which he doesn’t say.
Instead, the same lefties who want to stop us having fags or drinking too much in public (and even alcoholics and chain smokers are healthier than the obese) are the same ones urging the authorities to treat “fat-shaming” as a crime and investigate it. Insane!
There are, contrary to popular belief, obese people who are metabolically healthy. Blüher (2012) reviewed the data on obese patients and found that 30 percent of them were metabolically healthy with the obese patients having similar levels of insulin sensitivity similar to lean individuals.
Moreover, new research has found that having a BMI of 27 leads to a decrease in mortality. In a huge study of over 120,000 people, the researchers gathered people from Copenhagen, Denmark, recruiting people from 1976 to 2013. They were then separately compared to those who were recruited in the 70s, 90s, and 00s. Surprisingly, the BMI linked with the lowest risk of having died from any cause was 23.7 in the 70s, 24.6 in the 90s, and 27 from 2003-2013. Due to the results of this study, the researchers are arguing that BMI categories may need adjusting.
As shown in that 2014 study, young people in particular are concerned about what their peers think about them, especially when they start high school. That’s why it’s so critical to let them know that their instincts are correct, and that they can’t be “healthy at any size.”
If you can be unhealthy at any size, why can’t you be ‘healthy at any size’? As I’ve shown, those with a BMI of 27, on average, are metabolically similar to those with to those with lower BMIs. Since, in the study previously cited, BMI increased while mortality decreased, technological advancements in caring for diseases, such as Diabetes Mellitus, improved, this is one possible explanation for this.
Those with a BMI under 25 may still suffer from negative effects, the same as obese people. They may suffer from metabolic syndrome, high triglycerides, low HDL, small LDL particles, high blood sugar and high insulin. Those who are skinny fat need to worry more about their vital organs, as the fat deposits they carry are white fat which is wrapped around the vital organs in the body. These are some of the reasons why being skinny fat can be more dangerous than being obese or overweight: they think that because their BMI is in the ‘normal range’ that they’re fine and healthy. Clearly, sometimes even being ‘underlean’ can have serious consequences worse than obesity.
Then he brings up smoke shaming and bills being passed to stop smokers from smoking in certain public areas lead to a decrease in smoking, so fat shaming makes sense in that manner.
Except it doesn’t.
Humans need to eat, we don’t need to smoke. Moreover, since the rising rates in obesity coincide with the increase in height, it has been argued by some researchers that having an obese population is just a natural progression of first world societies.
Fat shaming doesn’t work. It, ironically, makes the problem worse. The physiological components involved with eating are a factor as well. It is known that the brain scans of the obese and those addicted to cocaine mirror each other. With this knowledge of food changing the brain, we can think of other avenues that do not involve shaming people for their weight, which increases the problem we all hate.
Individual and Racial Differences in IQ and Allele Frequencies
1300 words
In the past 100 years since the inception of the IQ test there have been racial differences in test scores. What causes these score differences? Genetics? Environment? Both? Recently it has come out that populations do differ in allele frequencies that affect intelligence. David Piffer’s “forbidden paper on population genetics and IQ” was rejected by the new editor of the journal Intelligence. In the paper, he shows how IQ alleles vary in frequency by population. One reviewer even said it should not be put up for review, which Piffer believes there was a hidden agenda or a closed minded attitude. He even puts reviewers comments and responds to them. He says science should be transparent, which is why he’s showing the researchers’ comments on his paper.
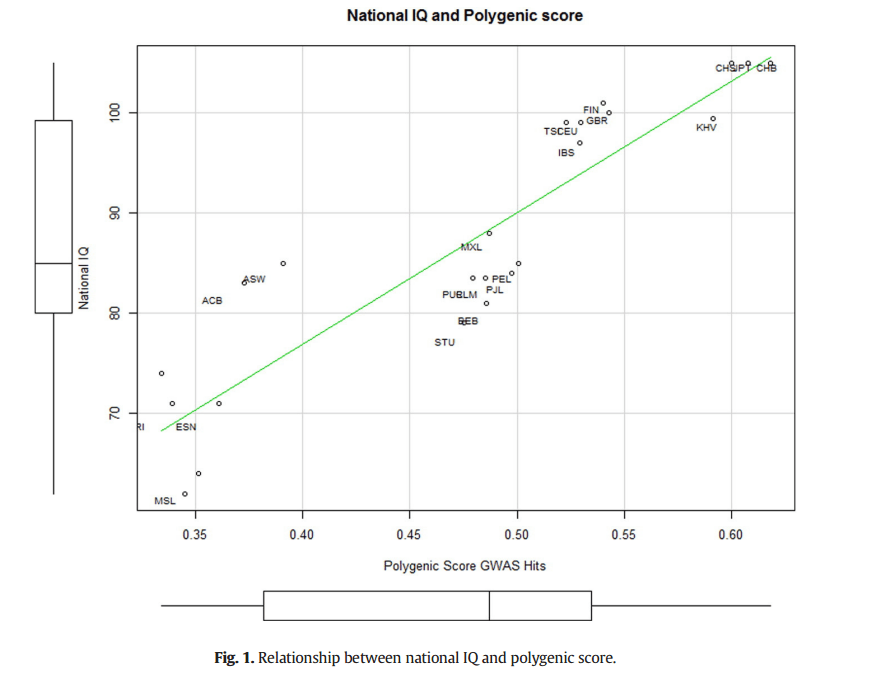
His December, 2015 paper titled: A review of intelligence GWAS hits: Their relationship to country IQ and the issue of spatial autocorrelation shows that there are differing allele frequencies in which IQ between populations that affect IQ which are then correlated highly with average IQ by country (r=.92, factor analysis showed a correlation of .86). There was also a “positive and significant correlation between the 9 SNPs metagene and IQ”(pg. 45). However, Piffer does conclude that since the 9 alleles are present within all populations (Africans, Latin Americans, Europeans, South Asians, and East Asians) that the intelligence polymorphisms don’t appear to be race-specific, but were already present in Homo Sapiens before the migration out of Africa. He then goes on to say that it’s extremely likely that the vast majority of alleles were subject do differential selection pressure which lead increases in cognitive abilities at different rates rates in different geographical areas (pg. 49). It’s of course known that differing populations faced differing selection pressures which then lead to genotypic changes which then affected the phenotype. It’s not surprising that genes that correlate strongly with intelligence have differing frequencies in different geographical populations; it’s to be expected with what we know about evolution and natural selection. Below is the scatter plot showing the relationship between polygenic score GWAS (Genome Wide Association Studies) hits and IQ:
The fact that these differences exist should not come as a shock to those who want to seek the truth, but as seen with how David Piffer didn’t even get consideration for a revision, this shows the bias in science to studies such as this that show racial differences in intelligence exist.
Piffer’s data also corroborates Lynn and Meisenberg’s (2010) finding of a correlation of .907 with measured and estimated IQ. This shows that the differing allele frequencies affect IQ, which then affect a countries GDP, GNP, and over all quality of life.
With a sample with a huge n (over 100,000 subjects) cognitive abilities tests were performed on verbal-numerical reasoning, memory and reaction time (a huge correlate for IQ itself, see Rushton and Jensen, 2005). Davies et al (2016) discovered that there were significant genome-wide SNP based associations in 20 genomic regions, with significant gene-based regions on 46 loci!! Once we find definitive proof that intelligence differences vary between individuals, as well as the loci and genomic regions responsible, we can then move on to difference in allele frequency in depth (which Piffer 2015 was one of the starts to this project).
Moreover, genes that influence intelligence determine how well axons are encased in myelin, which is the fatty insulation that coats our axons, allowing for fast signaling to the brain. Thicker myelin also means faster nerve impulses. The researchers used HARDI to measure water diffusion in the brain. If the water diffuses rapidly in one direction, that shows the brain has very fast connections. Whereas a more broad diffusion would indicate slower signaling, thus lower intelligence. It basically gives us a picture of an individuals mental speed. Thinking of reaction time tests where Asians beat whites who beat blacks, this could possibly show how differing process times between populations manifest itself in reaction time. Since myelin is correlated with fast connections, we can make the inference that Asians have more than whites who have more than blacks, on average. The researchers also say that it’s a long time from now, but we may be able to increase intelligence by manipulating the genes responsible for myelin. This leads me to believe that there must be racial differences in myelin as well, following Rushton’s Rule of Three.
Since the mother’s IQ is the best predictor of the child’s IQ, this should really end the debate on its own. Sure on average, intelligent black mothers would birth intelligent children, but due to regression to the mean, the children would be less intelligent than the mother. JP Rushton also says that regression works in the opposite way. Both blacks and whites who fall below their racial means will have children who regress to the means of 85 and 100 respectively, showing the reality of the genetic mean in IQ between the races.
Why would differing allele frequencies lead to the same cognitive processes in the brain in genetically isolated populations? I’ve shown that brain circuits vary by IQ genes, and populations do differ in this aspect, like all other differing genotypic/phenotypic traits.
East Asians have bigger brains, as shown by MRI studies. Rushton and Rushton (2001) showed that the three races differ in IQ, brain size, and 37 different musculoskeletal traits. We know that West Africans and West African-descended people have genes for fast twitch muscle fibers (Type II) (Nielson and Christenson, 2001). Europeans and East Asians have slow twitch muscle fibers (Type I) for strength and endurance. (East Africans have this as well, which allows for ability to run for distance, which fast twitch fibers do not allow for. The same is true for slow twitch fibers and sprinting events.) Bengt Saltin showed that European distance runners have up to 90 percent slow twitch fibers (see Entine, 2000)! So are genetic IQ differentials really that hard to believe? With all of these differing variables in regards to intelligence that all point to a strong genetic cause for individual differences in other genes that lead to stark phenotypic differences between the races, is it really not plausible that populations differ in intelligence, which is largely inherited?
Is it really plausible that differing populations would be the same cognitvely? That they would have the same capacity for intelligence? Even when evolution occurred in differing climates? The races/ethnicities differ on so many different variables with differing genes being responsible for it. Would IQ genes really be out of the question? Evolution didn’t stop from the neck up. Different populations faced different selection pressures, so different human traits then evolved for better adaption in that environment. Different traits clearly developed in genetically isolated populations that had no gene flow with each other for tens of thousands of years. These differing evolutionary environments for the races put different pressures on them, selecting some for high IQ alleles and others for low IQ alleles.
We are coming to a time where intelligence differences between populations will become an irrefutable fact. With better technology to see how differing genes or sets of genes affect our mind as well as physiology, we will see that most all human differences will come down to differing allele frequencies along with differing gene expression. Following Rushton’s simple rule based on over 60 variables, East Asians will have the most high IQ alleles followed by Europeans and then blacks. The whole battery of different cognitive abilities tests that have been conducted over the past 100 years show us that there are differences, yet we haven’t been able to fully explain it by GWAS and other similar techniques. Charles Murray says within the next 5 to 10 years we will have definitive proof that IQ genes exist. After that, it’s only a matter of time before it comes out that racial differences in IQ are due to differing allele frequency as well as gene expression.
How to Use Current Knowledge to Effectively Treat the Symptoms of PWS Patients
2550 words
Abstract
Researchers have tried to manage those with Prader-Willi’s Syndrome for multiple decades. Though they have greatly curbed some of the implications of the disease, there are still numerous ways in which we can better use our knowledge of how the disease manifests in order to better help those suffering from PWS. Looking at research into how the extra chromosome 15 is linked to low IQ; IQ and its relationship to obesity; how the ability to delay gratification leads to obesity; growth hormone treatment to better treat low muscle mass and higher body fat; and finally using reinforcement theory to punish a response, where doing so will greatly diminish the probability of that response occurring again in the future; all of these factors can be used in conjunction to better mitigate problems from the disease. By examining all of these variables and thinking of better ways to handle them, we can then think of other, better ways to manage those with PWS. In doing so, we can better increase the quality of life of those suffering from PWS, as well as have less of a strain on healthcare workers who care for them. With new advances in technology with CRISPR Cas9, we can then edit the genomes and chromosomes of those suffering from this disease.
How to Use Current Knowledge to Effectively Treat and Manage the Symptoms of PWS Patients
How can we use the research on chromosomal differences, research on their IQ differences and their lack of ability to delay gratification that, in turn, would help those individuals with the disease? Seventy percent of PWS cases are attributed to the deletion of chromosome 15 (Ledbetter et al, 1981). Maternal uniparental disomy, which involves receiving an extra chromosome 15 from the mother, is yet another cause of PWS (Wang, 2004).
Whittington, Holland and Webb (2009) found that there was variation between families in deletion of chromosome 15. They found that the PWS and sibling IQ correlation was .3, a modest correlation. What was also noticed was that there were subtype differences which manifested itself in the familial differences in IQ. As they expected, the correlation with normal siblings and those with PWS was .5 in those who suffered from PWS due to unilateral disomy. But in the second subset (the chromosomal deletion subset), the correlation was negative at -0.07. Their research shows great promise in the role of chromosome 15 and IQ. They end up concluding that there needs to be an explanation for the small genetic differences between them. How can we use these differences in IQ to help people with PWS and what does this suggest for other symptoms of their disease?
Kanazawa (2014), reviewed the data on the research between obesity and IQ. What he found was that those studies that concluded that obesity causes lowered intelligence only observed cross-sectional studies. Longitudinal studies that looked into the link between obesity and intelligence found that those who had low IQs since childhood then became obese later in life and that obesity does not lead to low IQ. The average IQ for an individual suffering from PWS is 65 (Butler, Lee and Whitman 2006, p. 13), so that is one reason they have a tendency to be obese. He states that those with IQs below 74 gained 5.19 BMI points, whereas those with IQs over above 126 gained 3.73 BMI points in 22 years, which is a statistically significant difference. Also noted, was that those at age 7 who had IQs above 125 had a 13.5 percent chance of being obese at age 51, whereas those with IQs below 74 at age 7 had a 31.9 percent chance of being obese. This data makes it clear: low IQ is correlated with obesity, so we, therefore, need to find sufficient measures to help those with lower IQs who also suffer from PWS to better maintain their good health. Since we can better identify those PWS individuals who have lower IQs based on how they got the disease, we can then show them more attention in an effort to have them manage their gratification better. Moreover, the lack of ability to delay gratification is also correlated with low IQ (Mischel, Ebbeson, and Zeiss, 1972).
Schlam et al. (2013) observed in a follow-up study to the Marshmallow Experiment that found in a longitudinal study of individuals they found forty years later from the original Marshmallow Experiment, due to inability to delay gratification forty years previously, that was one cause of becoming obese forty years later. Due to PWS sufferers having lower average IQs, and, therefore, a lack of ability to delay their gratification, this is direct evidence that those PWS sufferers with low IQs need more stringent measures to be taken on them, which would then be helpful to those individuals who have a hard time delaying their gratification, which is partially caused by the drop in IQ due to the additional chromosome 15. We can see how those with PWS act; they want their gratification now and do not want to wait for it. This is why, when unsupervised, that those with PWS gorge on the food they understand they should not have, but do so, nevertheless, since their low IQ is correlated with lack of ability to delay gratification, which manifests itself in their obesity. We clearly need to find better methods in which to help those with low ability to delay gratification, which would strongly help those suffering from PWS.
Dykens et al (1997) note that those with PWS have hyperphagia, which correlates with their insatiable want for food. They state that the lack of fullness is due to an altered function of the hypothalamus, which is the part of the brain that is in control of feelings of satiety. Certain States gave restrictions to homes that take care of those with PWS and have come under fire because of this, mainly due to human rights violations. We must ask, then, should we limit their access to food if it will prolong their lives? Will doing so inhibit their freedom to do as they choose? PWS sufferers also have coronary heart problems; one could argue that given their free ability to choose what they want to do unfettered will lead to premature death due to obesity-related complications. Does their disease truly not allow them to learn the consequences of their behavior? Do they have the intellect to really understand the consequences of their actions of consuming too much food? There is no established or known way to control those with insatiable eating habits due to hyperphagia. So would the best course of action to take with those with PWS actually be to constantly monitor them and to lock access to easily attainable food? My answer is yes, however, there is a clear fine line in whether restricting access to food and constantly monitoring those with PWS infringes on their human rights, or that doing so actually will help them live better, healthier lives since they would have the constant supervision around them to better control their out of control eating habits. When negative actions occur, one idea that can be shown to them is constant positive reinforcement so that they may be better able to understand that what they are doing is harmful to their bodies. We can then use positive reinforcement when they do reach a healthy weight, so, in turn, they will have a higher chance of keeping a healthy weight. They may reap the benefits of positive reinforcement, and stick more closely to their program, and therefore, stay healthy.
The hormone ghrelin is secreted from the hypothalamus. With an altered hypothalamus, this would cause ghrelin levels to overload; then the individual suffering from PWS would feel the need to insatiably gorge on food due to this chemical imbalance in the brain. Ghrelin increased feeding in rats and ghrelin is the physiological mediator of feeding and probably has a function in growth regulation by stimulating feeding and release of growth hormone (Nakazato et al, 2001). There is a correlation between want of food, ghrelin release and growth hormone production. By attempting to mediate these variables, those who suffer from PWS will be able to better control their eating habits through positive reinforcement and better, more sustainable habits. Since whenever we eat we get a release of ghrelin that makes us hungry, people pretty much set their own eating times by eating multiple times a day. This affects PWS patients the same way. They can’t stop eating, due in part to constantly eating which constantly releases ghrelin in their body.
PWS sufferers have low muscle tone and, conversely, more body fat. Growth hormones may be a valid way of alleviating that problem, which in turn will give them a slightly higher resting metabolic rate so that they may burn slightly more calories, in an effort to stay healthier. Growth hormone therapy is great for those with PWS though they are largely inactive and lead a sedentary lifestyle, the growth hormone will allow them to have less body fat and more muscle mass. As noted earlier in my paper, those suffering from PWS have altered function in their hypothalamus, which is also where growth hormone is secreted. Aycan and Bas (2014) state that treatment with growth hormones should be strongly considered for those with PWS.
PWS sufferers are also quick to anger, which can be correlated with their sub-average IQ. They may, for instance, become irate at the fact that they do not have constant access to food, and may turn to emotional, angry and infantile outbursts in an attempt to receive what they want. This is one way that it’s tricky to treat those with the disease. How do you tell an individual with PWS who wants something “No”? Measures should be taken to show those with the disease what they are doing to their bodies in the simplest way possible as to better get the point across to them. We can help those sufferers of PWS who are quick to anger with by allowing them to discern between right and wrong ways to handle times when they don’t get what they want with positive reinforcement.
Since those who suffer from PWS have behavioral problems, there are better measures we can take to assure that they don’t have their violent outbursts. When positive reinforcement is consistently shown to an individual who has PWS, he will have more success with his program. When they do something wrong, they can then be shown positive reinforcement, and through being shown positive things with reinforcement theory, they can better learn that certain actions they take are dangerous and shouldn’t be done again, as Rushton (1980) states: “If one rewards a response, it will increase the probability of the future occurrence of that response. If one punishes a response, it will decrease the future probability of the occurrence of that response.” (p. 90).
Discussion
In this paper, I have presented causes for PWS as well as effective ways to manage the disease. To look at how IQ affects individuals in regards to obesity and because it is highly correlated with other measures as well, we can then better help those with the disease. By seeing which individuals have the parental disomy version of PWS, we can then monitor them and give them better care because of their lowered IQ and make sure they stay at a healthy weight. One of the best measures to take is to heavily restrict food, i.e., make sure ability to access food at all hours of the day is restricted along with constant supervision. Though, there are rights groups fighting for them saying that their human rights are being infringed on. In allowing them to have free reign over what, how and when they eat, they will gorge themselves to obesity, as well as lead themselves to horrible complications that come along with increased food consumption. When one is caught consuming food he or she shouldn’t be consuming, punishing them and letting them understand that the behavior they took was wrong will lead to better choices and outcomes from those choices, due in part to the main facet of reinforcement theory, that punishing a response will lead to a reduced outcome in that response that was punished happening in the future. Also, with the advent of CRISPR Cas9, we will be able to edit genomes, and therefore, eventually, put an end to PWS. It will enable us to fix the chromosomal deletion and uniparental disomy, which will eradicate this disease.
Conclusion
There are better, more helpful ways in which to help those suffering from PWS. By identifying and attempting to correct these abnormalities, those who suffer from the disease can, therefore, have a better quality of life due in part to the extra measures taken. By understanding that their lower average IQs lead to a lot of the problems associated with the disease, we can better structure methods for them to keep on a healthy track and reinforce positive behavior through reinforcement theory. Since obesity is correlated highly with low IQ, we can, therefore, use this information to better help those who suffer from PWS that have low IQs. Locking up food instead of providing free access, as well as understanding they do not have the ability to delay gratification, would be a big start to find better ways to treat sufferers of PWS. Treating negative actions with positive reinforcement through reinforcement theory will lead to better and increased prosocial behavior. It’s been shown that if you punish a response, then it will decrease the future probability of that response occurring. The advent of CRISPR Cas9 will then allow us to edit the chromosomes of those with this disease in the future. Should we use genome editing on individuals with this disease, as well as several other chromosomal/genetic diseases? I believe we should, in doing so, we will greatly increase the quality of life of those with the disease.
References
Aycan, Z., & Baş, V. N. (2014). Prader-Willi Syndrome and Growth Hormone Deficiency. Journal of Clinical Research in Pediatric Endocrinology Jcrpe, 62-67.
Butler, M. G., Lee, P. D., & Whitman, B. Y. (2006). Management of Prader-Willi syndrome (3rd ed.). New York: Springer-Verlag.
Dykens, E. M., Goff, B. J., Hodapp, R. M., Davis, L., Devanzo P., Moss, F. . . King, B. (1997). Eating Themselves to Death: Have “Personal Rights” Gone Too Far in Treating People With Prader-Willi Syndrome? Mental Retardation, 35(4), 312-314.
Kanazawa, S. (2014). Intelligence and obesity. Current Opinion in Endocrinology & Diabetes and Obesity, 21(5), 339-344.
Ledbetter, D. H., Riccardi, V. M., Airhart, S. D., Strobel, R. J., Keenan, B. S., & Crawford, J. D. (1981). Deletions of Chromosome 15 as a Cause of the Prader–Willi Syndrome. New England Journal of Medicine N Engl J Med, 304(6), 325-329.
Mischel, W., Ebbesen, E. B., & Zeiss, A. R. (1972). Cognitive and attentional mechanisms in delay of gratification. Journal of Personality and Social Psychology, 21(2), 204-218.
Nakazato, M., Murakami, N., Date, Y, et al (2001). A role for ghrelin in the central regulation of feeding Nature 409, 194-198
Rushton, J. P. (1980). Altruism, socialization, and society. Englewood Cliffs, NJ: Prentice-Hall.
Schlam, T. R., Wilson, N. L., Shoda, Y., Mischel, W., & Ayduk, O. (2013). Preschoolers’ Delay of Gratification Predicts their Body Mass 30 Years Later. The Journal of Pediatrics, 162(1), 90-93.
Whittington, J., Holland, A., & Webb, T. (2009). Relationship between the IQ of people with Prader-Willi syndrome and that of their siblings: Evidence for imprinted gene effects. Journal of Intellectual Disability Research, 53(5), 411-418.
YM Wang, L Chuang, BT Wang, et al. Maternal uniparental disomy in a patient with Prader-Willi syndrome with an additional small inv dup(15) chromosome. J Formos Med Assoc, 103 (2004), pp. 943–947
Transvestic Disorder and Gender Dysphoria Identification and Prevention
2150 words
Abstract
Transvestic Disorder comes about in early childhood and manifests itself in sexually deviant actions. Men suffering from TD who aren’t homosexual, more likely than not, show attraction to themselves dressed in women’s clothing. The signs of TD are noticed at an early age when the individual begins to cross dress. TD is also correlated highly with numerous sexually deviant actions. Fluoxetine and serotonin reuptake blockers may be able to lessen TD since it is an impulsive disorder. With TD being co-morbid with OCD, by treating OCD we can better treat TD itself and give a better quality of life to the patient suffering from the disease. Since autogynephilia and transgenderism are related, measures taken to alleviate TD and autogynephilia could be taken to alleviate symptoms of gender dysphoria, since autogynephilia leads to transgenderism.
Transvestic Disorder and Gender Dysphoria Identification and Prevention
Transvestic disorder is a paraphilic disorder, classified by the American Psychological Association (2013), in which males dress up as women to gain sexual gratification. The individual suffering from TD suffers from compulsions to want to dress as a woman, which causes distress due to the individual not wanting their secret to come out. This then leads to the quality of life of the individual to decrease due to constantly being worried about his secret coming out. TD is diagnosed when a male has sexual feelings and gets sexual arousal from dressing in women’s clothing. It is only diagnosed when these activities are ongoing for at least six months. TD is also similar to another paraphilic disorder called ‘autogynephilia’ (Lawrence, 2011), in which the subject is aroused at the thought of himself being a female, so he, therefore, then begins to dress as a woman to fulfill his sexual desires. Blanchard (1989) proposed that most gender-dysphoric males who do not show sexual arousal to men, instead show sexual arousal to themselves dressed in the opposite sex’s clothing. He concludes that the hypothesis is supported that major types of those men who cross-dress are nonhomosexual, and do so because they become aroused at the thought of dressing as a woman. The DSM V says that autogynephilia is a specifier to transvestic disorder. This is because they are characterized by the same things (American Psychological Association, 2013).
The signs of TD are noticed at very early ages. Most notable are when children begin to cross-dress at or before puberty. This then continues into their adult lives where it begins to be a problem and cause dysfunction due to needing to keep their secret. Dr. Mark Griffiths (2012) states that all though children may engage in transvestic behavior, what differentiates it between an adult suffering from TD is that the child who cross-dresses does so for excitement and pleasure, not for sexual pleasure. Though some researchers say that the disorder is brought on through childhood trauma, i.e., accidental exposure to women’s clothing or exposure to a woman who is undressing. Numerous studies have also concluded that many men who suffer from TD have had to deal with parental separation during childhood.
The American Psychological Association (2013), reports that fewer than 3 percent of males are characterized as having transvestic disorder. TD is most always seen in males, though Moser (2009) noted that in his study using the Autogynephilia Scale for Women (ASW), that out of the 29 respondents that sent back questionnaires, 90 percent would be classified as having autogynephilia. Though, by using a more meticulous definition, only 28 percent were seen to be autogynephilic (Moser, 2009).
Langstrom and Zucker (2005) observed in a sample of 2,450 18 to 60-year-olds in Sweden that transvestic disorder was correlated significantly with being separated from their parents, homosexual relations, higher masturbatory frequency, being easily aroused sexually and pornography use. Also noticed, was a positive attitude in regards to sexual arousal from pain, exposing oneself to a stranger and voyeurism were all positively correlated with TD. Langstrom and Zucker observed how TD is co-morbid with many other paraphilic disorders as well as other deviant behavior. By attempting to treat what TD is correlated with, symptoms of TD can be lessened.
Men suffering from TD and autogynephilia are told that women are the standard of beauty. They then look at themselves in the mirror and see a male and not the standard of beauty they were told of growing up. They then turn to cross-dressing to finally see their “beauty standard” in the mirror but keep it a secret. This strong want to keep their disorder a secret then leads to dysfunction. Men suffering from TD will go to any lengths to hide their secret. This then causes extreme dysfunction in their lives, which leads to a lessened quality of life.
Less than three percent of males suffer from TD in the American population, as such, it is classified as a deviant lifestyle as it deviates from the norm of the population. It causes distress due to them not wanting their secret to be discovered. This, in turn, leads to dysfunction where the individual cannot live their daily lives to the fullest due to their abnormal disorder. It finally leads to danger due to their secret beginning to consume their lives so that they’re not discovered.
There are ways to treat TD. Usmani et al (2012) follow a case study in which a 17-year-old Indian male who had occurring desires to wear his mother’s clothes. He then would masturbate in his mother’s clothes to alleviate himself. This continued on for two years so he could pleasure himself. He was caught by his parents wearing his mother’s clothes and was beaten by them for it. He then said that it is a compulsive behavior and cannot be helped. This case also shows the obsessive compulsive side to TD. They have an urge so strong they cannot help but to do it compulsively to alleviate their sexual desires. He also said that the occurring thoughts then affected his schoolwork as he was so preoccupied with the thought of wearing women’s clothes. All of his brain scans were found to be normal, so what brought on this case in the individual in the case study? He was then diagnosed with TD and prescribed fluoxetine, an antidepressant SSRI. The dose was started at 20 mg and increased by 40 mg once a day for two weeks. In his six-month follow-up, he reported lessened desire to masturbate with women’s clothes (Usmani et al, 2012).
Paraphilias and other related disorders have been thought of as sexual addictions. Though it has been argued that they are not sexual addictions, but are sexual compulsions (Stein et al, S 1992). The researchers reviewed 13 patients who showed signs of TD and were administered serotonin reuptake blockers. The symptoms of those individuals were then divided into paraphilias, non-paraphilic sexual addictions, and sexual addictions. Stein et al discovered that paraphilias had the least improvement with the reuptake blockers whereas sexual compulsions showed the best improvement. They end up concluding that paraphilias and other related disorders are on the impulsive end of the spectrum compared to the compulsive end. These impulsions, then, have those men suffering from TD have the urge to dress in women’s clothes to fulfill their sexual impulsion.
TD is co-morbid with obsessive compulsive disorder (Abdo, Hounie, de Tubino Scanavino, and Miguel, 2001). They used longitudinal case studies in which they assessed two individuals who had OCD as well as TD. They conclude that some cases of TD may be OCD related and not always be caused by gender dysphoria. Since OCD and TD are co-morbid, by treating symptoms of OCD, the want to cross-dress will lessen, which will then lessen the symptoms of TD. Treatments could include SSRI and fluoxetine, as previously stated in the paper. Other treatment for TD should be looked at, such as treatment for OCD due to the co-morbidity between the two. By doing so, feelings of wanting to cross-dress may lessen due to one of the underlying causes (OCD) of TD being treated.
Autogynephlia could also explain transgenderism.Transvestism can be called both a paraphila and a sexual orientation. Lawrence (2004) says that it can explain mid-life MtF transitions, progression from transvestism to transgenderism, the prevalence of other paraphilias among MtF transsexuals and the late development of male intrest in MtF transsexuals. However, when Lawrence says that “Hormone therapy and sex reassignment surgery can be effective treatments in autogynephilic transsexualism”, that is incorrect. The prevalence of suicide attempts among transgenders is 41 percent according to the Williams Institute, UCLA School of Law, in comparison to 4.6 percent for the average population. That’s almost ten times higher than the national average. Clearly, surgery doesn’t do anything to alleviate the feelings of gender dysphoria, and as shown in this paper, therapy and drugs like Prozac can better help to alleviate feelings of gender dysphora in transsexuals due to them being extremely similar to eachother. These two disorders greatly mirror each other. Since Lawrence (2004) observed that there is a progression from transvestism to transgenderism, using similar techniques that work on those with TD may also work on those with gender dysphoria.
Discussion
TD can be helped with the correct therapy as well as right medication. With those, impulsions to wear women’s clothes, as well as impulsions to commit abnormal acts will be greatly lessened and quality of life will be restored to a somewhat normal level. Due to co-morbidity between TD and OCD, treating OCD will, in turn, better help the patient suffering from TD. When more studies are carried out on those suffering from TD, we can see whether or not SSRI drugs and fluoxetine will have the desired effect in alleviation of the symptoms of TD. The individual in the Usmani study reported lessened symptoms and impulsions of cross-dressing, so by identifying which parts of the brain are and were activated during the fluoxetine therapy, we can then better give better care and treatment to those suffering from TD. We can also use some data from TD cases for transgenders, as TD and transgenders have a lot of things in common. With therapy as well as, maybe even fluoxetine (which is just Prozac), and high doses of testosterone/estrogen, this could possibly help to alleviate ‘gender dysphoria’. It could also lower the suicide rate as it’s completely possible that these interventions could fix them mentally.
Conclusion
There is little current literature in treating TD, due to it being a shameful disorder and many men not speaking about what they suffer from. One major way in which to help those with TD is to administer SSRI drugs, in which compulsion to cross-dress, and other attitudes associated with TD lessened. Blanchard (1989) proposed the autogynephilia theory for those transgenders who are not attracted to men. With the obseration by Lawrence (2004) on how autogynephilia and transgenderism are related, this can better help those with transgenderism, as they can get correct help and the right hormones they need, instead of the opposite hormones. SSRI therapy is a good candidate in treating TD, as drastic changes in deviant behavior are seen while the patient is taking the SSRI drug. Seeing as most cases of TD begin in childhood before puberty, by better identifying warning signs of these disorder, we can better treat those children who are at risk of developing these disorders before they become a big problem later in life. As more men come out and say that they suffer from these disorders, more studies can be carried out that corroborate the findings in the studies laid out here. It is extremely promising that these disorders can be treated with common drugs already on the market. In those individuals suffering from TD as well as OCD, by treating the OCD first (which may be an underlying cause) the symptoms of TD may be lessened and the individual may eventually have the ability to lead a life without TD. In using these measures on those with transgenderism, this could possibly alleviate suicide rates and other negative variables associated with these paraphilic disorders and sexual orientations.
References
Abdo, C.H.N., Hounie, A., de Tubino Scanavino, M., & Miguel, E.C. (2001). OCD and transvestism: Is there a relationship?. ACTA Psychiatrica Scandinavica, 103(6
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Blanchard, R. (1989). The Concept of Autogynephilia and the Typology of Male Gender Dysphoria. The Journal of Nervous and Mental Disease, 177(10), 616-623. doi:10.1097/00005053-198910000-00004
Griffiths, M. (2012, February 28) Dressed to thrill? A brief overview of transvestic fetishism. Retrieved from https://drmarkgriffiths.wordpress.com/2012/02/28/dressed-to-thrill-a-brief-overview-of-transvestic-fetishism/
Lawrence AA . Autogynephilia: An Underappreciated Paraphilia . In: Balon R, Hrsg . Sexual Dysfunction: Beyond the Brain-Body Connection. Adv Psychosom Med 2011 ; 135 – 148
Långström, N., & Zucker, K. J. (2005). Transvestic fetishism in the general population: Prevalence and correlates. Journal of Sex and Marital Therapy, 31, 87–95
Moser, C. (2009). Autogynephilia in Women. Journal of Homosexuality, 56(5), 539-547. doi:10.1080/00918360903005212
Stein DJ, Hollander E, Anthony DT, Schneier FR, Fallon BA, Liebowitz MR, Klein DF: Serotonergic medications for sexual obsessions, sexual addictions, and paraphilias. J Clin Psychiatry 1992; 53:267–271
Usmani et al, (2012) Treatment of Transvestic Fetishism With Fluoxetine: A Case Report. Iran J Psychiatry Behav Sci. 2012 Autumn-Winter; 6(2): 100–101
