
Home » Steroids
Category Archives: Steroids
Racial Differences in Steroid (AAS) Use
1550 words
I’ve written on steroid use between blacks and whites last year, but it was a smaller part of an article concerning the misconceptions people have on steroids and what they do (responding to the hysteria that the media and the like discuss with their claims of “roid rage”). I cited some studies showing that blacks use more drugs than whites; that blacks are more likely to lie about drug-use than whites; and that blacks are more likely to use steroids than whites (indeed, minorities were twice as likely to use steroids compared to whites in one study). (It is also worth noting that “roid rage” is a myth; AAS use is associated with other drug use, which explains the relationship. See Lundholm et al, 2015. For further information on this matter, see the documentary Bigger, Stronger, Faster.)
Steroids are synthetic hormones—lab-made hormones that mimic the so-called “male hormone” testosterone. Though the term “steroid” is misleading; what is being discussed are androgenic anabolic steroids (AAS), since, for example, estrogen is a steroid and does not have the muscle-building and recovery properties of AAS. The term “anabolic” refers to muscle-building whereas the term “androgenic” refers to the increase in male sexual characters. AAS abuse is associated with tendon ruptures, a lower incidence of prostate hypertrophy, anxiety, depression, and a decreased libido (Bagge et al, 2017). Furthermore, the negative effects of AAS (ab)use cause cardiovascular problems, dyslipedemia—which may impact vascular functioning, ventricular arrhythmias while training, hypertension, etc. (Goldman and Basaria, 2018). Further negative effects include raised cholesterol, hair thinning, sterility, and decreased hormone levels. Croaker (2017) notes that AAS use is prevalent throughout high school and collegiate sports, though “When the desired outcome is achieved, the results are always short lived.”
Individuals use steroids for myriad reasons—despite the well-known adverse effects. A few considered are: (1) to become better at sports; (2) to increase muscle mass (which then relates to increased recovery time so the individual can train more); and (3) they are administered a script by their primary care doctor because their testosterone levels are low for their age range. In any case, in this article, I will discuss (1) and (2).
Whichever way the racial differences in AAS use go, we can all agree on one thing: in young men, they most likely want to become better athletes. AAS use is associated with shorter recovery times (
How can you tell if any individual is using steroids? It’s very simple. An increase in upper-body mass, most notably the shoulders and traps. The reason for this is that there are more androgen receptors in the shoulders and so they respond better to the flood of synthetic hormone.
AAS (ab)use is pretty prevalent throughout America. For example, Blashill et al (2017) write that “Black, Hispanic, and White sexual minority boys reported misuse at approximately 25%, 20%, and 9%, respectively.” “Sexual minorities” refers to sexual identity and the sex of the sexual partner. “Whites” were those who said they were not “Hispanic” and were white; “blacks” were those who said that they were not “Hispanic” and were black; while “Hispanics” were those who identified as a “Hispanic” ethnicity while marking down another race. (Note that “white” and “black” are socialraces.)
The (ab)use of AAS particularly affects homosexual minorities. Blashill et al (2017) write:
Sexual orientation health disparities in anabolic steroid misuse disproportionally affect Black and Hispanic sexual minority adolescent boys …
Blashill et al (2017) conclude from the results of their study that the (ab)use of AAS by sexual minorities may be due to “muscularity-oriented body image concerns.” I have heard (albeit, anecdotally) that a lot of homosexuals use AAS in order to look good so they would fall under (2).
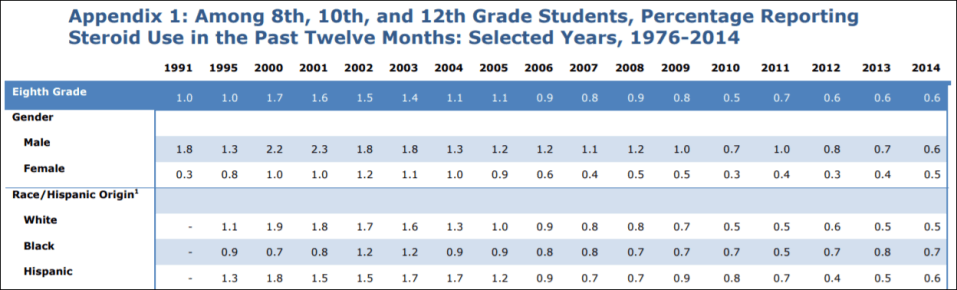
The Child Trends Data Bank writes that “There are no significant differences in use of steroids in the past 12 months when comparing whites, blacks, and Hispanics.”
Hua and Braddock (2008: 29) write that “White males reported higher prevalence of steroid use than Black males, and sport participation served as a protective factor, but only for Black males.” They conclude that:
Specifically, our results show that sport participation served as a protective factor, but only for Black males. Sports active black male adolescents reported lower rates of steroid use than Black males who were not involved in sports.
So, it seems that sport participation is protective for blacks in regard to steroid use. However, black males lie about drug use more than white males, and so, I don’t see why we should accept the conclusions of this study. I also find it hard to believe that sport participation would be protective against AAS use. Intuitively, you would expect it to cause more AAS use.
The Journal of Ethics states that AAS (ab)use was higher in white (6.2%) and “Hispanic” students (7.2%) than black students (3.6%).
Irving et al (2002) state that 2.1% of white males 7.6 percent of black males, 6.1% of “Hispanic” males, 14.8% of Hmong males, 7.9% of “other Asian”, 3.1% of Native Americans, and 11.3% of mixed race males reported AAS use. Whereas 0.5% of white females, 4.3% of black girls, 0.9% of “Hispanic” girls, 8.9% of Hmong girls, 3% of “other Asian” girls, 4.7% of Native American girls, and 4.1% of mixed race girls used steroids. Here is table 1 from Irving et al (2002):
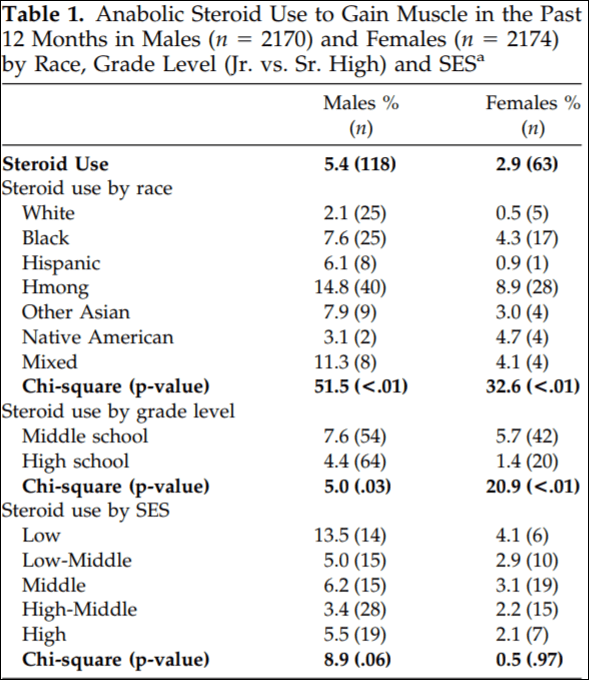
Low SES individuals were more likely to (ab)use AAS than high SES individuals in both sexes. Middle schoolers were more likely than high schoolers. (Where are they getting the AAS? Their parents? Older siblings?)
Irving et al noted that the male AAS users were least satisfied with their shoulders (we can’t all be so lucky). Fortunately for them, as noted above, the shoulders have the most androgen receptors in the body and so their shoulders will grow. However, other than not being satisfied with their shoulders, body image was not associated with AAS use in males. Female AAS users, more so than non-AAS users, were more likely to report that they used AAS to for “weight and shape.” Further, sport players were more likely than non-sport players to use AAS—as expected. In a nutshell, AAS use is associated with poor markers of physical health—most importantly because many individuals wanted to lose weight (most likely fat mass). It should be noted that those who were dissatisfied with their bodies were less knowledgable about nutrition, so to amleiorate some of this, nutrition should be taught earlier in schools.
I can’t think of any reasons why, however, Hmong males and females would be using AAS more than other ethnies. However, Irving et al (2002: 251) write:
One finding regarding the demographic characteristics of steroid users in our sample is worth noting. Steroid use was more common in non-Caucasian respondents (both male and female), with particularly high rates among Hmong participants. Initially, we were puzzled by this result and questioned its validity. However, in consultation with community informants from social service agencies that work with southeast Asian youth in the Minneapolis/St. Paul area, we were told by some informants that the “word on the street” was the Hmong youth were attempting to “bulk up” physically, by working out and using steroids. One possible explanation for this finding is that, as fairly recent immigrants (most Hmong immigrated to the U.S. in the past 20 years), Hmong youth may be “bulking up” to gain status in a culture that emphasizes physical appearance, including weight, shape, and physical strength. This interpretation is supported by anthropological research wherein exposure to western ideals of beauty and eating habits is followed by increases in weight and shape preoccupation and disordered eating practices among individuals from non-western cultures. On the other hand, it is possible that Hmong youth may have misinterpreted the question.
So if the Hmong did not misunderstand the question, it is possible, for example, that they were getting bullied (due to being new immigrants) and decided to take AAS in order to get bigger to stop the bullying.
Stilger et al (1999) note that (my emphasis):
Of the 873 high school football players participating in the study, 54 (6.3%) reported having used or currently using AAS. Caucasians represented 85% of all subjects in the survey. Nine percent were African-American while the remainder (6%) consisted of Hispanics, Asian, and other. Of the AAS users, 74% were Caucasian, 13% African American, 7% Hispanic, and 3% Asian, x2 (4,854 4) 4.203, p 4 .38. The study also indicated that minorities are twice as likely to use AAS as opposed to Caucasians. Cross tabulated results indicate that 11.2% of all minorities use/used AAS as opposed to 6.5% of all Caucasians (data not displayed).
Lastly, Green et al (2001) note that whites and blacks used AAS at the same rate, though the n = 10,850 Caucasians while for African Americans the n = 1,883.
However, unless a study notes that the participants’ blood was assayed, why should we believe the results when it’s been noted that blacks underreport and lie about drug use more than whites (Bauman and Ennett (1994); Ledgerwood et al, 2008; Lu et al, 2001)?
In sum, many studies report different results. I would say that the difference is due to cultural/social differences based on where the studies were carried out. The mixed results of these studies points to one thing: AAS use is prevalent throughout school life, and since it starts so young with many people, older siblings seem to be getting it for them. Sexual minorities are more likely to use than whites and this seems to come down to body image; Hmong seem more likely to use than non-Hmong; and the racial differences seem to hold with females as well.
Steroid Mythconceptions and Racial Differences in Steroid Use
2000 words
Steroids get a bad reputation. It largely comes from movies and people’s anecdotal experiences and repeating stories they hear from the media and other forms of entertainment, usually stating that there is a phenomenon called ‘roid rage’ that makes steroid users violent. Is this true? Are any myths about steroids true, such as a shrunken penis? Are there ways to off-set it? Steroids and their derivatives are off-topic for this blog, but it needs to be stressed that there are a few myths that get pushes about steroids and what it does to behavior, its supposed effects on aggression and so forth.
With about 3 million AAS (ab)users (anabolic-androgenic steroids) in America (El Osta et al, 2016), knowing the effects of steroids and similar drugs such as Winny (a cutting agent) would have positive effects, since, of course, athletes mostly use them.
Shrunken testicles
This is, perhaps, one of the most popular. Though the actual myth is that AAS use causes the penis to shrink (which is not true), in reality, AAS use causes the testicles to shrink by causing the Leydig cells to decrease natural testosterone production which then decreases the firmness and shape of the testicles which then results in a loss of size.
In one study of 772 gay men using 6 gyms between the months of January and February (and you need to think of the type of bias there that those people who are ‘Resolutioners’ would be more likely to go to the gym those months), a questionnaire was given to the men. 15 .2 percent of the men had used, with 11.7 percent of them injecting within the past 12 months. HIV positive men were more likely to have used in the past compared to negative men (probably due to scripts). Fifty-one percent of them reported testicular atrophy, and they were more likely to report suicidal thoughts (Bolding, Sherr, and Elford, 2002). They conclude:
One in seven gay men surveyed in central London gyms in 2000 said they had used steroids in the previous 12 months. HIV positive men were more likely to have used steroids than other men, some therapeutically. Side effects were reported widely and steroid use was associated with having had suicidal thoughts and feeling depressed, although cause and effect could not be established. Our findings suggest that steroid use among gay men may have serious consequences for both physical and mental health.
Of course, those who (ab)use substances have more psychological problems than those who do not. Another study of 203 bodybuilders found that 8 percent (n = 17) found testicular atrophy (for what it’s worth, it was an internet survey of drug utilization) (Perry et al, 2005). Another study found that out of 88 percent of individuals who abused the drug complained of side-effects of AAS use, about 40 percent described testicular atrophy (Evans, 1997), while testicular atrophy was noted in about 50 percent of cases (sample size n = 24) (Darke et al, 2016).
Sperm production
One study of steroid users found that only 17 percent of them had normal sperm levels (Torres-Calleja et al, 2001), this is because exogenous testosterone will result in the atrophy of germinal cells which cause a decrease in spermatogenesis. Though, too, increased AAS (ab)use later into life may lead to infertility later in life. Knuth et al (1989) also studied 41 bodybuilders with an average age of 26.7. They went through a huge laundry list of different types of steroids they have taken over their lives. Nineteen of the men were still using steroids at the time of the investigation (group I), whereas 12 of them (group II) stopped taking steroids 3 months prior, while 10 of them (group III) stopped steroid use 4 to 24 months prior.
They found that only 5 of them had sperm counts below the average of 20 million sperm per square ml, while 24 of the bodybuilders showed these symptoms. No difference between group I and II was noticed and group III (the group that abstained from use for 4 to 24 months) largely had sperm levels in the normal range. So, the data suggests that even in cases of severe decrease of sensitivity to androgens due to AAS (ab)use, spermatogenesis may still continue normally in some men, even when high levels of androgens are administered exogenously, while even after prolonged use it seems it is possible for sperm levels to go back to the normal range (Knuth et al 1989).
Aggression and crime
Now it’s time for the fun part and my reason for writing this article. Does (ab)using steroids cause someone to go into an uncontrollable rage, a la the Incredible Hulk when they inject themselves with testosterone? The media has latched into the mind of many, with films and TV shows showing the insanely aggressive man who has been (ab)using AAS. But how true is this? A few papers have shown that this phenomenon is indeed true (Konacher and Workman, 1989; Pope and Katz, 1994), but how true is it on its own, since AAS (ab)users are known to use multiple substances???
Konacher and Workman (1989) is a case study done on one man who had no criminal history, who began taking AASs three months before he murdered his wife, and they conclude that AAS can be said to be a ‘personality changer’. Piacetino et al (2015) conclude in their review of steroid use and psychopathology in athletes that “AAS use in athletes is associated with mood and anxiety disturbances, as well as reckless behavior, in some predisposed individuals, who are likely to develop various types of psychopathology after long-term exposure to these substances. There is a lack of studies investigating whether the preexistence of psychopathology is likely to induce AAS consumption, but the bulk of available data, combined with animal data, point to the development of specific psycho-pathology, increased aggressiveness, mood destabilization, eating behavior abnormalities, and psychosis after AAS abuse/dependence.” I, too, would add that since most steroid abuse are polysubstance abusers (they use multiple illicit drugs on top of AAS), that the steroids per se are not causing crime or aggressive behavior, it’s the other drugs that the steroid (ab)user is also taking. And there is evidence for this assertion.
Lundholm et al (2015) showed just that: that AAS (ab)use was confounded with other substances used while the individual in question was also taking AAS. They write:
“We found a strong association between self-reported lifetime AAS use and violent offending in a population-based sample of more than 10,000 men aged 20-47 years. However, the association decreased substantially and lost statistical significance after adjusting for other substance abuse. This supports the notion that AAS use in the general population occurs as a component of polysubstance abuse, but argues against its purported role as a primary risk factor for interpersonal violence. Further, adjusting for potential individual-level confounders initially attenuated the association, but did not contribute to any substantial change after controlling for polysubstance abuse.“
Even The National Institute of Health (NIH) writes: “In summary, the extent to which steroid abuse contributes to violence and behavioral disorders is unknown. As with the health complications of steroid abuse, the prevalence of extreme cases of violence and behavioral disorders seems to be low, but it may be underreported or underrecognized.” We don’t know whether steroids cause aggression or more aggressive athletes are more likely to use the substance (Freberg, 2009: 424). Clearly, the claims of steroids causing aggressive behavior and crime are overblown and there has yet to be a scientific consensus on the matter. A great documentary on the matter is Bigger, Stronger, Faster, which goes through the myths of testosterone while chronicling the use of illicit drugs in bodybuilding and powerlifting.
This, too, was even seen in one study where men were administered supraphysiologic doses of testosterone to see its effects on muscle size and strength since it had never been tested; no changes in mood or behavior occurred (Bhasin et al, 1996). Furthermore, injecting individuals with supraphysiological doses of testosterone as high as 200 and 600 mg per week does not cause heightened anger or aggression (Tricker et al, 1996; O’Connor et, 2002). Testosterone is one of the most abused AASs around, and if a heightened level of T doesn’t cause crime, nor can testosterone levels being higher this week compared to last seem to be a trigger for crime, we can safely disregard any claims of ‘roid rage’ since they coincide with other drug use (polysubstance abuse). So since we know that supraphysiologic doses of testosterone don’t cause crime nor aggression, we can say that AAS use, on its own (and even with other drugs) does not cause crime or heightened aggression since aggression elevates testosterone secretion, testosterone doesn’t elevate aggression.
One review also suggests that medical issues associated with AAS (ab)use are exaggerated to deter their use by athletes (Hoffman and Ratamess, 2006). They conclude that “Existing data suggest that in certain circumstances the medical risk associated with anabolic steroid use may have been somewhat exaggerated, possibly to dissuade use in athletes.”
Racial differences in steroid use
Irving et al (2002) found that 2.1 percent of whites used steroids, whereas 7.6 percent of blacks did; 6.1 percent of ‘Hispanics’ use them within the past 12 months, and a whopping 14.1 percent of Hmong Chinese used them; 7.9 percent of ‘other Asians’ used them, and 3,1 percent of ‘Native Americans’ did with 11.3 percent of mixed race people using them within the past 12 months to gain muscle. Middle schoolers were more likely to use than high schoolers, while people from lower SES brackets were more likely to use than people in higher SES brackets.
Stilger and Yesalis (1999: 134) write (emphasis mine):
Of the 873 high school football players participating in the study, 54 (6.3%) reported having used or currently using AAS. Caucasians represented 85% of all subjects in the survey. Nine percent were African-American while the remainder (6%) consisted of Hispanics, Asian, and other. Of the AAS users, 74% were Caucasian, 13% African American, 7% Hispanic, and 3% Asian, x2 (4,854 4) 4.203, p 4 .38. The study also indicated that minorities are twice as likely to use AAS as opposed to Caucasians. Cross tabulated results indicate that 11.2% of all minorities use/used AAS as opposed to 6.5% of all Caucasians (data not displayed).
One study even had whites and blacks reporting the same abuse of steroids in their sample (n = 10,850 ‘Caucasians’ and n = 1,883 black Americans), with blacks reporting, too, lower levels of other drug abuse (Green et al, 2001). Studies indeed find higher rates of drug use for white Americans than other ethnies, in college (McCabe et al, 2007). Black Americans also frequently underreport and lie about their drug use (Ledgerwood et al, 2008; Lu et al, 2001). Blacks are also more likely to go to the ER after abusing drugs than whites (Drug Abuse Warning Network, 2011). Bauman and Ennett (1994) also found that blacks underreport drug use whereas whites overreport.
So can we really believe the black athletes who state that they do not (ab)use AAS? No, we cannot. Blacks like about any and all drug use, so believing that they are being truthful about AAS (ab)use in this specific instance is not called for.
Conclusion
Like with all things you use and abuse, there are always side-effects. Though, the media furor one hears regarding AAS and testosterone (ab)use are largely blown out of proportion. The risks associated with AAS (ab)use are ‘transient’, and will subside after one discontinues using the drugs. Blacks seem to take more AAS than whites, even if they do lie about any and all drug use. (And other races, too, seem to use it at higher rates than whites.) Steroid use does not seem to be ‘bad’ if one knows what they’re doing and are under Doctor’s supervision, but even then, if you want to know the truth about AAS, then you need to watch the documentary Bigger, Stronger, Faster. I chalk this up to the media themselves demonizing testosterone itself, along with the ‘toxic masculinity’ and the ‘toxic jock effect‘ (Miller, 2009; Miller, 2011). Though, if you dig into the literature yourself you’ll see there is scant evidence for AAS and testosterone (ab)use causing crime, that doesn’t stop papers like those two by Miller talking about the effects of ‘toxic jocks’ and in effect, deriding masculine men and with it the hormone that makes Men men: testosterone. If taken safely, there is nothing wrong with AAS/testosterone use.
(Note: Doctor’s supervision only, etc)
