
Home » Vitamin D
Category Archives: Vitamin D
Vitamin D, Physiology, and the Cold
1200 words
I’ve been chronicling the VDH recently since it has great explanatory—and predictive—power. Light skin is a clear adaptation to low UVR, while dark skin is a clear adaptation to high UVR. Dark, highly melanized skin confers advantages in high UVR environments, such as protection against DNA damage, and also absorbs sufficient UV for vitamin D production while also protecting against folate depletion. However, when our ancestors migrated out of Africa, dark skin would not cut it in temperate environments with highly variable UV rays. This is where our highly adaptive physiology came into play, ensuring that we survived in highly variable environments. Light skin was important in low UVR environments in order to synthesize ample vitamin D, however, that synthesized vitamin D then conferred numerous other physiological advantages to the cold.
Eighty to ninety percent of the vitamin D required for humans comes from the sun, whereas ten to twenty percent comes from the diet, such as fatty fish, eggs, and dairy products (fortified with vitamin D, of course) (Ajabshir, Asif, and Nayer, 2014). Humans need to rely on high amounts of UV rays for vitamin D synthesis (Carlberg, 2014) other than Arctic peoples. Since dark skin does not synthesize vitamin D as well as light skin, skin gradually lightened as our ancestors migrated out of Africa (Juzeniene et al, 2009). This was then imperative to the physiologic adaptations that then occurred as our physiology had to adapt to novel, colder environments with fewer UV rays.
Sufficient amounts of vitamin D are highly important for the human musculoskeletal system (Wintermeyer et al, 2016), which is extremely important for birthing mothers. Along with the increased vitamin D synthesis in low UV environments, the heightened production of vitamin D conferred numerous other physiologic benefits which then helped humans adapt to colder environments with more varying UVR.
Vasoconstriction occurs when the blood vessels constrict which leads to heightened blood pressure, whereas vasodilation is the dilation of blood vessels which decreases blood pressure. So evolutionarily speaking, we had to have adaptive physiology in order to be able to “switch” back and forth between vasoconstriction and vasodilation, depending on what the current environment needed. Vasodilation, though, most likely had no advantage in high UV environments, and thus must have been an advantage in low UV environments, where it was more likely to be colder and so, when the blood vessels constrict, blood pressure increases and thus, heat loss could be considerably slowed in these environments due to these physiologic adaptations.
The races also differ, along with many other physiologic abilities, in nitric oxide-mediated vasodilation. Vasodilation is the dilation of blood vessels, which increases blood pressure. Mata-Greenwood and Chen (2008) reviewed the relevant literature regarding black/white differences in nitric oxide-dependent vasorelaxation and concluded that nitric oxide vasodilation is reduced in darker-skinned populations. Thus, we can infer that in lighter-skinned populations nitric oxide vasodilation is increased in lighter-skinned populations, which would have conferred a great physiological advantage when it came to colonizing environments with lower UV rays.
VDR and vitamin D metabolizing enzymes are present in adipose tissue. Tetrahydrobiopterin; which acts as a cofactor in the synthesis of nitric oxide and its primary function is as a vasodilator in the blood vessels (meaning that blood pressure is increased, to keep more heat in the cold) (Chalupsky and Cai, 2005). Since vasodilation is the body’s primary response to heat stress, blood flow increases which allows heat to leave the body. Therefore, the human body’s ability regarding vasodilation and vasoconstriction mechanisms were important in surviving areas with varying UVR.
One function of our adipose tissue is the storage of vitamin D, while vitamin D metabolizing enzymes and VDR are also expressed in the adipocyte (Abbas, 2017). With these known actions of vitamin D on adipose tissue, we can speculate that since vitamin D and the VDR are expressed in adipose tissue, it may have exerted a role in the adipose tissue which may have been important for surviving in cold, low UV environments (see below).
Furthermore, since these mechanisms are brought on by short-term changes, we can infer that it would hardly be of any use in high UVR environments and would be critical in temperate environments. So, vasodilation and vasoconstriction have little to no benefit in high UVR environments but seem to be imperative in temperate environments where UVR varies. It’s also likely that vitamin D influences vasodilation by influential nitric oxide synthesis (see Andrukhova et al, 2014) and vasoconstriction by influencing the renin-angiotensin system (Ajabshir, Asig, and Nayer, 2014).
This would have conferred great benefit to our ancestors as they migrated into more temperate and colder climates. You can read this for information on how adaptive our physiology is and why it’s like that. Because we went into numerous new environments and natural selection couldn’t act quickly enough, therefore the human body’s physiology is extremely adaptive.
What this suggests is that as skin lightened and adapted to low UV, the increased synthesis in vitamin D influenced vasodilation by a strong influence on nitric oxide synthase, along with vasoconstriction, implies that it would have been easier to survive in novel environments due to adaptive physiology and skin color, along with body fat reserves and the physiologic effects of vitamin D on adipose tissue. These physiologic adaptations would have been of no to little use in Africa. Thus, they must have been useful after we migrated out of Africa and experienced wildly varying environments—the whole reason why our physiology evolved (Richardson, 2017: chapter 5).
When the human body is exposed to cold, a few things occur: cutaneous vasoconstriction, shivering (Castellani and Young, 2016), “behavioral thermoregulation” (Young, Sawka, and Pandolf, 1996), while the human body can adapt physiologically to the cold (Young, 1994). The physiologic functions that vitamin D and folate in regard to vasodilation and vasoconstriction, there is a great chance that these effects were important in maintaining energy homeostasis in colder climates.
In sum, the evolution of light skin conferred a great survival advantage to our ancestors. This then upped the production of vitamin D synthesis in the body, which where then of utmost importance in regard to the adaptation of the human physiology to colder, lower-UV environments. Without our adaptive physiological systems, we would not have been able to leave Africa into novel environments. We need both behavioral thermoregulation as well as adaptive physiology to be able to survive in novel environments. Thus, the importance of skin lightening in our evolution becomes clearer:
As humans migrated out of Africa, lighter skin was needed to synthesize vitamin D. This was especially important to women, who needed higher amounts of vitamin D, in order to produce enough calcium for lactation and pregnancy—so the babe had enough calcium to grow its skeleton in the womb. With the uptake in vitamin D synthesis, this then allowed more adaptive physiologic changes that occurred due to the cold, and along with vasodilation and vasoconstriction, along with shivering and adapting behaviorally to the new environments, were our ancestors able to survive. Dark skin cannot synthesize vitamin D as well as light skin in low UV environments; this also can be seen with the lowered production of nitric oxide-dependent vasodilation in dark-skinned populations. Thus, vasoconstriction conferred no physiologic benefit in high UV environments, but almost certainly conferred a physiologic benefit in low UV environments.
Why Are Women Lighter than Men? Skin Color and Sexual Selection
1550 words
Skin color differences between the sexes are always discussed in terms of women being lighter than men, but never men being darker than women. This is seen in numerous animal studies (some reviewed by Rushton and Templer, 2012; read rebuttal here; also see Ducrest, Keller, and Roulin, 2008). Though, the colors that evolved on the animal’s fur due to whatever mate choices are irrelevant to the survival capabilities that the fur, feathers etc give to the organism in question. So, when we look at humans, we lost our protective body hair millions of years ago (Lieberman, 2015), and with that, we could then sweat. So since furlessness evolved in the lineage Homo, there was little flexibility in what could occur due to environmental pressures on skin color in Africa. It should be further noted that, as Nina Jablonski writes in her book Living Color: The Biological and Social Meaning of Skin Color (2012, pg 74)
No researchers, by the way, have explored the opposite possibility, that women deliberately selected darker men!
One hypothesis proposes that lighter skin in women first arose as a byproduct due to the actions of differing levels of hormones in the sexes—with men obviously having higher levels of testosterone, making them darker them women. So according to this hypothesis, light-skinned women evolved since men could tell high-quality from low-quality mates as well as measure hormonal status and childbearing potential, which was much easier to do with lighter- than darker-skinned women.
Another hypothesis put forth is that further from the equator, sexual competition between women would have increased for mates since mates were depleted, and so light skin evolved since men found it more beautiful. Thus, women living at higher latitudes were lighter than women living at lower latitudes because men had to go further to hunt which meant they were more likely to die which caused even greater competition between females, lightening their skin even more. And another, related, argument, proposed that light skin in women evolved due to a complex of childlike traits which includes a higher voice, smoother skin and childlike facial features, which then reduced male competition and aggressiveness. But women did not stay around waiting to be provisioned and they got out and gathered, and hunted sometimes, too.
Harris (2005) proposes that light skin evolved due to parental selection—mothers choosing the lightest daughters to survive, killing off the darker ones. All babies are born pale—or at least lacking the amount of pigment they have later in life. So how would parental—mostly maternal—selection have caused selection for lighter skin in girls as Harris (2005) proposes? It’d be a pretty large guessing game.
The role of sexual selection in regard to human skin color, though, has been tested and falsified. Madrigal and Kelly (2007a) tested the hypothesis that skin reflectance should be positively correlated with distance from the equator. It was proposed by other authors that as our ancestors migrated out of Africa, environmental selection relaxed and sexual selection took over. Their data did not lend credence to the hypothesis and falsified it.
Madrigal and Kelly (2007a: 475) write (emphasis mine):
We tested the hypothesis that human sexual dimorphism in skin color should be positively correlated with distance from the equator, a proposal generated by the sexual selection hypothesis. We found no support for that proposition. Before this paper was written, the sexual selection hypothesis was based on stated male preference data in a number of human groups. Here, we focused on the actual pattern of sexual dimorphism. We report that the distribution of human sexual dimorphism in relation to latitude is not that which is predicted by the sexual selection hypothesis. According to that hypothesis, in areas of low solar radiation, there should be greater sexual dimorphism, because sexual selection for lighter females is not counterbalanced by natural selection for dark skin. Our data analysis does not support this prediction.
Though Frost (2007) replied, stating that Madrigal and Kelly (2007a) presumed that sexual selection was equal in all areas. Madrigal and Kelly (2007b) responded, stating that they tested one specific hypothesis regarding sexual selection and found it to be false. Frost (2007) proposed two hypotheses in order to test his version, but, again, no one has proposed that women select darker men, which could be a cause of lighter-skinned women (though sexual selection does not—and cannot—explain the observed gradation in skin color between men and women).
Skin color differences between men and women first arose to ensure women enough calcium for lactation and pregnancies. Since skin pigmentation protects against UVR but also must generate vitamin D, it must be light or dark enough to ensure ample vitamin D production in that certain climate, along with protecting against the UVR in that climate. So women needed sufficient vitamin D, which meant they needed sufficient calcium to ensure a strong skeleton for the fetus, for breastfeeding and for the mother’s own overall health.
However, breastfeeding new babes is demanding on the mother’s body (calcium reserves are depleted four times quicker), and the calcium the babe needs to grow its skeleton comes directly from the mother’s bones. Even a mother deficient in vitamin D will still give calcium to the babe at the expense of her own health. But she then needs to increase her reserves of calcium in order to ensure future pregnancies aren’t fatal for her or her offspring.
Though, at the moment to the best of my knowledge, there are no studies on calcium absorption, vitamin D levels and the recovery of the female skeleton after breastfeeding. (Though n3 fatty acids are paramount as well, and so a mother must have sufficient fat stores; see Lassek and Gaulin, 2008.) Thus, light-skinned women are most likely at an advantage when it comes to vitamin D production: The lighter they are, the more vitamin D and calcium they can produce for more pregnancies. Since light skin synthesizes vitamin D more efficiently, the body could then synthesize and use calcium more efficiently. The body cannot use and absorb calcium unless vitamin D is present. Since the fetus takes calcium from the mother’s skeleton, ample amounts of vitamin D must be present. For ample amounts of vitamin D to be present, the skin must be light enough to ensure vitamin D synthesis which would be needed for calcium absorption (Cashman, 2007; Gallagher, Yalamanchili, and Smith, 2012; Aloia et al, 2013).
Nina Jablonski writes in her book (2012, 77):
Women who are chronically deficient in vitamin D because of successive pregnancies and periods of breastfeeding experience a form of bone degeneration called osteomalacia. This has serious consequences for infants born of later pregnancies and for mothers themselves, who are at greater risk of breaking bones. It makes sense that protection of female health during the reproductive years would be a top evolutionary priority, so we are now investigating whether, in fact, slightly lighter skin in women might be a fairly simple way of ensuring that women get enough vitamin D after pregnancy and breastfeeding to enable their bodies to recover quickly. The need for maintaining strong female skeletons through multiple pregnancies may have been the ultimate evolutionary reason for the origin of differences in skin color between men and women.
While Jablonski and Chaplin (2000: 78) write:
We suggest that lighter pigmentation in human females began as a trait directly tied to increased fitness and was subsequently reinforced and enhanced in many human populations by sexual selection.
It is obvious that skin color in women represents a complex balancing act between giving the body the ability to synthesize ample vitamin D and protect from UVR. Skin coloration in humans is very clearly highly adaptive to UVR, and so, with differing average levels of UVR in certain geographic locales, skin color would have evolved to accommodate the human body to whichever climate it found itself in—because human physiology is perhaps the ultimate adaptation.
Sexual selection for skin color played a secondary, not primary role (Jablonski, 2004: 609) in the evolution of skin color differences between men and women. There is a delicate balancing act between skin color, vitamin D synthesis, and UVR protection. Women need to produce enough vitamin D in order to ensure enough calcium and its absorption to the baby and then ensure there are ample amounts to replace what the baby took while in the womb in order for future pregnancies to be successful. Sexual selection cannot explain the observed gradation in skin color between the races and ethnies of the human race. In my opinion, the only explanation for the observed explanation is the fact that skin color evolved due to climatic demands, while independent justification exists for the hypothesis as a whole (Jablonski and Chaplin, 2010).
I don’t see any way that sexual selection can explain the observed gradation in skin color around the world. Skin color is very clearly an adaptation to climate, though of course, cultural customs could widen the skin color differences between the sexes, and make women lighter over time. Nevertheless, what explains the observed skin gradation is adaptation to climate to ensure vitamin D synthesis among a slew of other factors (Jones et al, 2018). Sexual selection, while it may explain small differences between the sexes, cannot explain the differences noted between the native human races.
The Vitamin D Receptor and the Updated VDH
2850 words
The relationship between vitamin D and the vitamin D receptor (VDR) has been found to be of recent importance in explaining the modulation of gene expression. The VDR helps us adapt to the climate, is epistatic with skin color genes, and so on. Due to the importance of the VDR, vitamin D, and another nutrient I’ve discussed in the past—folate—this drives the argument that the need to produce vitamin D was an important factor in the evolution of skin colors around the world as migrations out of Africa took place. It is also important to note that other competing hypotheses are not necessarily alternative hypotheses to the VDH (which is short for vitamin D-folate hypothesis), since there is significant overlap between them due to what we now know about the roles of vitamin D, folate (especially due to what we know now about how vitamin D, folate and the VDR regulate gene expression),the VDR, and skin color genes. Thus, the theories have been integrated and the updated hypothesis takes into account the other theories which has significant overlap with the VDH.
Jones et al (2018) is the most recent review of the VDH; in the review, they integrate new findings of folate, vitamin D, the VDR, and skin color genes with other supposedly competing hypotheses into a new and improved VDH model which will be discussed at the end of this article.
Vitamin D
Vitamin D is an important hormone (since it is a steroid, not a vitamin), which is the only one that is produced exogenously (from UV rays). Vitamin D is responsible for many physiologic functions including: regulating calcium levels by increasing calcium absorption, stimulates intestinal absorption of phosphate, stimulates osteoblasts which then produce receptor activator nuclear factor (RANKL) which then stimulates osteoclastogenesis which then activates osteoclasts for bone reabsorption (DeLuca, 2004). It has been further noted that around 5 percent of the human genome is under the influence of vitamin D (Jones et al, 2018).
Folate
Folate is an important water-soluble B vitamin. Since vitamin D and folate are linked by their sensitivities to UVR, then we must look at them independently and see what they do. In the case of folate, UVR causes folate degradation through the absorption of UVRs or, on the other hand, when folate oxidizes through free radicals after UVR exposure (Jones et al, 2018). So the hypothesis proposes that skin color in high UV areas evolved due to the need for protection of folate levels due to UVR degradation. On the other hand, depigmentation occurred in order for the body to produce adequate vitamin D in low UV areas.
Folate is needed to synthesize and repair DNA (Mahmood, 2014). Though common rebuttals to the VDH include supposed lack of evidence for the VDH, Jones et al (2018) write:
The potential impacts of a deficiency of these nutrients on natural selection is an ongoing debate and is a common argument raised against the vitamin D–folate hypothesis. However, these arguments often do not consider that the benefits of an adequate vitamin D and folate status on reproductive success extend far beyond their roles in maintaining reproductive health.
Vitamin D receptor
In recent years, it has been found that the VDR has had a profound influence on our adaptation to local climates our ancestors found themselves in after the trek out of Africa. Most cells and organs of the body have a vitamin D receptor (Wacker and Holick, 2013), so the importance of the VDR and certain genes involved in the production of skin color, vitamin D, and folate can be seen. Thus, evidence for the hypothesis would be differential expression of certain genes that are related to the VDR. Jones et al (2018) report on a few common VDR variants and ethnicity: FOK1 which has a lower frequency in African than European and East Asian populations, and Cdx2 which was highest in Africans and lowest in Europeans. Tiosano et al (2016) reported that multiple loci which are involved with the VDR gene display strong latitudinal clines, which is evidence for the hypothesis.
The VDR helps humans adapt to changes in UV radiation, it is “part of an evolutionary complex that adapts humans to changing UV radiation” (Hochberg and Templeton, 2010: 310). This is further corroborated by the fact that the VDR promoter and skin color genes are epistatic (Popsiech et al, 2014; Tiosano et al, 2016). Skin pigmentation levels, furthermore, determine plasma vitamin D levels and VDR autoregulation (Saccone, Asani, and Bornman, 2015).
The VDR works in concert with retinoic acid receptors (Schrader et al, 1993) which then bind to nucleotide base pairs called the vitamin D-responsive elements (VDRE) which then exert their effects on gene expression (Kato, 2000; Pike and Meyer, 2010; Janik et al, 2017).
Gene expression
Vitamin D elicits numerous functions on gene expression through the VDR, by binding elements of vitamin D to the target genes. Since the VDR works together with other receptors that bind to the VDRE, they can have strong effects on gene expression. Now, we know that vitamin D and folate are important for humans. We know that the VDR gene appears to be under strong selection, though only in the context of other genes (Tiosano et al, 2016). Thus, the VDR—along with folate and vitamin D—are extremely important for gene expression and the adaptation of the human body to differing climates.
Competing hypotheses
Skin barrier hypothesis
The skin barrier hypothesis (SBH) proposes that dark skin color arose to protect against environmental damage. This hypothesis is based on the fact that darker-pigmented peoples posess an enchanced barrier function in comparison to ligher-pigmented people, which is mainly due to the role of melanin in the scattering of UVR across the skin (Jones et al, 2018). Jones et al state that this hypothesis is “proposed as a discrete theory to the vitamin D-folate hypothesis“, but since both vitamin D and folate both have other responsibilities in the human body such as the development of skin structure, and the development of defense mechanisms that protect against UV radiation including heat and microbial stressors.
Folate may also have another important role in the human body: regulating the production, and stabilizing tetrahydrobiopterin. Melanin supports folate from UVR degradation, which then supports folate’s influence on melanin. But, as Jones et al write, tetrahydrobiopterin also acts as a cofactor in the synthesis of nitric oxide which is important in regard to vasoconstriction (blood vessel constriction). Vasoconstriction is related to increased heat flow since blood vessels are constricted, along with an increase in heart rate. As I have noted in the past, shivering revs the body’s metabolism in cold clmates in order to produce ample heat. Jones et al (2018) write:
From an evolutionary perspective, our ability to maintain vasodilation/vasoconstriction mechanisms would have been important in surviving varying UVR environments. As these mechanisms may been seen as relatively short-term responses to temperature changes, they are likely to be of greater importance in temperate UVR environments rather than environments of high UVR. This is supported by nitric oxide dependent vasodilation shown to be reduced in darkly skinned populations [59]. This suggests that vasodilation processes offer no advantage in extreme UVR environments but may be important in temperate UVR environments, where seasonal and daily temperature fluctuations are seen.
Thus, since there would be no advantage for this mechanism in equatorial climates, it must be for more colder, Arctic climates which further lends credence to the VDH. (Since vitamin D and folate play many roles in regard to human physiologic adaptation to climate, along with the VDR.)
Metabolic conservation hypothesis
This hypothesis proposes that our ancestors became depigmented after the migrations out of Africa since there was a need to draw energetic resources away from melanin production and move that energy that would have been for melanin production for other metabolic processes that a population would need in a colder environment. Thus, it is argued that the lighter skin of European and East Asian populations can be explained by the need energetic resources being moved away from pigmenting the skin to other, more important, metabolic processes that the ancestors of Europeans and East Asians experienced. But this hypothesis has numerous premises of the VDH, including the main premise: that human skin depigmented as we migrated into areas with fewer UV rays (Jones et al, 2018). Thus, vitamin D was extremely important in driving the effects of vasodilation/vasoconstriction.
Clearly, the role of vitamin D in the adipose tissue was important for human adaptation to colder climates. Since lighter skin can produce more vitamin D in low UV climates, this was another factor that helped when we left Africa: skin lightened for better vitamin D synthesis. Since vitamin D synthesis is related to gene expression and expression of about 5 percent of our genomes, the production of more vitamin D was beneficial. So depigmentation, while being primarily due to low UV radiation, can also be seen to allow for more efficient physiologic responses and adaptations to the newer, colder climates.
Skin mutagenesis hypothesis
The last competing theory is the skin mutagenesis hypothesis. This hypothesis proposes that skin pigmentation arose as a mechanism to protect against various skin cancers. The hypothesis is based on the fact that darker-pigmented individuals are at lower risk of developing skin cancers since their skin pigmentation can fight off UV radiation. Of course, knowing what we know about vitamin D and folate, these two agents would be involved regarding this hypothesis, since both agents have photoprotective effects. Vitamin D is extremely important to DNA repair (Graziano et al, 2016), as vitamin D reduces cell and DNA damage.
Though many authors dispute the claims of this hypothesis since the effects of skin cancer would occur after the reproductive years and would thusly not have an effect on natural selection for skin color. Though those who argue for the validity of the hypothesis propose that it would help in hunter-gatherer peoples whose old train their young their ways of life.
Since these interactions have between these variables have been verified at the molecular genetic level, this lends even more credence to the VDH. (The findings inclue the frequency of common VDR variants between different ethnic groups, to UVR and folate metabolism genes which were found to be significantly associated with the frequency of 16 common folate variants and skin pigmentation in a genomic analysis of 30,000 people which were novel relationships; Jones et al, 2018a). These findings discussed by Jones et al (2018b) “indicate the existence of interactions between UVR, skin type, and vitamin D and folate genes, and they provide supporting molecular evidence for the vitamin D–folate hypothesis.”
Sexual selection
Madrigal and Kelly (2007a) tested a sexual selection hypothesis proposed by a few proponents of the sexual selection hypithesis. Madrigal and Kelly (2007a) tested the hypothesis that skin color reflectance should be positively correlated with distance from the equator. They, however, showed that the pattern in skin color dimorphism seen around the globe was not consistent with the sexual selection hypothesis, and thus their data did not lend credence to the sexual selection hypothesis. The hypothesis states that in areas with low UV radiation, environmental selection for skin color should be relaxed and there should be a higher rate of sexual dimorphism in peoples from northerly climates due to sexual selection for lighter-skinned women. Nevertheless, the data compiled by Madrigal and Kelly (2007a) do not lend credence to the hypothesis.
Frost (2007) responded that Madrigal and Kelly (2007a) presumed that sexual selection was equal in all areas, but was constrained by natural selection for dark skin. Frost (2007) also states that sexual dimorphism in human skin color may not be able to be expressed in lighter-skinned populations at higher latitudes. Frost’s objections stem from the fact that Madrigal and Kelly tested a specific hypothesis proposed by proponents of the sexual selection hypothesis, though Madrigal and Kelly hope that Frost can test his hypotheses. However, I think it’s a moot issue. Sexual selection for women occurred after selection for light skin due to vitamin D synthesis which ensured more calcium for pregnancy and lactation.
Thusly, sexual selection for lighter skin would continue to ensure ample vitamins for women and their pregnancies and lactation to feed their babies. This would further be butressed by the fact that vitamin D exerts effects on the adipocites which lends even more credence to the claim that light skin evolved first for vitamin D synthesis. Vitamin D then exerted effects on the adipocite since more vitamin D could be produced in the absence of high levels of UV, which then aided in human physiologic adaptations to climate.
Integration of current skin color theories
As can be seen from the competing theories, they are not necessarily explaining different things, and each supposed competing theory has an aspect from the VDH in it. Thusly, it is possible to integrate the so-called competing theories into a larger explanatory framework.
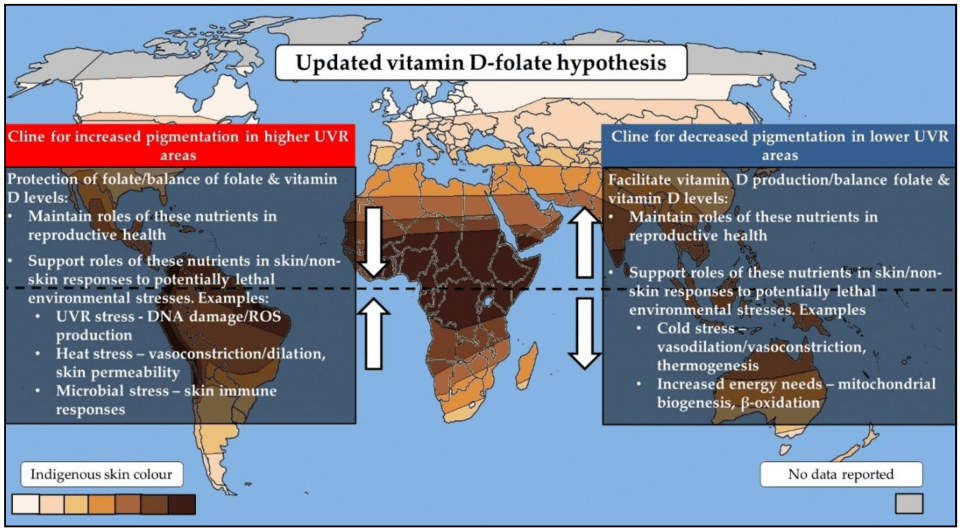
Jones et al (2018b) update the VDH by integrating the other theories into it, since they are similar and do not contradict the VDH (since aspects of each one can be used to explain different aspects of the VDH). The updated hypothesis is thus:
Vitamin D and folate have differing sensitivities to UVR. Vitamin D can be synthesized following UVR exposure, folate may be degraded. So the VDH proposes that the two differing skin colors (light and dark) evolved at differing latitudes as a “balancing mechanism” to maintain adequate levels of the two agents vitamin D and folate. Since adequate levels of vitamin D and folate were maintained, there would be no ill health effects after migrating into colder climates. Vitamin D and folate both act as photoprotectors of the skin and can decrease environmental stressors. Vitamin D also exerts important effects on adipocites—both types—which then further aid in human physiologic adaptations to the cold. Perhaps most importantly, the VDR and skin color genes are epistatic—the VDR is imperative in the human body’s adaptation to new climates.
The latest research (reviewed by Jones et al, 2018b) show strong support for the interaction between genes and folate/vitamin D processes with skin pigmentation and UVR.
Health Disparities
Health disparities due to vitamin D deficiency are well-noted in the literature. Human migrations over the recent centuries and decades have caused environmental mismatches between a population’s adapted skin type and current UV level in the location the population migrated to. Many darkly-pigmented people now live in areas with low UVR, and thusly suffer from health consequences. This leads to them either not having an adequate vitamin D-folate balance along with the risk of not having the adequate skin protections for a given environment, since UV rays influence folate and vitamin D production and so, a mismatched skin color to UV environment would cause problems for skin protection since the environment is not ancestral to that certain skin color.
As I have previously noted, it has been argued that blacks are not vitamin D deficient, and thusly not vitamin D deficient. Though, these claims rest on a slew of false arguments that have since been rebutted. It has been argued that since blacks are deficient in vitamin D, which begins in the womb, and vitamin D deficiencies cause changes in large and small arteries and arterials, that vitamin D deficiency could be the cause of higher rates of hypertension in black Americans (Rostand, 2010).
Conclusion
The role of vitamin D, folate, the VDR, and certain genes is under further invesitgation. This group of agents exert powerful effects on human physiology which then help with the adaptation of humans to differing climates. Folate and the vitamin D receptor play a crucial role in protecting the skin from environmental and microbial stressors. Vitamin D and the VDR are expressed in the adipose tissue, while vitamin D regulates adipogenesis and adipocite apoptosis (Abbas, 2017). Further evidence shows that there are multiple loci that are involved in the VDR that show latitudinal clines (Tiosano et al, 2016). One of the most things that lends credence to the VDH is the fact that the VDR and skin color genes are epistatic and help humans adapt to climates.
The VDH is in great shape, contrary to popular belief (Elias, Williams, and Bikle, 2016). The VDH is one of the only games in town to explain the skin color gradient noticed around the world, with vitamin D being the only agent that accounts for skin color differences. The VDH explains how and why human skin color is vastly different, and the main reason is adaptation to UV rays—or lack thereof.
Grant (2018) concludes that:
The UVB–vitamin D–cancer hypothesis has considerable supporting scientific evidence from a variety of study types: geographical ecological, observational, and laboratory studies of mechanisms, as well as several clinical trials.
Clearly, the VDH explains the incidence of the observed skin gradiation around the world the best out of the so-called competing hypotheses (which are similar enough to the VDH to where they can be absorbed into the VDH). Most importantly, the VDH predicted a novel fact—that molecular genetic evidence would show that light skin evolved independently numerous times in our lineage (Jablonksi and Chaplin, 2009).
Race and Vitamin D Deficiency
1600 words
Vitamin D is an important “vitamin” (it is really a steroid hormone). It is produced when the skin (the largest organ in the body) is exposed to the sun’s UVB rays (Nair and Maseeh, 2012). So this is one of the only ways to get natural levels of UVB. We can then think that, if a population is outside of its natural evolutionary habitat (the habitat where that skin color evolved), then we should note numerous problems caused by the lack of vitamin D in whichever population is studied outside of a location that doesn’t get the correct amount of UVB rays from the sun.
Black Americans are more likely than other ethnies to be deficient in vitamin D (Harris, 2006; Cosman et al, 2007; Nair, 2012; Forest and Stuhldreher, 2014; Taksler et al, 2014). But, paradoxically, low vitamin D levels don’t cause weaker bones in black Americans (O’Conner et al, 2014). However, like with all hypotheses, there are naysayers. For example. Powe et al (2013) argue that vitamin D tests misdiagnose blacks, that blacks have a form of the vitamin that cells can use called 25-hydroxyvitamin D. They conclude: “Community-dwelling black Americans, as compared with whites, had low levels of total 25-hydroxyvitamin D and vitamin D–binding protein, resulting in similar concentrations of estimated bioavailable 25-hydroxyvitamin D. Racial differences in the prevalence of common genetic polymorphisms provide a likely explanation for this observation.” Though there are a whole host of problems here.
The limitations of Powe et al (2013) striking: it was cross-sectional and observational (like most nutrition studies) so they were unable to predict effects of vitamin-D binding protein on bone fractures; no data on the consumption of vitamin D supplements; measurement of bone turnover markers, urinary calcium excretion and levels of 1,25-dihydroxyvitamin D may explain the effect of VDBP (vitamin D-binding protein) on mineral metabolism; and they relied on a calculation, rather than a measurement of 25-hydroxyvitamin D levels.
Powe et al’s (2013) findings, though, have been disputed. Using different measurement tools from Powe et al (2013), Henderson et al (2015) conclude that “Counter to prior observations by immunoassay, VDBG concentrations did not vary by race.” While Bouillon (2014) writes: In our view, black Americans, as compared with white Americans, have lower levels of not only total 25-hydroxyvitamin D but also free or bioavailable 25-hydroxyvitamin D.” And finally, Hollis and Bikle (2014) write: “Specifically, for any given physically measured level of bio-available 25-hydroxyvitamin D, the authors are overestimating bio-available 25-hydroxyvitamin D by 2 to 2.5 times owing to underestimation of vitamin D–binding protein in blacks.”
Either way, even if what Powe et al (2013) conclude is true, that would not mean that black Americans should not supplement with vitamin D, since many diseases and health problems are associated with low vitamin D intake in blacks, including osteoporosis, cardiovascular disease, cancer, diabetes, and other serious conditions (Harris, 2006). An indirect relationship between low levels of vitamin D and hypertension is also noted (Mehta and Agarwal, 2017). Since there is an indirect relationship between vitamin D levels and hypertension, then we should keep an eye on this because black Americans have some of the highest levels of hypertension in the world (Ferdinand and Armani, 2007; see also Fuchs, 2011).
Vitamin D is, of course, important for skeletal and nonskeletal health (Kennel et al, 2010). So if vitamin D is important for skeletal and nonskeletal health, we should see more diseases in black Americans that imply a lack of this steroid in the body. Although blacks have stronger bones even when deficient in vitamin D, it is still observed that black children who break their forearms have less vitamin D circulating in their blood (Ryan et al, 2011). This observation is borne out by the data, since black children are more likely to be deficient in vitamin D compared to other ethnies (Moore, Murphy, and Hollick, 2005). Since black skin predicts vitamin D deficiency (Thomas and Demay, 2000), it seems logical to give vitamin D supplements to children, especially black children, on the basis that it would help lower incidences of bone fractures, even though blacks have stronger bones than whites.
Furthermore, physiologically “normal” levels of vitamin D differ in blacks compared to whites (Wright et al, 2012). They showed that it is indeed a strong possibility that both whites and blacks have different levels of optimum vitamin D. Wright et al (2012) showed that there is a relationship between 25(OH)D levels and intact parathyroid hormone (iPth); for blacks, the threshold in which there was no change was 20 ng/ml whereas for whites it was 30 ng/ml which suggests that there are different levels of optimal vitamin D for each race, and the cause is due to skin color. Thus, physiologically “normal” levels of vitamin D differ for blacks and whites.
There is also a high prevalence of vitamin D deficiency/insufficiency and asthma in black inner-city youth in Washington DC (Freishtat et al, 2010). We can clearly see that, even though black Americans have stronger bones than white Americans and vitamin D predicts bone strength, the fact that blacks have stronger bones than whites even while being deficient in vitamin D on average does not mean that black Americans should not supplement with vitamin D, since it would ameliorate many other problems they have that are related to vitamin D deficiency.
There are also racial differences in prostate cancer (PCa) acquisition too, and vitamin D deficiency may also explain this disparity (Khan and Partin, 2004; Bhardwaj et al, 2017). I have heavily criticized the explanations that testosterone influences PCa, while having indicated that environmental factors such as diet and vitamin D deficiency may explain a large amount of the gap (Batai et al, 2017; but see Stranaland et al, 2017 for a contrary view). Since low vitamin D is related to prostate cancer, by supplementing with vitamin D, it is possible that levels of PCa may decrease. Kristal et al (2014) show that both high and low levels of vitamin D are associated with PCa.
Evidence also exists that vitamin D levels and hypertension are related. Rostand (2010) proposes a unified hypothesis: an important role exists in vitamin D deficiency and the pathogenesis and maintenance of hypertension in blacks (Rostand, 2010).
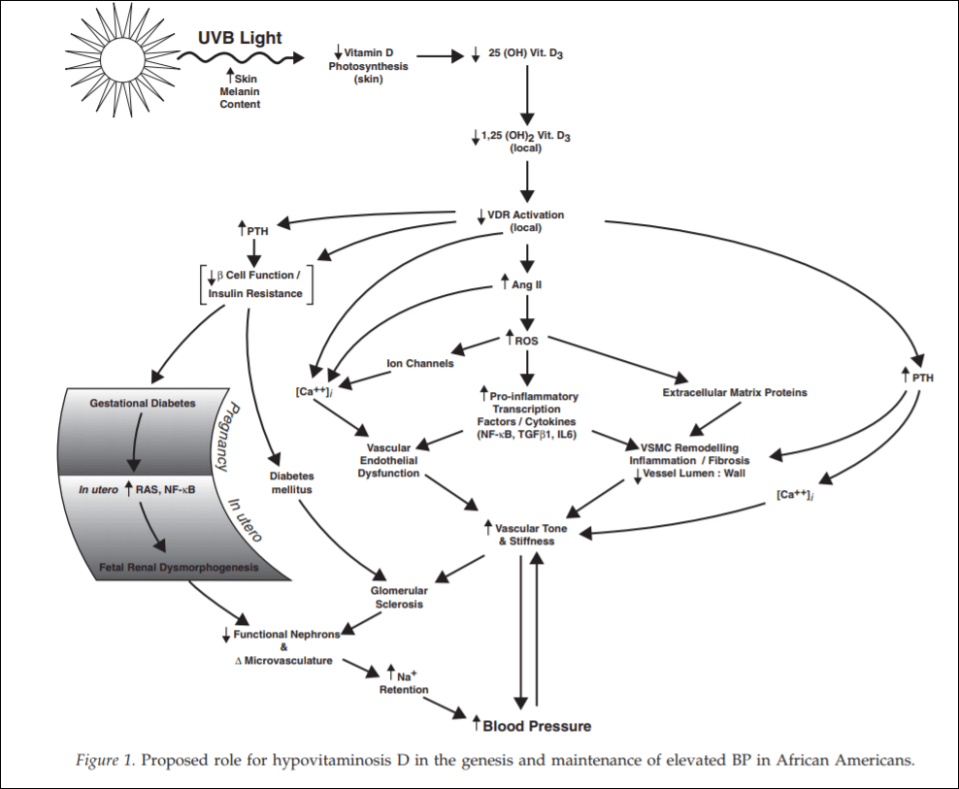
(From Rostand, 2010)
Since black Americans are no longer near the equator, their ability to synthesize vitamin D from UVB rays is diminished. This then probably leads the RAS (renin-angiotensin system) and inflammatory cytokine activation which then leads to vascular endothelial dysfunction along with structural changes to the microvasculature, which have been linked to vascular (arterial) stiffness along with increased vascular resistance, and these changes are shown to precede hypertension, which also occurs early in life. So since blacks are deficient in vitamin D, which even starts in the womb (Bodnar et al, 2007; Dawodu and Wagner, 2007; Lee et al, 2007; Khalessi et al, 2015; Seto et al, 2016), and this vitamin D deficiency most likely produces changes in large and small arteries and arterials, this could be the explanation for higher hypertension in black Americans (Rostand, 2010: 1701).
This would be a large environmental mismatch: since the population is displaced from its ancestral homeland, then this causes problems since it is not the environment where their ancestors evolved. So in this case, since black Americans are concentrated in the southeast corner of the United States, this may explain the high rates of vitamin D deficiency and hypertension in the black American community.
People whose ancestors evolved in locations with fewer UVB rays have lighter skin, whereas people whose ancestors evolved in locations with more UVB rays have darker skin. Thus, by placing populations in their opposite evolutionary environment, we can see how and why deleterious effects would occur in the population that is in the mismatched environment. For whites, skin cancer would occur, whereas for blacks, higher rates of hypertension and low birth weights occur.
Looking at levels of vitamin D deficiency in races is a great way to understand the evolution of certain populations. Because if the vitamin D hypothesis is correct, if skin color is an adaptation to UVB rays, with light skin being an adaptation to low UVB while dark skin is an adaptation to high UVB, then we can safely hypothesize about certain problems that would arise in races that are outside of their natural habitats. We have confirmed these hypotheses—black Americans who are outside of the location that their ancestors evolved in are more likely to have deleterious symptoms, and the symptoms are due to differences in vitamin D production, which come down to differences in skin color and how the skin synthesizes vitamin D in low-light environments.
Even though blacks have stronger bones than whites, this does not mean that they do not experience fractures at a high rate—especially children—and since the association was noticed, then by supplementing with vitamin D, this may lower the disparity of these types of injuries.
Since black Americans, compared to their evolutionary history, live in low-light environments, this then explains the how and why of vitamin D deficiency and why blacks need to supplement with vitamin D; no matter if certain studies show that blacks are ‘healthy’ even though they have low levels of vitamin D. If true (which I strongly doubt), that does not mean that black Americans should not supplement with vitamin D, because numerous other maladies are associated with vitamin D intake. This is one aspect where understanding the evolution of our species and the different races in it would lead to better medical care for individuals and ancestral groups that may need special treatment.
It is clear that race and geography should inform vitamin D intake, for if we do this, many diseases that arise can be ameliorated and quality of life can increase for everyone.
