
Home » Posts tagged 'Prostate Cancer'
Tag Archives: Prostate Cancer
Race and Vitamin D Deficiency
1600 words
Vitamin D is an important “vitamin” (it is really a steroid hormone). It is produced when the skin (the largest organ in the body) is exposed to the sun’s UVB rays (Nair and Maseeh, 2012). So this is one of the only ways to get natural levels of UVB. We can then think that, if a population is outside of its natural evolutionary habitat (the habitat where that skin color evolved), then we should note numerous problems caused by the lack of vitamin D in whichever population is studied outside of a location that doesn’t get the correct amount of UVB rays from the sun.
Black Americans are more likely than other ethnies to be deficient in vitamin D (Harris, 2006; Cosman et al, 2007; Nair, 2012; Forest and Stuhldreher, 2014; Taksler et al, 2014). But, paradoxically, low vitamin D levels don’t cause weaker bones in black Americans (O’Conner et al, 2014). However, like with all hypotheses, there are naysayers. For example. Powe et al (2013) argue that vitamin D tests misdiagnose blacks, that blacks have a form of the vitamin that cells can use called 25-hydroxyvitamin D. They conclude: “Community-dwelling black Americans, as compared with whites, had low levels of total 25-hydroxyvitamin D and vitamin D–binding protein, resulting in similar concentrations of estimated bioavailable 25-hydroxyvitamin D. Racial differences in the prevalence of common genetic polymorphisms provide a likely explanation for this observation.” Though there are a whole host of problems here.
The limitations of Powe et al (2013) striking: it was cross-sectional and observational (like most nutrition studies) so they were unable to predict effects of vitamin-D binding protein on bone fractures; no data on the consumption of vitamin D supplements; measurement of bone turnover markers, urinary calcium excretion and levels of 1,25-dihydroxyvitamin D may explain the effect of VDBP (vitamin D-binding protein) on mineral metabolism; and they relied on a calculation, rather than a measurement of 25-hydroxyvitamin D levels.
Powe et al’s (2013) findings, though, have been disputed. Using different measurement tools from Powe et al (2013), Henderson et al (2015) conclude that “Counter to prior observations by immunoassay, VDBG concentrations did not vary by race.” While Bouillon (2014) writes: In our view, black Americans, as compared with white Americans, have lower levels of not only total 25-hydroxyvitamin D but also free or bioavailable 25-hydroxyvitamin D.” And finally, Hollis and Bikle (2014) write: “Specifically, for any given physically measured level of bio-available 25-hydroxyvitamin D, the authors are overestimating bio-available 25-hydroxyvitamin D by 2 to 2.5 times owing to underestimation of vitamin D–binding protein in blacks.”
Either way, even if what Powe et al (2013) conclude is true, that would not mean that black Americans should not supplement with vitamin D, since many diseases and health problems are associated with low vitamin D intake in blacks, including osteoporosis, cardiovascular disease, cancer, diabetes, and other serious conditions (Harris, 2006). An indirect relationship between low levels of vitamin D and hypertension is also noted (Mehta and Agarwal, 2017). Since there is an indirect relationship between vitamin D levels and hypertension, then we should keep an eye on this because black Americans have some of the highest levels of hypertension in the world (Ferdinand and Armani, 2007; see also Fuchs, 2011).
Vitamin D is, of course, important for skeletal and nonskeletal health (Kennel et al, 2010). So if vitamin D is important for skeletal and nonskeletal health, we should see more diseases in black Americans that imply a lack of this steroid in the body. Although blacks have stronger bones even when deficient in vitamin D, it is still observed that black children who break their forearms have less vitamin D circulating in their blood (Ryan et al, 2011). This observation is borne out by the data, since black children are more likely to be deficient in vitamin D compared to other ethnies (Moore, Murphy, and Hollick, 2005). Since black skin predicts vitamin D deficiency (Thomas and Demay, 2000), it seems logical to give vitamin D supplements to children, especially black children, on the basis that it would help lower incidences of bone fractures, even though blacks have stronger bones than whites.
Furthermore, physiologically “normal” levels of vitamin D differ in blacks compared to whites (Wright et al, 2012). They showed that it is indeed a strong possibility that both whites and blacks have different levels of optimum vitamin D. Wright et al (2012) showed that there is a relationship between 25(OH)D levels and intact parathyroid hormone (iPth); for blacks, the threshold in which there was no change was 20 ng/ml whereas for whites it was 30 ng/ml which suggests that there are different levels of optimal vitamin D for each race, and the cause is due to skin color. Thus, physiologically “normal” levels of vitamin D differ for blacks and whites.
There is also a high prevalence of vitamin D deficiency/insufficiency and asthma in black inner-city youth in Washington DC (Freishtat et al, 2010). We can clearly see that, even though black Americans have stronger bones than white Americans and vitamin D predicts bone strength, the fact that blacks have stronger bones than whites even while being deficient in vitamin D on average does not mean that black Americans should not supplement with vitamin D, since it would ameliorate many other problems they have that are related to vitamin D deficiency.
There are also racial differences in prostate cancer (PCa) acquisition too, and vitamin D deficiency may also explain this disparity (Khan and Partin, 2004; Bhardwaj et al, 2017). I have heavily criticized the explanations that testosterone influences PCa, while having indicated that environmental factors such as diet and vitamin D deficiency may explain a large amount of the gap (Batai et al, 2017; but see Stranaland et al, 2017 for a contrary view). Since low vitamin D is related to prostate cancer, by supplementing with vitamin D, it is possible that levels of PCa may decrease. Kristal et al (2014) show that both high and low levels of vitamin D are associated with PCa.
Evidence also exists that vitamin D levels and hypertension are related. Rostand (2010) proposes a unified hypothesis: an important role exists in vitamin D deficiency and the pathogenesis and maintenance of hypertension in blacks (Rostand, 2010).
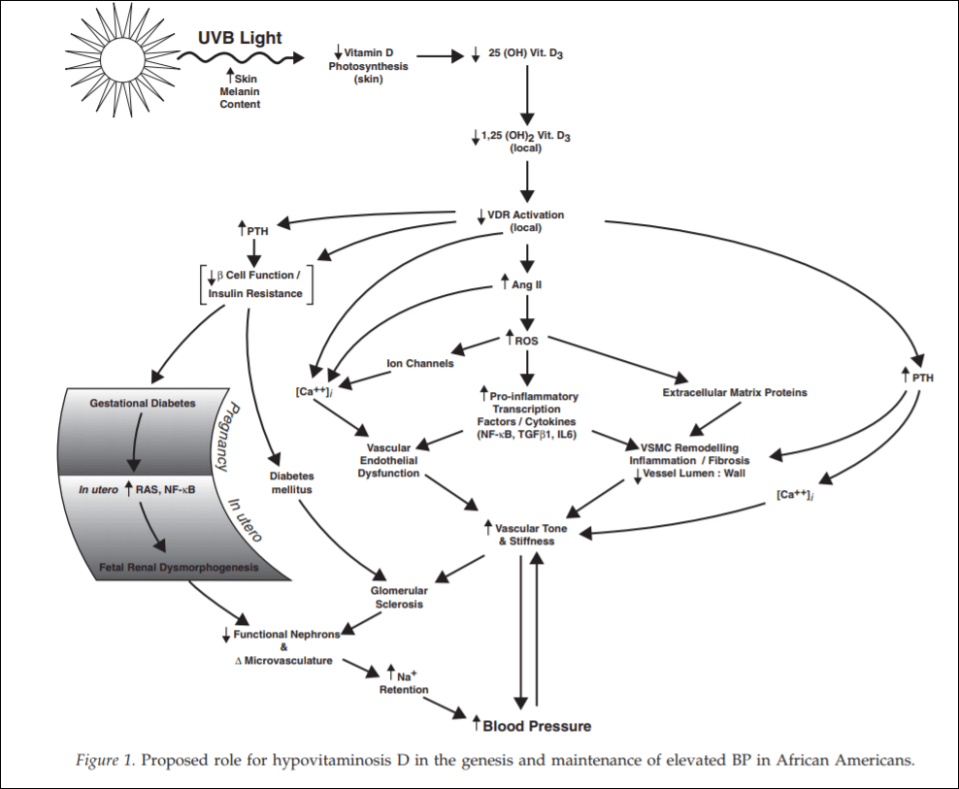
(From Rostand, 2010)
Since black Americans are no longer near the equator, their ability to synthesize vitamin D from UVB rays is diminished. This then probably leads the RAS (renin-angiotensin system) and inflammatory cytokine activation which then leads to vascular endothelial dysfunction along with structural changes to the microvasculature, which have been linked to vascular (arterial) stiffness along with increased vascular resistance, and these changes are shown to precede hypertension, which also occurs early in life. So since blacks are deficient in vitamin D, which even starts in the womb (Bodnar et al, 2007; Dawodu and Wagner, 2007; Lee et al, 2007; Khalessi et al, 2015; Seto et al, 2016), and this vitamin D deficiency most likely produces changes in large and small arteries and arterials, this could be the explanation for higher hypertension in black Americans (Rostand, 2010: 1701).
This would be a large environmental mismatch: since the population is displaced from its ancestral homeland, then this causes problems since it is not the environment where their ancestors evolved. So in this case, since black Americans are concentrated in the southeast corner of the United States, this may explain the high rates of vitamin D deficiency and hypertension in the black American community.
People whose ancestors evolved in locations with fewer UVB rays have lighter skin, whereas people whose ancestors evolved in locations with more UVB rays have darker skin. Thus, by placing populations in their opposite evolutionary environment, we can see how and why deleterious effects would occur in the population that is in the mismatched environment. For whites, skin cancer would occur, whereas for blacks, higher rates of hypertension and low birth weights occur.
Looking at levels of vitamin D deficiency in races is a great way to understand the evolution of certain populations. Because if the vitamin D hypothesis is correct, if skin color is an adaptation to UVB rays, with light skin being an adaptation to low UVB while dark skin is an adaptation to high UVB, then we can safely hypothesize about certain problems that would arise in races that are outside of their natural habitats. We have confirmed these hypotheses—black Americans who are outside of the location that their ancestors evolved in are more likely to have deleterious symptoms, and the symptoms are due to differences in vitamin D production, which come down to differences in skin color and how the skin synthesizes vitamin D in low-light environments.
Even though blacks have stronger bones than whites, this does not mean that they do not experience fractures at a high rate—especially children—and since the association was noticed, then by supplementing with vitamin D, this may lower the disparity of these types of injuries.
Since black Americans, compared to their evolutionary history, live in low-light environments, this then explains the how and why of vitamin D deficiency and why blacks need to supplement with vitamin D; no matter if certain studies show that blacks are ‘healthy’ even though they have low levels of vitamin D. If true (which I strongly doubt), that does not mean that black Americans should not supplement with vitamin D, because numerous other maladies are associated with vitamin D intake. This is one aspect where understanding the evolution of our species and the different races in it would lead to better medical care for individuals and ancestral groups that may need special treatment.
It is clear that race and geography should inform vitamin D intake, for if we do this, many diseases that arise can be ameliorated and quality of life can increase for everyone.
Racial Differences in Prostate Cancer: Part II
1050 words
I showed in part I, that the oft-cited reason for racial differences in prostate cancer acquisition and mortality are not due to higher levels of circulating testosterone when comparing blacks to whites (Richard et al, 2014). I posited (and provided sufficient evidence) that the disparity could come down to differences in vitamin D between the races. Black Americans are far removed from their ancestral environment, living in a cooler area. Their pigmentation reduces vitamin D production in the skin, since blacks need a lot more sunlight to synthesize the hormone than whites do, and the main culprit is the environment: not getting enough sunlight (Harris, 2006). I will provide further evidence for the theory.
The etiology of prostate cancer is not known (ACA, 2016; Bashir, 2015). The cause for the disparity in racial differences in prostate cancer may possibly come down to circulating vitamin D levels, with sunlight playing a large role in the variance. Racial differences in prostate cancer were larger in areas with less sunshine (Taksler et al, 2013). However, it is not known whether getting more sunlight (though the problem would still be getting enough in places with low levels of sunlight) or supplementing with vitamin D will help close the gap. Vitamin D is relevant for lethal prostate cancer (Shui et al 2012), whereas Li et al (2007) showed that supplementing with higher rates of vitamin D, especially during the winter months, may be particularly beneficial to men with low levels of circulating vitamin D. A study on veterans showed that men who had prostate cancer AND the lowest levels of vitamin D were more likely to die than veterans who had higher levels of the hormone (Der et al, 2014). Murphy et al (2014) showed in a biopsy, that in black Americans, low levels of vitamin D were associated with increased the odds of prostate cancer acquisition during the biopsy.
Black Americans are significantly more likely than European Americans to suffer from and die from prostate cancer (Hardiman et al, 2016). A difference of over 8,000 genes were found to be expressed differently. Blacks also have higher rates of prostate tumors and higher grade tumors than do European men. The racial disparity in prostate cancer mirrors circulating levels of vitamin D in the blood between the races (Nelson et 2016). Prostate cells become less sensitive to vitamin D through loss of receptors or signaling molecules “that mediate vitamin D’s actions, or through changes in metabolic enzymes that synthesize or degrade vitamin D compounds” (Peehl and Feldman, 2013). Hardiman et al (2016) showed that there were over 3,000 genes that differed between blacks and whites. Due to the fact that blacks are living outside of their ancestral climes, this is a large mediator of the prostate cancer gap. Vitamin D deficiency can also explain a large variation of the black-white prostate cancer gap (Grant and Peiris 2011).
Along with direct measurement of circulating vitamin D in the bloodstream, we also have correlates. Hypertension is correlated with prostate cancer: blacks have higher rates of hypertension; obesity further exacerbates the problem. Blacks males are more likely to be obese (though barely, which is where the other environmental factors come in). Men suffering from two or more health problems linked to metabolic syndrome are more likely to get prostate cancer. Blacks are more likely to get metabolic syndrome.
Clearly, a large portion of the variation in prostate cancer acquisition and mortality can be attributed to environmental factors (vitamin D intake specifically). We can also look to East Asia and their increasing rates of prostate cancer as well (Chen et al, 2014; Zhu et al, 2014). There are no genetic changes in the past ten years to account for this, so the only culprit is diet. Our Americanized diets have been making it to East Asia recently and it’s having a negative effect on them. China’s obesity rate is dramatically increasing, along with their rates of prostate cancer acquisition. It seems that the Western diet could also play a part in racial differences in prostate cancer acquisition.
To be fair the non-significance of this result might be attributable to the small number (only four) of African nations in the analysis. A number of previous studies have actually found that people of African descent on average do have shorter CAG repeats than other peoples (Ackerman et al., 2012; Esteban et al., 2005; Kittles et al., 2001; Lange et al., 2008). However, whether this actually indicates anything about the life history strategy of different populations remains questionable. The two other androgen indicators for which African data was available follow a completely different pattern. For androgenic hair, Caucasians have the highest rate, followed by Asians, then Africans. For prostate cancer, Caucasians have the highest rate, followed by Asians and Africans, who do not significantly differ.
The difference comes down, mostly in my opinion, due to diet. You can see this by looking at rates of prostate cancer in populations that have adopted, or are current adopting our Western diet.
There is a good chance that environmental factors explain a large part of the variance in prostate cancer acquisition and mortality. I, of course, do not deny intrinsic genetic explanations or other hormonal imbalances, however this is the best explanation I’ve come across. The fact that sunlight dictates prostate cancer acquisition is a huge tell and should be further researched.
I used to be a proponent of the testosterone theory, however, Richard et al (2014) shows a 2.5 to 4.9 percent difference in free testosterone between blacks and whites, which they conclude, does not explain the disparity between the races. Hormones do matter, and hormones can and do vary individually and by group, which are mediated by diet. Once we find out which foods either hurt or help prostate cancer growth, then we can have better treatments for this disease for men of all races.
There are numerous ways in which prostate cancer can be mitigated, with diet obviously playing a large factor (Son, Aronson, and Litwin, 2005; Lin, 2015; Nelson, Demarzo, and Yegnasubramanian, 2014). Future studies researching the racial disparities in prostate cancer should take into account UV radiation from the sun, circulating vitamin D in the blood, and diet amongst a myriad of other variables (these three just stand out to me). Moreover, large-scalre cohorts should be undertaken to see what effects diet can have on the mortality of those suffering from prostate cancer, as possibly supplementing vitamin D to attempt to fight the disease
Explaining the Black-White Prostate Cancer Gap
800 words
The black-white prostate cancer gap: genetic? Environmental? Both? Over the years, countless studies have been carried out—mostly on testosterone—to find the cause of the disparity between American blacks and whites. Numerous research has shown that black Americans’ test is substantially higher than white Americans (Ross et al, 1986; Winters et al, 2001; etc). However, studies with larger samples showed this was not the case. In a sample of 3,654 whites and 585 black Vietnam veterans shows there is a 3 percent difference favoring blacks (Ellis and Nyborg, 1992). The gold standard—a meta-analysis on 14 relevant studies (which I will discuss tonight) shows that the difference in (free) testosterone is nowhere near what Ross et al (1986) say, but was substantially lower at 2.5 to 4.9 percent (Richard et al, 2014). The meta-analysis, which was done due to the conflicting figures in each study showed that the gap in testosterone.
Obviously these people weren’t genotyped for racial ancestry, so the authors included studies that only included racial descriptors:
If races/ethnicities included in the study were referred to as ‘black’, ‘African-American’, ‘non-Hispanic black’, ‘white’, ‘non-Hispanic white’ or ‘Caucasian’. We did not include men of Hispanic or Asian origin.
Since we know that self-identified race is an almost perfect predictor of genetic ancestry, and the meta-analysis included studies that used the only the descriptors for race/ethnicity then the fact that this is done on American sample shows that testosterone is not as high as commonly thought in blacks when compared to whites (13 percent higher free testosterone).
In this sphere, one of the most common things said is that testosterone is one of the biggest causes of the black-white crime gap. High levels of testosterone ARE linked to higher crime rates, and blacks commit the most crimes, therefore blacks MUST have substantially higher levels of testosterone to account for the difference, right? Wrong. As I’ve shown above, Richard et al (2014) show that even after controlling for age, the difference in free testosterone was 2.5 to 4.9 percent. Black American males have an annual death rate from prostate cancer 2.4 times higher than whites (Taksler, Keating, and Cutler, 2012). If testosterone—one of the main possible culprits—does not explain the higher rate of prostate cancer mortality in American blacks in comparison to whites, what does?
Diet/environment and smaller genetic effects. People who have lower income cannot afford high-quality food, so they, therefore, have to buy low-quality, high carb, highly processed foods which lead to nutrient deficiencies. Drewnowski and Specter (2004) showed that 1) the highest rates of obesity are found in populations with the lowest incomes and education (correlated with IQ); 2) an inverse relationship between energy density and energy cost; 3) sweets and fats have higher energy density and are more palatable; and 4) poverty and food insecurity are associated with lower food expenditures, lower fruit and vegetable intake, and lower-quality diet. All of these data points show that those who are poor are more likely to be obese due to more energy-dense food being cheaper and fats and sugars being more palatable.
One important nutrient that people are often deficient in is vitamin D. Due to the name, people assume it’s a vitamin. It’s really not. It’s a steroid hormone. Vitamin D promotes calcium absorption, maintains normal calcium and phosphate levels, promotes bone and cell growth, and reduces imflamation. Black Americans have numerous ailments that are associated with low vitamin D intake.
Black Americans have a lower intake of vitamin D in comparison to white Americans. This is due to low dietary intake of vitamin D and less sun exposure. Dark skin pigmentation reduces vitamin D production in the skin, as dark skin requires more sunlight in order to produce vitamin D. Rickets is a common a common problem for blacks as when the mother is pregnant, she doesn’t get sufficient vitamin D so when the baby is born, it is deficient.
One variable that Dr. Joseph Mercola brings up is that black women don’t breastfeed as much as white women (though the gap is beginning to close a bit) causing rickets (as well as the lack of availability of vitamin D for the baby due to darker skin needing more sunlight to acquire adequate vitamin D).
Pretty much a great case for why race and geography should inform vitamin D intake. This is pivotal for our understanding for racial/ethnic differences in disease acquisition, why these differences occur and what can be done to prevent them.
Elevated levels of testosterone in black men comparison to white men are supposed to explain the higher rate of mortality in black men compared to white men. Except Richard et al (2014) showed that the testosterone gap wasn’t as high as previously thought (at 2.4 to 5.9 percent higher). The deficiency in vitamin D explains this phenomenon. Low vitamin D is linked to aggressive prostate cancer. This is the cause for the disparity, not higher rates of testosterone.
Are There Race Differences in Penis Size? Part II
1000 words
I haven’t completely discredited the notion that Rushton and Lynn may be correct on this variable, but I’m highly skeptical. Hormonal data doesn’t show it. Hormones like IGF-1 and androgen don’t show the differences between races that would lead you to believe that Rushton’s Rule applies here.
PP is at it again, citing the same studies, not providing primary sources, and not addressing what I say to him about hormones in regards to penis size. Hormones affect the body in different ways, and different races have different levels of hormones. This is what I will discuss today.
Insulin-like growth factor 1 (IGF-1) is a hormone that, as it’s name implies, is structurally similar to the hormone insulin. IGF-1 is “partly responsible for systemic GH activities although it possesses a wide number of own properties (anabolic, antioxidant, anti-inflammatory and cytoprotective actions).” Laron and Klinger (1998) showed that children with Laron syndrome who stopped receiving IGF-1 injections showed reductions in penile and testicular size and they returned to pretreatment serum levels. This shows the effects of IGF-1 on sexual organ size.
Knowing this about IGF-1, for Rushton’s theory to be plausible, Blacks would have higher levels, Asians the lowest, and whites in the middle, skewing towards Asians. Platz et al (1999) investigated whether there were racial differences in circulating IGF-1 and insulin-like growth factor-binding protein 3 (IGFBP-3). IGFBP-3 binds IGF-1 and 2, with a dysregulation of IGFBP-3 correlating with cancer. IGFBP-3 is the main transporter of IGF-1 and 2 in the blood stream. The researchers tested men whose self-described ancestry (we know that self-describer ancestry is a great proxy for race, having a 99.86 percent success rate) African American (63) a random sample of Asians and Caucasians (75 respectively) aged 45 to 78 years old. Caucasians had the highest levels of IGF-1 (224 ng/ml), Asians (208 ng/ml), and African Americans (205 ng/ml). The IGF-1:IGFBP-3 ratio was greatest in Caucasians and lowest in Asians. This study was carried out to see if IGF-1 had an effect on prostate cancer. The 13 percent difference in IGFBP-3 between blacks and whites may account for the higher levels of prostate cancer, as IGFBP-3 can control IGF-1 bioavailabilty.
PP also cites Ross et al (1986) showing that blacks have “19 percent higher testosterone”, attempting to use this as evidence for the theory in favor of an inverse relationship between brain size and penis size. He seems to think that total testosterone matters, when what matters is free testosterone.It’s also 15 percent circulating testosterone, 13 percent free testosterone in that one study. Free testosterone is biologically active, and is able to exert its effect by passing through a cell and activating its receptor. Speaking of free testosterone, in this meta-analysis of 23 studies on black-white differences in testosterone, Richard et al (2014) showed a 2.5 to 4.9 percent difference in free testosterone and concluded that that difference was not enough to account for the racial disparity in prostate cancer. So it’s either black Americans have lower levels of IGFBP-3 or diet/environmental factors that cause this racial disparity in prostate cancer, not testosterone.
Rohrmann et al (2007) showed that testosterone differences between blacks (n=363) and whites (n=674) did not noticeably differ (5.29 ng/ml and 5.11 ng/ml respectively). Mexican Americans (n=376) , on the other hand, showed a higher average rate (5.48 ng/ml) over both cohorts. Blacks had higher levels of estradiol than whites (40.80 pg/nl and 35.46 pg/nl respectively). Blacks also had a higher level of sex hormone-binding globulin (SHGB) (36.49 nmol/liter) than whites (34.91 nmol/liter) and Mexican Americans (34.91 nmol/liter). That may account for some of the racial disparity in prostate cancer, but it’s not testosterone (which shows that ‘higher levels of testosterone’ as PP says, isn’t proof of any racial differences in penis size).
The Kinsey data is nonrepresentative and nonrandom. We have comparative sizes for certain ethnies, and the only statistical difference is between Nigerians and Koreans and Czechs. Rushton and Boegart didn’t mention that blacks danced less than white college students, blacks are more prudish regarding nudity, more likely to have a prostitute as a sexual partner and less likely to want large families (Weizmann et al, 1990). A study on certain CAG repeats shows that Africans cluster with East Asians on two measures, contradicting Lynn’s hypothesis. French Army Surgeon, lol (see Weizman et al 1990 from above):
This work is filled with internal contradictions. For example, an average African Negro penis is said to be 7 3/4 to 8 inches long on p. 56, while on p. 242 it is stated that it “generally exceeds” 9 inches. Similarly, while the French Army surgeon announces on p. 56 that he once discovered a 12-inch penis, an organ of that size becomes “far from rare” on p. 243. As one might presume from such a work, there is no indication of the statistical procedures used to compute averages, what terms such as “often” mean, how subjects were selected, how measurements were made, what the sample sizes were, etc.
I think I’ve shown that there are no “””racial””” differences in size with the Veale et al 2014 study and the Orakwe and Ebuh (2007) study. As far as I see, two statistical differences exist between Nigerians and Koreans and Czechs. But there’s not enough “””quality data””” to say “this race bigger than that race”. To believe there are racial differences in penis size or that there is even an inverse relationship between penis size and brain size takes a huge leap of faith to believe.
There are, without a doubt, average differences in a lot of things between races; hormones being one of them. Any differences between races in IGF-1 have no effect on penis size (IGF-1 is, however, one reason why black girls reach menarche at a younger age than white girls. Will write more on that in the future.). Africans were more similar to Asians that Caucasians on two of the five androgen indicators that Dutton (2015) tested. The Kinsey data is nonrepresentative and nonrandom and that is what PP continuously references. I’m highly skeptical leading towards no based on my knowledge of hormones and how they work in the human body. Testosterone does not explain any racial differences in penis size, and does not explain any differences in prostate cancer acquisition (though, other hormones do).
