
Explaining African Running Success Through a Systems View
2100 words
Last year I bought The Genius in All of Us: New Insights Into Genetics, Talent, and IQ (Shenk, 2010) and while the book is interesting and I agree with a few things he says, he gets it horribly wrong on athleticism and ethnicity. Some of it I may be able to forgive since the book was written in 2010, but he does make some glaring errors. Chapter 6—pages 100-111—is titled Can White Men Jump? Ethnicity, Genes, Culture, and Success.
In the beginning of the chapter, Shenk writes that after the 2008 Beijing Summer Olympics, many articles were written about the Jamaican women who took the top three spots in the 100 and 200m races, with the emergence of Usain Bolt and his record-setting performance. Shenk (2010: 101) writes:
The powerful protein [alpha-actinin-3] is produced by a special gene variant called ACTN3, at least one copy of which is found in 98 percent of Jamaicans—far higher than in many other ethnic populations.
An impressive fact, but no one stopped to do the math. Eighty percent of Americans also had at least one copy of ACTN3—that amounts to 240 million people. Eighty-two percent of Europeans have it as well—that tacks on another 597 million potential sprinters. “There’s simply no clear relationship between the frequency of this variant in a population and its capacity to produce sprinting superstars,” concluded geneticist Daniel MacArthur.
I have written about MacArthur’s thoughts on the ACTN3 variant—that he helped discover, no less—in an article on Jamaicans, Kenyans, and Ethiopians and the explanatory factors in regard to their success in running competitions. Though, the article from MacArthur was written in 2008 and Shenk’s book was written in 2010, considerable advances have been made in this field. It was found that “combined effects of morphological and contractile properties of individual fast muscle fibers attribute to the enhanced performance observed in RR genotypes during explosive contractions” (Broos et al, 2016). Of course when talking about sprinting and morphology, you must think of the somatype. The somatype that is conducive to running success is a tall, lanky body with long limbs, as longer limbs can cover more distance. So European runners don’t have the right somatype, nor are the XX genotype for the ACTN3 variant high in Jamaicans (this genotype is present in ~2 percent of the Jamaican population; Scott et al, 2010). This—among other reasons I have laid out in the past—are why Jamaicans excel in sprinting competitions compared to other ethnic groups.
Shenk (2014: 10) further writes that sports success seem to come in ‘geographic clusters’, and the field of sports geography has been developed to understand it. “What they’ve discovered is that there’s never a single cause for a single cluster,” Shenk writes. “Rather, the success comes from many contributions of climate, media, demographics, politics, training, spirituality, education, economics and folklore. In short, athletic clusters are not genetic, but systemic.” Shenk then discusses the fact that these explanations are not good enough and that some ‘sports geographers’ have transformed themselves into ‘sports geneticists’ and then cites Jon Entine’s 2002 book Taboo: Why Black Athletes Dominate Sports and Why We’re Afraid to Talk About It where Shenk quotes Entine who quotes geneticist and physiologist Claude Bouchard who says that “these biological characteristics are not unique to West or East African blacks. These populations are seen in all populations, including whites” (Shenk, 2010: 102). Of course they’re not unique to one population and I don’t think that anyone has ever claimed that. Though the frequencies of these biological, morphological and physiological characteristics are not distributed evenly amongst populations and this explains how and why certain populations excel in certain sports when compared to others.
Shenk (2010: 102) also quotes Entine (2002), writing: “Entine also acknowledges that we haven’t actually found the actual genes he’s alluding to. “These genes will likely be identified early in the [twenty-first century],” he predicts.” We have ‘found some genes’ that aid in athletic performance, the ACTN3 genotype combined with type II fibers and the right morphology, as mentioned above for one. (Though a systems view—one of holism—makes much more sense here than a reducionist view. You must look at the whole system, not reduce things down, but that’s for another day.) That, in my opnion, is a large driver for ethnic differences in sports like this, because you need certain traits if you want to excel in these types of competitions.
He then discusses the success of the Kenyans in distance running—stating that 90 percent of Kenyan runners come from a small subset of Kenyans called the Kalenjin. He cites a few stories of some Kalenjin who talk about their experiences with no running water in their homes and that they had to “run to the river, to take your shower, run home, change, [run] to school . . . Everything is running” (Keino, a Kalenjin boy, quoted from Shenk, 2010: 104). Of course this is attributed to a multitude of factors, all of which have to work in concert to get the desired effect. For instance, sports psychologists have found that strong cultural achievement and the ability to work hard, compete, outdo others and seek new challenges drives their running dominance.
Shenk (2010: 106-107) then writes:
1.DESPITE APPEARANCES TO THE CONTRARY, RACIAL AND ETHNIC GROUPS ARE NOT GENETICALLY DISCRETE.
Skin color is a great deceiver; actual genetic differences between ethnic and geographic groups are very, very limited. All human beings are descended from the same African ancestors … [blah blah blah] … By no stretch of the imagination, then, does any ethnicity or region have an exclusive lock on a particular body type or secret high-performance gene. Body shapes, muscle fiber types, etc., are actually quite varied and scattered, and true athletic potential is widespread and plentiful.
Of course, I don’t think I have ever read anyone who denies this. However, as I’ve noted too many times to count, certain body types and muscle fiber distributions are more likely to be found in certain populations due to where their ancestors evolved recently, and so the fact that ‘actual genetic differences between ethnic and geographic groups are very, very, limited’ does not mean much when talking about dominance by a few populations in elite sporting competition. It just so happens to be the case that the somatypes and muscle fiber distributions that are conducive to running success are more likely to be found in populations of West and East African descent. This is an undeniable fact. (Also note how these ‘appearances to the contrary’ show how race is real.)
2.GENES DON’T DIRECTLY CAUSE TRAITS; THEY ONLY INFLUENCE THE SYSTEM.
Consistent with other lessons of GxE [Genes x Environment], the surprising finding of the $3 billion Human Genome Project is that only in rare instances do specific gene variants directly cause specific traits or diseases. …
As the search for athletic genes continues, therefore, the overwhelming evidence suggests that researchers will instead locate genes prone to certain types of interactions: gene variant A in combination with gene variant B, provoked into expression by X amount of training + Y altitude + Z will to win + a hundred other life variables (coaching, injuries, etc.), will produce some specific result R. What this means, of course, What this means, of course, is that we need to dispense rhetorically with thick firewall between biology (nature) and training (nurture). The reality of GxE assures that each persons genes interacts with his climate, altitude, culture, meals, language, customs and spirituality—everything—to produce unique lifestyle trajectories. Genes play a critical role, but as dynamic instruments, not a fixed blueprint. A seven- or fourteen- or twenty-eight-year-old is not that way merely because of genetic instruction. (Shenk, 2010: 107)
Nothing really wrong here. He is correct, which is why you need to look at the whole biological system, which also includes the culture, climate, environment and so on that the biological, developmental system finds itself in. However, Shenk then gets it wrong again writing that Jamaicans are a ‘quite heterogenous genetic group’ due to being a transport between North and South America. He states—correctly—that Jamaicans ancestry is about equal to that of African-Americans, but the individual variation in ancestry varies by “46.8 to 97.0 percent” (Shenk, 2010: 108).
Shenk gets a lot wrong here. For example. African-American and Jamaicans—despite both being descended from slave populations—have differing maternal ancestry which somehow influences athletic success. Deason (2017) found that 1) modern Jamaicans are descended from slaves and, who had considerable selective pressure on the population; 2) maternal ancestry could either influence sports success or be a false positive; 3) maternal lineages were different in Jamaicans and African-Americans, implying that the same maternal lineage is not distributed evenly between both sprinting populations; 4) some evidence exists that the genetic histories of Jamaicans and African-Americans are different based on their maternal haplotypes; 5) low SES and low access to healthcare—classic indicators of high African ancestry—were not directly linked to elite athletic success; 6) comparisons of the genomes of African-Americans and Jamaicans did not significantly differ since the estimated number of generations since admixture occurred, which implies that controls were not more likely to have more recent European ancestry than athletes; and 7) the regions of the genome that influence sprinting performance may be different in both populations. This is the best evidence to date against Shenk’s simplistic notions of the genetics between Jamaicans and African-Americans.
Differences in fast twitch fibers between Europeans and West Africans explain a large amount of the variance between Europeans and West African descendants in regard to sprinting success, while those with more symmetrical knees and ankles tend to run faster in the 100m dash (Trivers et al, 2014). This would also imply that Jamaicans have more symmetry in their knees and ankles than Europeans, though I am not aware of data that makes this comparison.
Shenk finally discusses the psycho-social-cultural aspects behind the phenomenon, stating that Roger Bannister, the first person to break the four minute mile, stated that while “biology sets limits to performance, it is the mind that plainly determines how close individuals come to those absolute limits” (Shenk, 2010: 110-111). Numerous psychological factors do, indeed, need to combine in order for the individual in question to excel in sports—along with the requisite anatomical/physiological/morphological traits too. Sasaki and Sekiya note that “changes in physiological arousal and movement velocuty induced by mild psychological pressure played a significant role in the sprint performance.” (See also Bali, 2015.)
Lippi, Favaloro, and Guidi, (2008) note how “An advantageous physical genotype is not enough to build a top-class athlete, a champion capable of breaking Olympic records, if endurance elite performances (maximal rate of oxygen uptake, economy of movement, lactate/ventilatory threshold and, potentially, oxygen uptake kinetics) (Williams & Folland, 2008) are not supported by a strong mental background.” I have argued this for months, even if the beneficial somatype is there in the athlete in question, if he/she does not have the will to win they will not succeed in their goals. Psychosocial factors, of course, matter just as much as the physical but all of these factors work in concert to get the outcomes that occur in these sports.
Attempting to pinpoint one or a few traits—while it may help us to understand better physilogic and anatomic processes—tells us nothing about the entire system. This is why, for instance, the whole athletes system needs to be looked at—call it the ‘systems view of the athlete’, where all of these aforementioned variables work in concert to express elite athletic performance, with no one variable being higher than another as an explanatory factor in sports success. Though Shenk gets a few things right (like his point on genes not causing traits on their own, they just influence the system, and I’d take it a step further to note that genes are passive in their relationship to the physiological system as a whole and are only activated by the system as needed, not being ’causes’ on their own; Noble, 2008), he’s largely misguided on how certain aspects of Jamaican ancestry and morphology help propel them to running success in comparison to other ethnies.
When explaining elite athletic performance in certain areas of sports, you must take a view of the whole system, with each known variable influencing the next in the chain, if you want to explain why certain ethnies or racial groups do better in a given sport than other groups. A systems view is the only view to take when comparing populations in different athletic competitions. So the influence of culture, psychology, social effects, morphology, ancestry, anatomy, physiology, muscle fibers, etc all work in concert to produce elite athletic phenotypes that then excel in these sports, and reducing this down to certain variables—while it may help us understand some of the inner mechanics—it does nothing to help advance the hows and whys of elite success in sports competition when comparing different populations.
Malaria, the Sickle Cell Trait, and Fast Twitch Muscle Fibers
2550 words
West Africans and their descendants have longer limbs and a shorter trunk than Europeans, on average—as I have extensively noted. Due to where they evolved, of course, they have a different morphology and physiology. Bergmann’s rule states that peoples with recent ancestry in the tropics will have slimmer pelvic bones and be narrower overall whereas Allen’s rule states that peoples with recent ancestry in the tropics will have long limbs, these traits being good for heat dissipation (Lieberman, 2015) and is one reason why West Africans and their descendants excel in these most sports in America.
The fact that a lot of African ethnic groups have different anatomic proportions and physiologic adaptations in comparison to people who have evolved in non-tropical climates is not contested. Morrison and Cooper’s (2006) hypothesis on sick cell anemia driving elite athletic performance in West Africans and their descendants is one of the most interesting explanations I’ve heard on the biochemical differences between the races. Sickle cell anemia is caused by a gene mutation. On amino acid 6, a single nucleotide substitution from A to T (As pair it Ts, Gs pair with Cs). This substitution changes a glutamic acid codon to valine codon which then causes sickling of the blood. Sickle cell anemia, of course, is not a ‘black disease’ as is popularly believed, but it, in fact, has to do with geography and the prevalence of malaria-carrying mosquitoes in that location. “This mutation“, Morrison and Cooper (2006) write “appears to have triggered a series of physiological adjustments, which have had favourable athletic consequences.”
Now, I’m aware that those who are already skeptical of this hypothesis may say ‘so does this mean that Italians, Greeks, MENA peoples etc have more type II fibers and would excel in these competitions?’, no it does not mean that because they don’t have the requisite morphology that West Africans have.
In the 1970s, a study was carried out on the physiological and anatomical proportions of Olympic athletes who competed in the 1968 Olympic games. Anatomic and physiologic measures were taken for each athlete. They used four racial classifications: Negroid, Caucasoid, Mongoloid, and mestizo (Indian/Spanish mix). The classifications were based on “were based on identification and somatotype photographs, as well as physical characteristics including skin color; general body shape; proportions of segments of the limbs; facial structure; form of eyes, lips, and nose; and colour and texture of hair” (Morrison and Cooper, 2006). This study, of course, also confirmed the anatomic differences between blacks and other races and how it leads to superior sports performance. Though, something peculiar was noted in the black athletes. Morrison and Cooper (2006) write: “Although the study failed to link athletic capability to a single gene system, the authors expressed “surprise” that “a sizeable number of Negroid Olympic athletes manifested the sickle-cell trait.””
One interesting study looked at the sickle cell trait (SCT) in French West Indian elite sprint athletes (Marlin et al, 2005). Using the French National Team for the year 2000, Marlin et al (2005) identified 3 sprinters (2 males and 1 female) who tested positive for the SCT. They also noticed a significantly higher presence of titles for people who tested positive for the SCT (38.6 percent for males and 50 percent for females. Marlin et al (2005: 624) conclude “that male SCT carriers are able to perform sprints and brief exercises at the highest levels” and “that brief and intensive exercise performance involving mainly alactic anaerobic metabolism may be enhanced by HbS in elite male sprinters.”
Blacks had narrower hips, longer arms and legs and a shorter trunk in comparison to other races. Of course, somatype is the variable that matters here but certain races are more likely to have certain anatomic characters that lead to superior spots performance on comparison to other races. The authors also attempted to link traits with single gene networks but were unsuccessful. However, they did notice that a large number of black athletes tested positive for the sickle cell trait. There is a conundrum here, however. People with the sickle cell gene might have a greater oxygen demand which causes more in vivo cell sickling. It was hypothesized that these individuals would be at a disadvantage since the 1968 Olympic games were held in Mexico city which is a high altitude area. They theorized that their blood would sickle more at the high altitude in comparison to low altitude but this was not seen.
Then another study was carried out which showed that not only do individuals with the sickle cell trait have lower hemoglobin levels, but all blacks do (Garn, Smith, and Clark, 1975). This is how and why they can perform at high altitudes despite having the sickle cell trait. Then, to test if this was mostly ‘environmental’ or ‘genetic’ they undertook a large study where they followed individuals throughout their whole lives and the difference persisted even later in life. Of course, according to other authors, some sort of compensatory mechanism should exist to counteract black’s lower hemoglobin levels, since this deficiency even exists in athletes (Morrison and Cooper, 2006).
As I’ve written about in the past, it was established that type I and type II fibers use different metabolic pathways and that type II fibers lead to improved athletic performance (along with the certain genotype for the ACTN3 gene). Morrison and Cooper (2006) also state that, of course, not all West Africans and descendants have this trait, and that these people came from a small area of West Africa.
A study looking at pulmonary differences between blacks and whites was conducted which found that blacks compensated for smaller lungs by breathing harder than whites while engaged in physical activity. In a study of 80 Asians and Europeans, Korotzer, Ong, and Hansen (2000) also showed that Asians had lower pulmonary functioning than Europeans. Even differences in chest size has been purported to explain differences in lung functioning, though this relationship did not hold (Whittaker, Sutton, and Beardsmore, 2005). Though, in his short review on race and the history of lung functioning, Braun (2015) writes that “At the very least, the idea that people labelled ‘white’ naturally have higher lung capacity than other races throughout the world should be approached with some skepticism.” because “Most commercially available spirometers internationally ‘correct’ or ‘adjust’ for race in one of two ways: by using a scaling factor for all people not considered to be ‘white’; or by applying population-specific norms. To enable the spirometer, the operator must select the race of an individual, as well as indicate their age, sex/gender and height. How race (or population) is determined varies, with most operators either asking patients to self-identify or ‘eyeballing it’. Interviews with users of the spirometer indicate that many operators are unaware that they are automatically activating race correction when they select a patient’s race (3). Because ‘correction’ is programmed into the spirometer by the manufacturer, it can be difficult to disable.”
Braun, Wolfgang, and Dickerson (2013) and Braun (2015) critiques pulmonary studies because in a large majority of cases, possible explanatory variables for lower lung functioning in black Americans could be related to SES. Harik-Khan, Muller, and Wise (2004) used participants from the Third National Health and Nutrition Examination Survey. They chose black and white children between the ages of 8 and 17 who did not smoke (n=1462, 623 whites and 839 blacks). Blacks were taller but had lower SES, had lower levels of vitamins A and C, along with lower levels of alpha carotene. They also had lower lung functioning. When they adjusted for confounds, sitting explained 42 to 53 percent of the racial difference, SES factors and antioxidant vitamin levels accounted for 7 to 10 percent of the difference. So they could only account for 50 to 63 percent of the difference. In 752 children aged 8 to 10 years of age, low birth weight accounted for 3 to 5 percent of the differences whereas maternal smoking had no effect (Harik-Khan, Muller, and Wise, 2004). So the remaining variation, obviously, will be accounted for by other SES variables, biology, or environmental factors.
Whitrow and Harding (2004) show that, at least for Caribbean blacks living in the UK, upper body differences explained most of the variation in lung functioning than did sitting height, with social correlates having a small but significant impact.
So because blacks have more type II fibers on average, they will convert glucose into energy more rapidly than whites. The energy for these muscle contractions comes from adenosine triphosphate (ATP). Blacks and whites both convert glucose into ATP for cellular functioning but in different ratios. These differences in muscular contractions driven by the metabolic pathway differences of the fibers are one large reason why blacks dominate sports.
Fibers are broken down into two types: fast and slow twitch. Slow twitch fibers use aerobic metabolism which is how they generate ATP and greater oxidative capacity due to higher levels for myoglobin. Oxygen bound to hemoglobin is carried to the red blood cells through capillaries that then influence muscular performance. Myoglobin is also essential for the transport of oxygen to the mitochondria where it is then consumed. Conversely, fast twitch fibers use anaerobic metabolism, have less oxidative capacity, less myoglobin and due to this, they are more dependent on anaerobic metabolism. Blacks also have “significantly higher levels of activity in their phosphagenic, glycolytic, and lactate dehydrogenase marbling pathways than their Caucasian counterparts” (Morrison and Cooper, 2006). This is where the production of ATP is regenerated,and so they have a huge advantage here. So higher faster production of ATP lead to more efficient ATP production, too. However when the ATP is depleted then it’s replaced by a reaction that depletes creatine phosphate. Skeletal muscle then converts “chemical energy into mechanical work” which only 30 to 50 percent is wasted as heat, so even small physiological differences can lead to large differences in performance (Morris and Cooper, 2006).
Though that’s not the only biochemical difference (faster ATP regeneration and production) between the blacks and whites that would explain sports performance. Morrison and Cooper (2006) write: “There is also considerably greater activity in the lactate dehydrogenase pathway of people of West African descent. A primary function of this pathway is to reduce muscle fatigue by converting lactic acid back to glucose and refeeding the muscles. This cyclic set of reactions, from muscles to liver and back to muscles, is known as the Cori cycle.”
Lactic acid production is that feeling in your muscles when during extended athletic activity whereas the postponement of muscle fatigue rests on the rate at which lactic acid is covered into glucose. The rate of this removal is further increased by the lactate dehydrogenase pathway describe above by Morrison and Cooper.
Clearly, the production of lactic acid causes problems during physical activity. The production of lactic acid into glucose to refers the muscles through the lactate dehydrogenase pathway is critical, for if glycogen reserves are depleted during extended physical activity then blood glucose would become the primary source of energy for the muscles, which could lead to lowered blood glucose levels and the nervous system may become compromised. During prolonged activity, however, if glucose isn’t available for energy then the body uses fat reserves which is less efficient than carbohydrates for energy and combustion.
Morrison and Cooper conclude: “Not the least of coincidence seems to be the influence of the compensatory sickle cell gene on oxygen transport and availability to the tissues. The reduced availability pulled with reduced oxygen myoglobin in the preponderant fast-twitch muscle fibres which are adapted for rapid anaerobic energy (ATP) regeneration, all give a new outcome of muscle anatomical and biochemical advantages which proffer a superior athleticism.”
Though, at the moment, as David Epstein states in his 2014 book The Sports Gene: Inside the Science of Extraordinary Athletic Performance, in a few studies done on mice genetically altered to have low hemoglobin levels, a there was a “shift of type IIa fast-twitch muscle fibers to type IIb “super fast twitch” muscle fibers in their lower legs” (Epstein, 2014: 179). This is also a developmental effect of mice in their lifetime, not a direct effect of evolution (Epstein, 2014: 179). No compensatory mechanism yet exists for humans, which I will attempt to untangle in future articles on the matter.
At the end of the chapter on this subject (Chapter 11, Malaria and Muscle Fibers, page 179), Epstein states that he asked physiologists their thoughts on the hypothesis. A few people approved of it, whereas one stated that he had evidence for physiological differences between blacks and whites that have not been studied before but he won’t release his results:
Several scientists I spoke to about the theory insisted they woud have no interest in investigating it because of the inevitably thorny issue of race involved. On of them told me that he actually has data on ethnic differences with respect to a particular physiological trait, but that he would never publish the data because of potential controversy. Another told me he would worry about following Cooper and Morrison’s line of inquiry because any suggestion of a physical advantage among a group of people could be equated to a corresponding lack of intellect, as if athleticism and intelligence were on some kind of biological teeter-totter. With that stigman in mind, perhaps the most important writing Cooper did in Black Superman [Cooper’s book] was his methodical eviseceration of any supposed inverse link between physical and mental prowess. “The concept that physical superiority could somehow be a symptomn of intellectual inferiority only developed when physical superiority became associated with African Americans,” Cooper wrote. “That association did not begin until about 1936.” The idea that athleticism was suddenly inversely proportional to intellect was never a cause of bigotry, but rather a result of it. And Cooper implied a more serious scientific inquiry into difficult issues, not less, is the appropriate path. (Epstein, 2014: 179) [Entine (2002) also spends a considerable amount of time debunking the myth of intelligence and athletic ability being negatively correlated in his 2002 book Taboo: Why Black Athletes Dominate Sports and Why We’re Afraid to Talk About It, which was kind of popularized by Rushton (1997) with his now debunked r/K selection theory.]
Things like this piss me off. These differences are actually measurable and lead to trait differences between the races, and know the mechanisms, pathways and whatnot and people are still. Scared to share their findings. One day, I hope, science will find a way to disregard people’s feelings in regard to people’s feelings on notable, testable and replicable differences between the races, most importantly between blacks and whites. I’ve noted how type II fibers lead to metabolic changes and small tears which then cause big problems. This is due to how fast the type II fibers fire in comparison to the slow twitch fibers.
This hypothesis is extremely interesting and now that I’ve laid out Morrison and Cooper’s (2006) hypothesis, I’m going to take a deep dive into this literature to see what I can prove about this hypothesis. Of course, the somatype along with the fiber distribution matters, as does having the XX genotype and not RR, which lends to superior athletic performance when coupled with type II muscle fibers (Broos et al, 2016). The pieces of this puzzle are, in my opinion, slowly being put together for someone to come along and integrate them into a coherent theory for the sickle cell trait and superior athletic performance through type II muscle fibers. It’s very interesting to note that elite sprinters were more likely to carry the SCT and that champion sprinters were more likely to have it too.
Is Diet An IQ Test?
1350 words
Dr. James Thompson is a big proponent of ‘diet being an IQ test‘ and has written quite a few articles on this matter. Though, the one he published today is perhaps the most misinformed.
He first shortly discusses the fact that 200 kcal drinks are being marketed as ‘cures’ for type II diabetes. People ‘beat’ the disease with only 200 kcal drinks. Sure, they lost weight, lost their disease. Now what? Continue drinking the drinks or now go back to old dietary habits? Type II diabetes is a lifestyle disease, and so can be ameliorated with lifestyle interventions. Though, Big Pharma wants you to believe that you can only overcome the disease with their medicines and ‘treatments’ along with the injection of insulin from your primary care doctor. Though, this would only exacerbate the disease, not cure it. The fact of the matter is this: these ‘treatments’ only ‘cure’ the proximate causes. The ULTIMATE CAUSES are left alone and this is why people fall back into habits.
When speaking about diabetes and obesity, this is a very important distinction to make. Most doctors, when treating diabetics, only treat the proximate causes (weight, symptoms that come with weight, etc) but they never get to the root of the problem. The root of the problem is, of course, insulin. The main root is never taken care of, only the proximate causes are ‘cured’ through interventions, however, the underlying cause of diabetes, and obesity as well is not taken care of because of doctors. This, then, leads to a neverending cycle of people losing a few pounds or whatnot and then they, expectedly, gain it back and they have to re-do the regimen all over again. The patient never gets cured, Big Pharma, hospitals et al get to make money off not curing a patients illness by only treating proximate and not ultimate causes.
Dr. Thompson then talks about a drink for anorexics, called ‘Complan“, and that he and another researcher gave this drink to anorexics, giving them about 3000 kcals per day of the drink, which was full of carbs, fat and vitamins and minerals (Bhanji and Thompson, 1974).
The total daily calorific intake was 2000-3000 calories, resulting in a mean weight gain of 12.39 kilos over 53 days, a daily gain of 234 grams, or 1.64 kilos (3.6 pounds) a week. That is in fact a reasonable estimate of the weight gains made by a totally sedentary person who eats a 3000 calorie diet. For a higher amount of calories, adjust upwards. Thermodynamics.
Thermodynamics? Take the first law. The first law of thermodynamics is irrelevant to human physiology (Taubes, 2007; Taubes, 2011; Fung, 2016). (Also watch Gary Taubes explain the laws of thermodynamics.) Now take the second law of thermodynamics which “states that the total entropy can never decrease over time for an isolated system, that is, a system in which neither energy nor matter can enter nor leave.” People may say that ‘a calorie is a calorie’ therefore it doesn’t matter whether all of your calories come from, say, sugar or a balanced high fat low carb diet, all weight gain or loss will be the same. Here’s the thing about that: it is fallacious. Stating that ‘a calorie is a calorie’ violates the second law of thermodynamics (Feinman and Fine, 2004). They write:
The second law of thermodynamics says that variation of efficiency for different metabolic pathways is to be expected. Thus, ironically the dictum that a “calorie is a calorie” violates the second law of thermodynamics, as a matter of principle.
So talk of thermodynamics when talking about the human physiological system does not make sense.
He then cites a new paper from Lean et al (2017) on weight management and type II diabetes. The authors write that “Type 2 diabetes is a chronic disorder that requires lifelong treatment. We aimed to assess whether intensive weight management within routine primary care would achieve remission of type 2 diabetes.” To which Dr. Thompson asks ‘How does one catch this illness?” and ‘Is there some vaccination against this “chronic disorder”?‘ The answer to how does one ‘catch this illness’ is simple: the overconsumption of processed carbohydrates, constantly spiking insulin which leads to insulin resistance which then leads to the production of more insulin since the body is resistant which then causes a vicious cycle and eventually insulin resistance occurs along with type II diabetes.
Dr. Thompson writes:
Patients had been put on Complan, or its equivalent, to break them from the bad habits of their habitual fattening diet. This is good news, and I am in favour of it. What irritates me is the evasion contained in this story, in that it does not mention that the “illness” of type 2 diabetes is merely a consequence of eating too much and becoming fat. What should the headline have been?
Trial shows that fat people who eat less become slimmer and healthier.
I hope this wonder treatment receives lots of publicity. If you wish to avoid hurting anyone’s feelings just don’t mention fatness. In extremis, you may talk about body fat around vital organs, but keep it brief, and generally evasive.
So you ‘break bad habits’ by introducing new bad habits? It’s not sustainable to drink these low kcal drinks and expect to be healthy. I hope this ‘wonder treatment’ does not receive a lot of publicity because it’s bullshit that will just line the pockets of Big Pharma et al, while making people sicker and, the ultimate goal, having them ‘need’ Big Pharma to care for their illness—when they can just as easily care for it themselves.
‘Trial shows that fat people who eat less become slimmer and healthier’. Or how about this? Fat people that eat well and exercise, up to 35 BMI, have no higher risk of early death then someone with a normal BMI who eats well and exercises (Barry et al, 2014). Neuroscientist Dr. Sandra Aamodt also compiles a wealth of solid information on this subject in her 2016 book “Why Diets Make Us Fat: The Unintended Consequences of Our Obsession with Weight Loss“.
Dr. Thompson writes:
I see little need to update the broad conclusion: if you want to lose weight you should eat less.
This is horrible advice. Most diets fail, and they fail because the ‘cures’ (eat less, move more; Caloric Reduction as Primary: CRaP) are garbage and don’t take human physiology into account. If you want to lose weight and put your diabetes into remission, then you must eat a low-carb (low carb or ketogenic, doesn’t matter) diet (Westman et al, 2008; Azar, Beydoun, and Albadri, 2016; Noakes and Windt, 2016; Saslow et al, 2017). Combine this with an intermittent fasting plan as pushed by Dr. Jason Fung, and you have a recipe to beat diabesity (diabetes and obesity) that does not involve lining the pockets of Big Pharma, nor does it involve one sacrificing their health for ‘quick-fix’ diet plans that never work.
In sum, diets are not ‘IQ tests’. Low kcal ‘drinks’ to ‘change habits’ of type II diabetics will eventually exacerbate the problem because when the body is in extended caloric restriction, the brain panics and releases hormones to stimulate appetite while stopping hormones that cause you to be sated and stop eating. This is reality; these studies that show that eating or drinking 800 kcal per day or whatnot are based on huge flaws: the fact that this could be sustainable for a large number of the population is not true. In fact, no matter how much ‘willpower’ you have, you will eventually give in because willpower is a finite resource (Mann, 2014).
There are easier ways to lose weight and combat diabetes, and it doesn’t involve handing money over to Big Pharma/Big Food. You only need to intermittently fast, you’ll lose weight and your diabetes will not be a problem, you’ll be able to lose weight and will not have problems with diabetes any longer (Fung, 2016). Most of these papers coming out recently on this disease are garbage. Real interventions exist, they’re easier and you don’t need to line the pockets of corporations to ‘get cured’ (which never happens, they don’t want to cure you!)
Athletic Ability and IQ
1150 words
Proponents of the usefulness of IQ tests may point to athletic competitions as an analogous test/competition that they believe may reinforce their belief that IQ tests ‘intelligence’ (whatever that is). Though, there are a few flaws in their attempted comparison. Some may say that “Lebron James and Usain Bolt have X morphology/biochemistry and therefore that’s why they excel! The same goes foe IQ tests!” People then go on to ask if I ‘deny human evolution’ because I deny the usefulness (that is built into the test by way of ‘item analysis; Jensen, 1980: 137) of IQ tests and point out flaws in their construction.
People who accept the usefulness of IQ tests and attempt to defend their flaws may attempt to make sports competition, like, say, a 100m sprint, an analogous argument. They may say that ‘X is better than Y, and the reason is ‘genetic’ in nature!’. Though, nature vs. nurture is a false dichotomy and irrelevant (Oyama, 1985, 2000; Oyama, 1999; Oyama, 2000; Moore, 2003). Behavior is neither ‘genetic’ nor ‘environmental’. with that out of the way, tests of athletic ability as mentioned above are completely different from IQ tests.
Tests of athletic ability do not have any arbitrary judgments as IQ tests do in their construction and analysis of the items to be put on the test. It’s a simple, cut-and-dry explanation: on this instance in this test, runner X was better than runner Y. We can then test runner X and see what kind of differences he has in his physiology and somatype, along with asking him what drives him to succeed. We can then do the same for the other athlete and discover that, as hypothesized, there are inherent differences in their physiology that make runner X be better than runner Y, say the ability to take deeper breaths, take longer strides per step due to longer legs, having thinner appendages as to be faster and so on. In regard to IQ, the tests are constructed on the prior basis of who is or is not intelligent. Basically, as is not the case with tests of athletic ability, the ‘winners and losers’, so to speak, are already chosen on the prior suppositions of who is or is not intelligent. Therefore, the comparison of athletic abilities tests and IQ tests are not good because athletic abilities tests are not constructed on the basis of who the constructors believe are athletic, like IQ tests are constructed on the basis of who the testers believe is ‘intelligent’ or not.
Some people are so far up the IQ-tests-test-intelligence idea that due to the critiques I cite on IQ tests, I actually get asked if I ‘deny human evolution’. That’s ridiculous and I will explain why.
Imagine an ‘athletic abilities’ test existed. Imagine that this test was constructed on the basis of who the test constructor believed who is or is not athletic. Imagine that he constructs the test to show that people who had previously low ability in past athletic abilities tests had ‘high athletic ability’ in this new test that he constructed. Then I discover the test. I read about it and I see how it is constructed and what the constructors did to get the results they wanted, because they believed that the lower-ability people in the previous tests had higher ability and therefore constructed an ‘athletic abilities’ test to show they were more ‘athletic’ than the former high performers. I then point out the huge flaws in the construction of such a test. The logic of people who claim that I deny human evolution because I blast the validity and construction of IQ tests would, logically, have to say that I’m denying athletic differences between groups and individuals, when in actuality I’m only pointing out huge flaws in the ‘athletic abilities’ test that was constructed. The athletic abilities example I’ve conjured up is analogous to the IQ test construction tirade I’ve been on recently. So, if a test of ‘athletic ability’ exists and I come and critique it, then no, I am not denying athletic differences between individuals I am only pointing out flawed tests.
The basic structure of my ‘athletic abilities’ argument is this: that test that would be constructed would not test true ‘athletic abilities’ just like IQ tests don’t test ‘intelligence’ (Richardson, 2002). Pointing out huge flaws in tests does not mean that you’re a ‘blank slatist’ (whatever that is; it’s a strawman for people who don’t bow down to the IQ alter). Pointing out flaws in IQ tests does not mean that you believe that everyone and every group is ‘equal’ in a psychological and mental sense. Pointing out the flaws in IQ tests does not mean that one is a left-wing egalitarian that believes that all humans—individuals and groups—are equal and that the only cause of their differences comes down to the environment (whether SES or the epigenetic environment, etc). Pointing out flaws in these tests is needed; lest people truly think that they do test, say, ability for complex cognition (they don’t). Indeed, it seems that everyday life is more complicated than the hardest Raven’s item. Richardson and Norgate (2014) write:
Indeed, typical IQ test items seem remarkably un-complex in their cognitive demands compared with, say, the cognitive demands of ordinary social life and other everyday activities that the vast majority of children and adults can meet. (pg 3)
On the other hand abundant cognitive research suggests that everyday, “real life”
problem solving, carried out by the vast majority of people, especially in social-cooperative situations, is a great deal more complex than that required by IQ test items, including those in the Raven. (pg 6)
Could it be possible that ‘real-life’ athletic ability, such as ‘walking’ or whatnot be more ‘complex’ than the analog of athletic ability? No, not at all. Because, as I previously noted, athletic abilities tests test who has the ‘better’ physiology or morphology for whichever competition they choose to compete in (and of course there will be considerable self-selection since people choose things they’re good at). It’s clear that there is absolutely no possibility of ‘real-life’ athletic ability possibly being more complex than tests of athletic ability.
In sum, no, I do not deny human evolution because I critique IQ tests. Just because I critique IQ tests doesn’t mean that I deny human evolution. My example of the ‘athletic test’ is a sound and logical analog to the IQ critiques that I cite. Just framing it in the way of a false test of athletic ability and then pointing out the flaws is enough to show that I don’t deny human evolution. Because if such an ‘athletic abilities’ test did exist and I pointed out its flaws, I would not be denying differences between groups or individuals due to evolution, I’d simply be critiquing a shitty test, which is what I do with IQ tests. Actual tests of athletic ability are not analogous to IQ tests because tests of athletic ability are not ‘constructed’ in the way that IQ tests are.
The Genomic Health of Our Ancestors: What Was It Like and Is It Relevant for Us Today?
1500 words
After I published my article Thoughts On Diseases of Civilization: Romanticizing the Hunter-Gatherer’s Diet the other day, someone dropped by and stated that we are ‘getting healthier and healthier’, citing an article by Berens, Cooper, and Lachance (2017) titled “The genomic health of ancient hominins” who show, through genetic analyses, that many of our ancestors had the ‘genes for’ diseases that plague us today in our societies. While this may be true, one important thing that the individual who left the paper did not say is that genotypic health does not equal phenotypic health.
The basic assumption of the paper is this: They genotyped the Altai Neanderthal, Denisovans, pastoralists and hunter-gatherers and computed their ‘GRS’ (genetic [disease] risk score). When focusing on the GRS, they found that the Altai Neanderthal had 97 percent worse ‘genomic health’ when compared to the genomes of people today, whereas Otzi man had a ‘genetic predisposition’ to cardiovascular and gastrointestinal disease.
Something important to keep in mind here is that GRS and sequencing the genomes of ancient hominins can only ‘predict’ what types of problems one would have based on their genomes; it cannot realiably state that this individual would have gotten/did get a certain disease because he had the alleles for it.
What they did was genotype ancient hominins and then compute their GRS and compare the ancient hominins GRS to that of a modern human and then match the set of “disease loci to generate standardized GRS percentiles“. The ancient samples they tested had a similar genetic risk when compared to modern samples, though the ancient samples may underestimate their genetic risk since there are numerous other alleles yet to be discovered that may cause or add to genetic disease risk.
Ancient hominins had lower risks for cancer, miscellaneous diseases and neurological/psychological diseases when compared to modern humans. According to their analysis, ancient hominins only had a higher risk for cardiovascular disease while “Risks of allergy/autoimmune, morphological/muscular, metabolism/weight, and dental/periodontal diseases were not significantly different between ancient and modern hominins” (Berens, Cooper, and Lachance, 2017). So ancient hominins seemed to have a reduced risk of cancer, neurological disease and other unclassified diseases.
The Altai Neanderthal was at high risk of immunological diseases, cancers, gastrointestinal problems, morphological and muscular problems, and other metabolic disorders. However, and this is important, this is only what his genome showed. This is only a risk assessment and DOES NOT state anything about phenotypic health. The Altai Neanderthal, however, did have a lower GRS for cardiovascular disease and average risk for dental diseases. This is in contrast with Otzi man, who had a genetic risk for cardiovascular disease. Otzi also had a high GRS score on immuno-related diseases, gastrointestinal diseases and other metabolic disorders—which I would assume would be similar to type II diabetes mellitus. However, Otzi had ‘normal’ risk for morphological and neurological disease.
I had to wait all paper to read this:
We note that genomic health does not necessarily equate to phenotypic health. Genetic risk scores are not deterministic, instead they merely indicate whether an individual has a predisposition to a particular disease. In addition, alleles that contribute to disease in modern environments may not have had the same effects in past environments.
This makes it an open and shut case. Just because you have the ‘predisposition’ for something doesn’t mean that it will occur to you. For example, if someone has a ‘genetic predisposition’ to become and alcoholic and he never drinks alcohol, will he become an alcoholic? If someone is extremely sensitive to carbohydrate intake and more susceptible to the allure of sugar and more likely to get addicted to it, but they never eat the carbs will they become obese and insulin resistant? The genes-as-destiny paradigm is wrong—especially in regard to human disease. Human disease is extremely complex and doctors are even having problems with GWAS and what it shows for the genetic basis for disease.
Further, in regard to disease, GWAS has a huge problem in detecting genetic variants: “many GWAS hits have no specific biological relevance to disease and wouldn’t serve as good drug targets. Rather, these ‘peripheral’ variants probably act through complex biochemical regulatory networks to influence the activity of a few ‘core’ genes that are more directly connected to an illness.” See also Boyle and Pritchard (2017): An Expanded View of Complex Traits: From Polygenic to Omnigenic. Disease-nomics will be much more complicated than identifying one or a few genes; gene networks interact with the environment—whether by what we eat or our immediate surroundings—and diseases arise through a complex interaction between genes and environment: GxE.
When our ancestors made the transition from a hunter-gatherer lifestyle to a more sedentary, agricultural one, this is what then started up the environmental mismatch between humans and our environments. Agriculturalists had the highest GRS for dental caries and other problems to do with dentition, though the number of alleles was small, it makes logical sense for the advent of agriculture to increase the incidence of dental caries and other problems with dentition, which would then be selected for due to the change of lifestyle from mobile hunter-gatherer to relatively sedentary agriculturalist. Hunter-gatherers have fewer dental caries than agriculturalists. It is also argued that when we began to eat fermentable plant foods, that this caused “changes in food processing caused an early shift toward a disease-associated oral microbiota in this population” (Humphrey et al, 2014). Adler et al (2013) also show that “Data from 34 early European skeletons indicate that the transition from hunter-gatherer to farming shifted the oral microbial community to a disease-associated configuration.” Clearly, the transition from the mobile hunter-gatherer lifestyle to the sedentary agriculturalist one was extremely bad for our health and dentition.
Though agriculture did increase the incidence of dental caries, evidence exists that, through dietary shifts in the Upper Paleolithic, dental caries appeared, probably due to the shift to more processed foods (keep in mind that processing food only has to mean, say, mashing food to make it easier to chew, not in the modern definition of ‘processing’). Nevertheless, the first toothpicks were discovered from the Late Upper Paleolithic, which implies that some human populations encountered some foods that then gave them dental caries to which our ancestors responded by making toothpicks (Oxilia et al, 2015). Hunter-gatherers had few—if any—dental caries which implies that their lifestyles did not give them the oral disease. It’s very peculiar that these have only been noticed, really, in populations that underwent the agricultural transformation. That’s yet another ‘disease of civilization’ that is low to nonexistent in those populations, which is attributed to their lifestyle and their diet.
Cultural evolution drives mismatch diseases as cultural evolution can greatly outstrip Darwinian evolution. This, especially in regard to our health, is bad for us since we did not have the time to biologically adapt to our new, novel diets. We still have yet to adapt genetically to the diets and lifestyle taken on by our ancestors 10kya, and I think it will be a long time—if ever—before we do adapt. I mean come on, can you really see whole groups of people adapting to constant insulin spikes brought on by highly processed carbohydrates and other foods? We are the running ape, so do you ever see us adapting to constantly sit? These are modern problems, which were brought on by our ancestors’ adoption of agriculture. I agree with Jared Diamond when he says that farming was ‘the worst mistake in the history of the human race‘, but, obviously not for the Marxist reasons he proposes. Clearly, hunter-gatherers had better phenotypic health while ours suffers.
In sum, the paper Berens, Cooper, and Lachance (2017) does not refute anything that I wrote in my previous article on diseases of civilization. If anything, most of what I wrote is strengthened, especially on the basis of genotypic health not equalling phenotypic health. This paper can be summed with three points:
1) genes aren’t destiny. 2) genes wouldn’t necessarily do the same things in different environments. 3) the GRS (genetic [disease] risk scores) are also not deterministic. This is the logical conclusion to draw. OK, so ancient hominins had a higher genetic risk for certain diseases. Here’s the catch: if they weren’t in the environments that would exacerbate the disease and cause it to express in the phenotype, does it really matter that they had ‘genetic predispositions’ for certain diseases? Of course it matters for us today due to our built food environments, but did it matter for them who did not have access to the novel environments that we do today?
This is a very interesting paper but my arguments on diseases of civilization still stand. Diseases of civilization will still plague our societies until we change the built food environment, but until then, we will have to live with the worst mistake we have made as a species: constructing obesogenic environments that then lead to a huge decrease in quality of life and life expectancy.
IQ Test Construction
1550 words
No one really discusses how IQ tests are constructed; people just accept the numbers that are spit out and think that it shows one’s intelligence level relative to others who took the test. However, there are huge methodological flaws in regard to IQ tests—one of the largest, in my opinion, being that they are constructed to fit a normal curve and based on the ‘prior knowledge’ of who is or is not intelligent.
What people don’t understand about test construction is that the behavior genetic (BG) method must assume a normal distribution. IQ tests have been constructed to display this normal distribution, so we cannot say whether or not it exists in nature, though few human traits fall on the normal distribution. The fact of the matter is this: The normal curve is achieved through keeping more items that people get right while keeping the smaller proportion of items that people get right and wrong. This forces the normal curve and all of the assumptions that come along with this so-called IQ bell curve.
Even then, the fact that the normal distribution is forced doesn’t mean as much as the assumptions and conclusions drawn from the forced curve. It is assumed that individual test score differences arise out of ‘biology’, however with how test questions are manipulated to get the results that the test constructors want, it is then assumed that the cause for individual test score differences are ‘biological’ in nature, however we don’t know if these distributions are ‘biological’ in nature due to how the tests are constructed.
The fact of the matter is, the tests are constructed based off of the prior knowledge of who is or is not intelligent. This means that we can ‘build the test’ to fit these preconceived notions. The problem of item selection was discussed by Richardson (1998) who discussed boys scoring a few points higher than girls, and wondering whether or not these differences should be ‘allowed to persist’ or not. Richardson (1998: 114) writes (12/26/17 Edit: I’ll also provide the quote that precedes this one):
“One who would construct a test for intellectual capacity has two possible methods of handling the problem of sex differences.
1 He may assume that all the sex differences yielded by his test items are about equally indicative of sex differences in native ability.
2 He may proceed on the hypothesis that large sex differences on items of the Binet type are likely to be factitious in the sense that they reflect sex differences in experience or training. To the extent that this assumption is valid, he will be justified in eliminating from his battery test items which yield large sex differences.
The authors of the New Revision have chosen the second of these alternatives and sought to avoid using test items showing large differences in percents passing.” (McNemar 1942:56)This is, of course, a clear admission of the subjectivity of such assumptions: while ‘preferring’ to see sex differences as undesirable artefacts of test composition, other differences between groups or individuals, such as different social classes or, at various times, different ‘races’, are seen as ones ‘truly’ existing in nature. Yet these, too, could be eliminated or exaggerated by exactly the same process of assumption and manipulation of test composition.
And further writes on page 121:
Suffice it to say that investigators have simply made certain assumptions about ‘what to expect’ in the patterns of scores, and adjusted their analytical equations accordingly: not surprisingly, that pattern emerges!
The only ‘assumption’ that the test constructors have is the biases they already have on who is or is not ‘intelligent’ and then they construct the test through item selection, excising items that don’t fit their desired distribution. Is that supposed to be scientific? You can ask a group of children a bunch of questions and then construct a test to get the conclusion you want based on item selection.
The BG method needs to assume that IQ test scores lie on a normal curve and that it is a quantitative trait that exhibits a normal distribution, though Micceri (1989) showed that normal distributions for measurable traits are the exception, rather than the rule, for numerous measurable traits. Richardson (1998: 113) further writes:
The same applies to many other ‘characteristics’ of IQ. For example, the ‘normal distribution, or bell-shaped curve, reflects (misleadingly as I have suggested in Chapters 1 to 3) key biological assumptions about the nature of cognitive abilities. It is also an assumption crucial to many statistical analyses done on test scores. But it is a property built into a test by the simple device of using relatively more items on which about half the testees pass, and relatively few items on which either many or only a few of them pass. Dangers arise, of course, when we try to pass this property off as something happening in nature instead of contrived by test constructors.
So with the knowledge of test construction, then there is something very obvious here: we can construct IQ tests that, say, show blacks scoring higher than whites and women scoring higher than men. We can then make the assumption that there are genes that are responsible for this distribution and then ‘find genes’ that supposedly cause these differences in test scores (which are constructed to show the differences!). What then? Let’s say that someone did do that, would the logical conclusion be that there are genes ‘driving’ the differences in IQ test scores?
Richardson (2017: 3) writes:
In summary, either directly or indirectly, IQ and related tests are calibrated against social class background, and score differences are inevitably consequences of that social stratification to some extent. Through that calibration, they will also correlate with any genetic cline within the social strata. Whether or not, and to what degree, the tests also measure “intelligence” remains debateable because test validity has been indirect and circular. … Such circularity is also reflected in correlations between IQ and adult occupational levels, income, wealth, and so on. As education largely determines the entry level to the job market, correlations between IQ and occupation are, again, at least partly, self-fullfilling. … CA [cognitive ability], as measured by IQ-type tests, is intrinsically inter-twined with social stratification, and its associated genetic background, by the very nature of the tests.
This, again, falls back on the non-existent construct validity that IQ tests have. Construct validity “defines how well a test or experiment measures up to its claims.” No such construct validity exists for IQ tests. If breathalyzers didn’t test someone’s fitness to drive, would they still be a good measure? If they had no construct validity, if there was no biological model to calibrate the breathalyzer against, would we still accept it as a realistic model to test people against and judge their fitness to drive? Still yet another definition of construct validity comes from Strauss and Smith (2009) who write that psychological constructs are “validated by testing whether they relate to measures of other constructs as specified by theory.” No such biological model exists for IQ; why expect some type of biological model like this when there are other perfectly well-reasoned response to how and why individuals differ in IQ test scores (Richardson, 2002)?
The normal distribution is forced, which IQ-ists claim to know. Richardson (1998) notes that Jensen “noted how ‘every item is carefully edited and selected on the basis of technical procedures known as “item analysis”, based on tryouts of the items on large samples and the test’s target population’ (1980:145).” These ‘tryouts’ are what force the normal curve, and no matter how ‘technical’ the procedures are, there are still huge biases, which then make people draw huge assumptions, again, based on who is or is not intelligent.
Simon (1997: 204) writes (emphasis mine):
There is another, and completely irrefutable, reason why the bell-shaped curve proves nothing at all in the context of H-M’s book: The makers of IQ tests consciously force the test into such a form that it produces this curve, for ease of statistical analysis. The first versions of such tests invariably produce odd-shaped distributions. The test-makers then subtract and add questions to find those that discriminate well between more-successful and less-successful test-takers. For this reason alone the bell-shaped IQ curve must be considered an artifact rather than a fact, and therefore tells us nothing about human nature or human society.
Simon (1997) rightly notes, as I have numerous times, how biased (against certain classes) the excision of items during their analysis and selection (of test items). This shows that both the so-called normal curve and the outcomes they supposedly show aren’t “natural”, but are chosen and forced by the test constructors and their biased and presuppositions about what “intelligence” is. John Raven, for example, also stated in his personal notes how he used his “intuition” to rank-order items, while others further noted that there was no “underlying processing theory” to guide item difficulty and retain old items on newer versions of the test (Carpenter, Just, and Shell: 408).
In sum, IQ tests are constructed to fit a normal curve on the basis of an assumption of a normal distribution, and on the presupposed basis of who is or is not ‘intelligent’ (whatever that means). The BG method needs to assume that IQ is a quantitative trait which exhibits a normal distribution. IQ is assumed to be like height, or weight, but which physiological process in the body does it mimick? I have argued that there is no physiological basis to ‘IQ’ or what they test and that they can be explained not by biology, but through test construction. I wonder what the distributions of IQ test scores would look like without forced normal distributions? Since it is assumed that IQ tests something directly measurable—like height and weight as is normally used—then they must fall on a normal distribution, which all other measurable psychological traits do not show (Micceri, 1989; Buzsaki and Mizseki, 2014).
Some may argue that ‘they know this’ (they being psychometricians). However, ‘they’ must know that most of their assumptions and conclusions about ‘good and bad genes’ lie on the huge assumption of the normal distribution. IQ test scores do not show a normal distribution, they were designed to create it. The fact that most psychological traits show a strong skew to one side and so that’s why a normal distribution is forced is meaningless. The fact of the matter is, just through how the tests are constructed means that we should be cautious as to what these tests test with the assumptions that we currently have about them.
Race and Strength on the Big Four Lifts
2450 words
Different races have different morphology/somatype. Therefore, we can reason that different races would fare better or worse at a certain lift depending on their limb length, such as leg length, arm length, torso length and so on. How do somatypic differences lead to differences in strength between the races on the Big Four lifts? The four lifts I will cover are bench press, deadlift, squat and overhead press.
Squat
East Asians
East Asians have higher levels of body fat (for instance the Chinese, Wang et al, 2011) and have lower BMIs, yet higher levels of body fat (Wang et al, 1994). This, along with their somatype are part of the reason why they excel in some strength sports. Since East Asians have a smaller stature, averaging about 5 feet 8 inches, with shorter arms and legs. Thinking about how the ancestors of the East Asians evolved, this makes sense: they would have needed to be shorter and have shorter limbs as it is easier to warm a body with a smaller surface area. Therefore, while squatting they have a shorter path to travel with the bar on their back. East Asians would strongly excel at the squat, and if you watch these types of competitions, you’d see them strongly overrepresented—especially the Chinese.
African-Americans
African-Americans are descended from West African slaves, and so they have longer, thinner limbs with lower amounts of body fat on average (especially if they have more African ancestry), which is a classic sign of a mesomorphic phenotype. They do also skew ecto, which is useful in the running competitions they dominate (in the case of West Africans and descendants and certain tribes of Kenyans and Ethiopians). Either way, due to their long limbs and a short torso, they have to travel further with the weight therefore here they suffer and wouldn’t be as strong as people who have a long torso with shorter limbs.
European Americans
Like East Asians, Europeans have similar morphology—skewing ectomorphic, the somatype that dominates strength competitions. Having a long torso with shorter limbs and more type I than type II fibers, they would then be able to lift more, especially since these competitors keep a high body fat percentage. Again, like with East Asians, there is a biomechanical advantage here and due to their higher levels of body fat and endomorphic somatype along with shorter limbs, they would be able to move more weight on the squat, especially more than African-Americans. Biomechanics is key when it comes to evaluating different groups’ morphology when attempting to see who would be stronger on average.
Deadlift
East Asians
The deadlift is pretty straightforward: bending down and deadlifting the weight off of the ground. Key anatomic differences between the races dictate who would be better here. East Asians, with shorter limbs and a longer torso the bar has to travel a further path, compared to someone with longer limbs and shorter torso. Though, someone with short limbs and a short torso would also have a biomechanical advantage in pulling, it is nothing like if one has long arms and a short torso.
African-Americans
Here is where they would shine. Their anatomy is perfect for this lift. Since they have longer limbs and a shorter torso, the bar has a shorter path to travel to reach the endpoint of the lift. At the set-up of the lift, they already have a biomechanical advantage and they can generate more power in the lift due to their leverage advantage. The deadlift favors people with a long torso, short femurs, and long arms, and so it would favor African-Americans. (Their long arms off-sets their short torsos, though the bar would still have to travel further, they still would have the ability to move more weight.)
European Americans
European Americans would have the same biomechanical problems as East Asians, but not as much since they have a taller stature. It is well-known in the world of weightlifting that having shorter, ‘T-rex arms’ impedes strength on the lift, since speaking from an anatomic viewpoint, they are just not built for it. No style of deadlift (the sumo or conventional) suits people with short arms, and so they are already at a biomechanical disadvantage. Relative to African-Americans, European Americans have ‘T-rex arms’ and therefore they would suffer at pulling exercises—deadlift included.
Overhead press
East Asians
The overhead press is where people with shorter arms would excel. Thus, East Asians would be extremely strong pushers. Say the bar starts at the top of their chest, the path of the bar to the lockout would be shorter than if someone had longer arms. The size of the trapezius muscles also comes into play here, and people with larger trapezius muscles have a stronger press. The East Asians short stature and therefore shorter limbs is perfect for this lift and why they would excel.
African-Americans
African-Americans would suffer at the overhead press for one reason: their long limbs, mainly their arms. The bar has a further path to travel and thus strength would be impeded. Indeed, people not built for pressing have long arms, long torsos, and long legs. Performing the full range of motion, African-Americans would have less strength than East Asians and European Americans.
European Americans
Again, due to similar morphology as East Asians, they, too, would excel at this lift. Since the lift is completed when the arms lock out, those with shorter arms would be able to move more weight and so what hurts them on the deadlift helps on pressing movements like the overhead press.
Bench press
East Asians
Lastly, the bench press. East Asians would excel here as well since they have shorter arms and the bar would have a shorter path to travel. Notice anything with bar movement? That’s a key to see which group would be stronger on average: looking at the average morphology of the races and then thinking about how the lift is performed, you can estimate who would be good at which lift and why. The bench press would favor someone with a shorter stature and arms, and they’d be able to lift more weight. (I personally have long arms compared to my body and my bench press suffers compared to my deadlift.) However, Caruso et al (2012) found that body mass is a more important predictor of who would excel at the bench press. East Asians have a higher body fat percentage, and therefore would be stronger on average in the lift.
African Americans
Here, too, African-Americans will suffer. Like with the overhead press, the bar has a further path to travel. They also have less body fat on average and that would also have the bar travel more, having the individual put more exertion into the lift compared to someone who had shorter arms. The longer your arms are in a pushing exercise, the further the bar has to travel until lockout. Thus you can see that people with longer arms would suffer in the strength department compared to people with shorter arms, but this is reversed for pulling exercises like the deadlift described above. (There is also a specific longitudinal study on black-white differences in bench press which I will cover in the ‘Objections‘ section.)
European Americans
Again, like with East Asians due to similar somatype, European Americans, too, would excel at this lift. They are able to generate more pound-for-pound power in the lift. The bar also has a shorter path to travel and since the people who compete in these competitions also have higher levels of body fat, then the bar has less of a distance to travel, thus increasing the amount of force the muscle can generate. Limb size/body mass/somatype predict how races/individuals would do on specific lifts.
Objections
One of the main objections that some may have is that one longitudinal study on black and white police officers found that blacks were stronger than whites at the end of the study (Boyce et al, 2014). However, I heavily criticized this paper at the beginning of the year and for good reason: heights of the officers weren’t reported (which is not the fault of the researchers but of an ongoing lawsuit at that department since people complained that they were discriminating against people based on height). The paper is highly flawed, but looking at it on face value someone who does not have the requisite knowledge they would accept the paper’s conclusions at face value. One of the main reasons for my criticism of the paper is that the bench press was tested on a Smith machine, not a barbell bench press. Bench pressing on the Smith machine decreases stability in the biceps brachii (Saterbakken et al, 2011) but there is similar muscle recovery between different bench presses in trained men (Smith, barbell, and dumbbell) (Ferreira et al, 2016). This does not affect my overall critique of Boyce et al (2014) however, since you can move more weight than you would normally be able to, along with the machine being on one plane of motion so everyone has to attempt to get into the same position to do the lift and we know how that is ridiculous due to individual differences in morphology.
Some may point to hand-grip tests, which I have written about in the past, and state that ‘blacks are stronger’ based on hand-grip tests. Just by looking at the raw numbers you’d say that blacks had a stronger grip. However, to get an idea of the strength differences pound-for-pound there is a simple formula: weight lifted/bodyweight=how strong one is pound-for-pound on a certain exercise. So using the values from Araujo et al (2010), for blacks we have a grip strength of 89.826 with an average weight of 193 pounds. Therefore pound-for-pound strength comes out to .456. On the other hand, for Europeans, they had an average grip strength of 88.528 pounds with an average weight of 196 pounds, so their pound-for-pound grip strength is about .452, which, just like African-Americans is almost half of their body weight. One must also keep in mind that these hand-grip studies are done on older populations. I have yet to come across any studies on younger populations that use the big four lifts described in this article and seeing who is stronger, so inferences are all that we have.
Further, Thorpe et al (2016) also show how there is an association between household income and grip-strength—people who live in homes with higher incomes have a stronger grip, with blacks having a stronger grip than whites. Thorpe et al (2016) showed that black women had a stronger grip strength than white women, whereas for black men they only had a stronger grip than white men at the highest SES percentile. This could imply nutrient deficiencies driving down their ability for increases grip strength, which is a viable hypothesis. Although Thorpe et al (2016) showed that black men had a stronger grip strength, these results conflict with Haas, Krueger, and Rohlfson (2012) though the disparities can be explained by the age of both cohorts.
Nevertheless, grip strength—as well as overall strength—is related to a higher life expectancy (Ruiz et al, 2008; Volkalis, Haille, and Meisinger, 2015). If blacks were stronger—and this is being debated with studies like hand-grip—then we should expect to see black men living longer than white men, however, we see the opposite. Black men die earlier than white men, and it just so happens that the diseases that are correlated with strength and mortality are diseases that blacks are more likely to get over whites. One should think about this if they’re entertaining the idea that blacks have an inherent strength advantage over whites.
Others may argue that since chimpanzees have a higher proportion of type II fibers and that’s one reason why they are stronger than us by 1.35 times (O’Neill et al, 2017) and have the ability to rip our faces off. Of course, other factors are at play here other than the chimps’ fast twitch fiber content. Of course, one must also think of the chimpanzee’s way smaller stature when discussing their overall strength. It’s not just their type II fibers, but how much smaller they are which gives them the ability to generate more force pound-for-pound in comparison to humans. So this is a bad example to attempt to show that blacks are stronger than whites based solely on the composition of the muscle fibers.
Finally, back in July I argued that Neanderthals would be stronger than Homo sapiens due to their morphology and a wide waist. This, of course, has implications for strength differences between the races. People with a wider waist would have the ability to generate more power. Blacks have a higher center of gravity due to longer limbs whereas whites and Asians have lower centers of gravity due to a longer torso. Along with climatic conditions, the Neanderthal diet also contributed to their wide waist and thorax, which would then help with strength. Therefore, this has implications for racial differences in strength. We can replace Europeans with Neanderthals and Homo sapiens with Africans and the relationship would still hold. This is yet more proof that blacks are not stronger than whites. This article also contributes to the argument I laid out in my article on how racial differences in muscle fiber typing predict differences in elite sporting competition. Morphology/somatype is the final piece of the puzzle; without the correct morphology, it’d be really hard for someone to become an elite athlete in a certain field if they do not have the correct morphology.
Conclusion
Looking at the big four lifts, the advantage goes to European Americans and East Asians. This is due to their average somatype and morphology. The only lift that Africans would excel at is the deadlift and this is due to their morphology—mainly their long arms. People with longer arms excel at pulling exercises whereas people with shorter arms excel at pushing exercises. Hand-grip strength studies show blacks having a higher grip strength than whites, however in one study if you see who is stronger pound-for-pound, the differences are insignificant. The longitudinal bench press study is highly flawed due to numerous confounds and is therefore unacceptable to assess strength and race. The fact that chimpanzees have a higher proportion of type II fibers compared to humans is also irrelevant. Chimpanzees have a smaller stature and they can, therefore, generate way more power pound-for-pound. Attempting to replace Africans with chimpanzees in this scenario doesn’t make sense because Africans have longer limbs than Europeans and would, therefore, generate less force pound-for-pound. Overall strength is related to mortality; stronger people live longer and have fewer maladies than weaker people. This too lends credence to my argument that whites are stronger than blacks.
Thoughts On Diseases of Civilization: Romanticizing the Hunter-Gatherer’s Diet
2650 words
One of the first things that pops into people’s minds when they hear about hunter-gatherers is most likely the myth of the ‘Noble Savage’—the belief that those who do not have civilization are ‘good’, whereas civilization corrupts Man. This myth, though, has been put to bed numerous times, like in Steven Pinker’s 2003 book The Blank Slate and more recently @EvolvingMoloch’s article Romanticizing the Hunter-Gatherer. (H/t to @EvolvingMoloch for the title.) However, I’m not too worried about claims about their ‘good nature’ from anthropologists; what I find much more interesting is their low rates of so-called diseases of civilization—diseases that seemed to appear after a society reaches a certain ‘tipping point’ if you will. These diseases that are prevalent in first-world societies are low to non-existent in these types of societies. Why?
All you need to do when thinking about the why of diseases of civilization is simple: think about the introduction of processed carbohydrates along with the introduction of a lot of high sugar, highly processed, high salt food. Though, people who do not eat these types of foods—especially on a societal level—do not have the same types of diseases that we have in the first-world. Since this seems to be true—that societies don’t have what I term ‘the Western scourge’, our Western diet—then it would seem that civilization had one negative effect on our lives, and that is the reason why I romanticize the hunter-gatherers’ diet.
My two main sources on diseases of civilization are Gary Taubes’ 2008 book Good Calories, Bad Calories and Daniel Lieberman’s 2013 book The Story of the Human Body: Evolution, Health, and Disease. Taubes’ book has a singular chapter—chapter 5—on diseases of civilization whereas Lieberman’s book goes much more in-depth on the hows and whys. Though Taubes’ whole book—along with his follow-up Why We Get Fat: And What to Do About It and his new book published in December of 2016 titled The Case Against Sugar—are pretty much critiques of the Western diet and explain the biochemical and physiological processes and reasons of how and why we get fat and how our first-world lifestyles are the cause of it. There are numerous testimonies from doctors from the early 19th century that attest to the great health and non-existent diseases that plague us in our societies.
The following are quotes from Taubes’ (2008) book Good Calories, Bad Calories:
In 1914, Hoffman himself had surveyed physicians working for the Bureau of Indian Affairs. “Among some 63,000 Indians of all tribes,” he reported, “there occurred only 2 deaths from cancer as medically observed from the year 1914.” (Taubes, 2008: 92)
“There are no known reasons why cancer should not occasionally occur among any race of people, even though it be below the lowest degree of savagery and barbarism,” Hoffman wrote. (Taubes, 2008: 92)
“Granting the practical difficulties of determining with accuracy the causes of death among the non-civilized races, it is nevertheless a safe assumption that the large number of medical missionaries and other trained medical observers, living for years among native races throughout the world, would long ago have provided a substantial basis of fact regarding the frequency of malignant disease among the so-called “uncivilized” races, if cancer were met with among them to anything like the degree common to practically all civilized countries. Quite the contrary, the negative evidence is convincing that in the opinion of qualified medical observers cancer is exceptionally rare among the primitive peoples.” (Taubes, 2008: 92)
These reports, often published in the British Medical Journal, The Lancet or local journals like the East African Medical Journal, would typically include the length of service the author had undergone among the natives, the size of the local native population served by the hospital in question, the size of the local European population, and the number of cancers involved in both. F.P. Fouch, for instance, district surgeon of the Orange Free State in South Africa, reported to the BMJ in 1923 that he had spent six years at a hospital that served fourteen thousand natives. “I never saw a single case of gastric or duodenal ulcer, colitis, appendicitis, or cancer in any form in a native, although these diseases were frequently seen among the white or European population.” (Taubes, 2008: 92)
As a result of these modern processed foods, noted Hoffman, “far-reaching changes in bodily functioning and metabolism are introduced which, extending over many years, are the causes or conditions predisposing to the development of malignant new growths, and in part at least explain the observed increase in cancer death rate of practically all civilized and highly urbanized countries.” (Taubes, 2008: 96)
Is it any coincidence that these diseases are so prevalent in European populations but not hunter-gatherer’s? I think not.
The same has been noted with the Pima Indians: before the introduction of the scourge we call a ‘diet’, they had low to non-existent rates of obesity and other types of metabolic diseases. Then, when our diet made its way to their societies, their lives changed:
For perhaps two millenia, the Pima have lived as both hunter-gatherers and agriculturalists. Game was abundant in the region, as were fish and clams in the Gila River. When the Jesuit missionary Eusebio Kino arrived among the Pima in 1787, the tribe was already raising corn and beans on fields irrigated with Gila River water. In the decades that followed, they took to raising cattle, poultry, wheat, melons, and figs. They also ate mesquite beans, the fruit of the saguaro cactus and a mush of what Russell later called “unidentified worms.” In 1846, when a U. S. Army battalion passed through Pima lands, the battalion’s surgeon John Griffin describes the Pima as “sprightly” and in “fine health.” He also noted that the Pima has “the greatest abundance of food, and take care of it well, as we saw many of their storehouses full of pumpkins, melons, corn, etc.” (Taubes, 2007: 237)
Hrdlicka also noted that by 1905 the Pima diet already included “everything obtainable that enters into the dietary of the white man,” which raises the possibility that this might have been responsible for the obesity. (Taubes, 2007: 238)
Obesity and diabetes (diabesity) was low to nonexistent in the Pima and perhaps the only reason for this was that they did not live off of highly processed carbohydrates and other Western foods. When these foods were introduced to these people, then the modern diseases of civilization then appeared.
This is noticed everywhere the Western diet goes. This is even occurring in China, which had historically low rates of obesity. However with the introduction of the Western ‘diet’, this is now changing. China now has the largest overweight population in the world, along with the largest number of obese children in the world. Another coincidence?
Though these civilizational diseases weren’t noticed in ancient peoples like the Maya, the Romans, the Chinese, the Egyptians, or Indians (Betlejewski, 2007). This implies that it’s something in our immediate environments—our obesogenic environments—which we have constructed for ourselves since the industrial revolution which then gave us the ability to over-consume highly processed carbs and other things not found in our natural diets that our ancestors evolved eating. There are also “astonishing [differences] in acne incidents between nonwesternized and fully modernized societies [that] cannot be solely attributed to generic differences among populations but likely results from differing environmental factors” (Cordain et al, 2002).
This also implies that our modern diets and lifestyles—our civilization— “may be depriving us of something our bodies require if we are able to be healthy” (Oschman, 2011). In fact, one of the biggest drivers of diseases of civilization is prolonged sitting (Chau et al, 2013; Biddle et al, 2016). It is correlated with numerous negative maladies, which could be alleviated if a person becomes physically active; even 30 minutes a day 5 days a week is enough stave off negative outcomes.
All of these are caused by what is termed the ‘environmental mismatch’, which Lieberman (2013) discusses in depth. The basic line of reasoning is this: we are evolved for our past environments, not any possible future ones. Our current lifestyle diseases and diseases of civilization are caused by sedentary activities along with highly processed food which we have not evolved to process correctly. What then follows are high rates of disease and mortality due to the lifestyle that our bodies cannot cope with.
Though some people, like JayMan, state that the rise of diseases or civilization are due to just simply living longer lives than hunter gatherers who had an average life expectancy of around 45 years of age. This hypothesis, however, has been rebutted for decades. The only thing that can explain the huge uptick in these diseases, along with their appearance in other societies which did not have these diseases until the introduction of our Westernized diet, is the built food environment which is full of process carbohydrates.
JayMan even says that “we don’t know what causes heart disease” but this is bullocks. We definitely know the cause, and it’s not dietary fat which has been believed since the 70s when dietary fat was demonized and carbohydrates were championed. What causes heart disease? Carbohydrates and decreased physical activity.
JayMan writes:
Contrary to what health experts might lead you to believe, fundamentally, we have no idea what causes heart disease.
This is straight bullshit. We have a great idea of what causes heart disease along with CVD (cardiovascular disease), it’s not dietary fat that causes heart disease—which I agree with JayMan on—but, and this goes with the theme of this article, carbohydrates:
Dr. Dariush Mozaffarian, dean of the Friedman School of Nutrition Science & Policy at Tufts University, who was not involved in the research, described the work as a well-controlled interventional study confirming that dietary refined carbohydrate is the primary driver of circulating saturated fatty acids in the blood stream.
“White bread, rice, cereals, potatoes, and sugars — not saturated fat — are the real culprits in our food supply,” he Mozzafarian [sic].
JayMan then takes another jab at the Look AHEAD trial, stating that diet and exercise did nothing to decrease the incidence of heart disease and mortality in obese subjects with type II diabetes and uses the trial as evidence that dieting and exercise doesn’t work. However, as I have noted in two replies to JayMan on this matter (Diet and Exercise: Don’t Do It? and Diet and Exercise: Don’t Do It? Part II), the results of Look AHEAD don’t rail against diet and exercise interventions for obese people with type II diabetes (Annuzzi et al, 2014). Keep in mind that type II diabetes is a mismatch disease and, clearly, changing the environment will change how many people are afflicted by type II diabetes.
Nevertheless, these problems are due directly to our sedentary lifestyles which stem from civilization and the types of foods we make and consume that then drive these diseases. JayMan then goes on to say that “the health beliefs that most people today are basically religion” and while I don’t disagree since the general population is clueless on nutrition science, this doesn’t hold for people who know their stuff and the causes of diseases of civilization.
Lieberman (2013: 169) writes:
There are many mismatch diseases, but all of them are caused by environmental changes that alter how the body functions. The simplest way to classify mismatch diseases is by how a given environmental stimulus has changed. Broadly speaking, most mismatch diseases occur when a common stimulus either increases or decreases beyond levels for which the body is adapted, or when the stimulus is entirely novel and the body is not adapted for it at all. Put simply, mismatches are caused by stimuli thst are too much, too little, or too new. For example, as cultural evolution transforms people’s diets, some mismatch diseases occur from eating too much fat, others from eating too little fat, and yet others from eating new kinds of fat that the body cannot digest (such as partially hydrogenated fats).
So clearly, with this knowledge, the easiest way to acquire a mismatch disease is migration into a new location. A good example is when light-skinned people migrate to more tropical climates and then get skin cancer. Their skin isn’t adapted for the strong UV rays coming from the sun.
Though the main driver for mismatch diseases is cultural evolution. Cultural evolution has outstripped Darwinian evolution through natural selection, and since we’ve not had time to adapt to these new ways of life, deleterious consequences soon followed. Lieberman (2013: 171) further writes:
In the absence of better information we can only hypothesize that many diseases, such as multiple sclerosis, attention deficit hyperactivity disorder (ADHD), and pancreatic cancer, as well as afflictions such as generalized lower back pain, are causes of evolutionary mismatch.
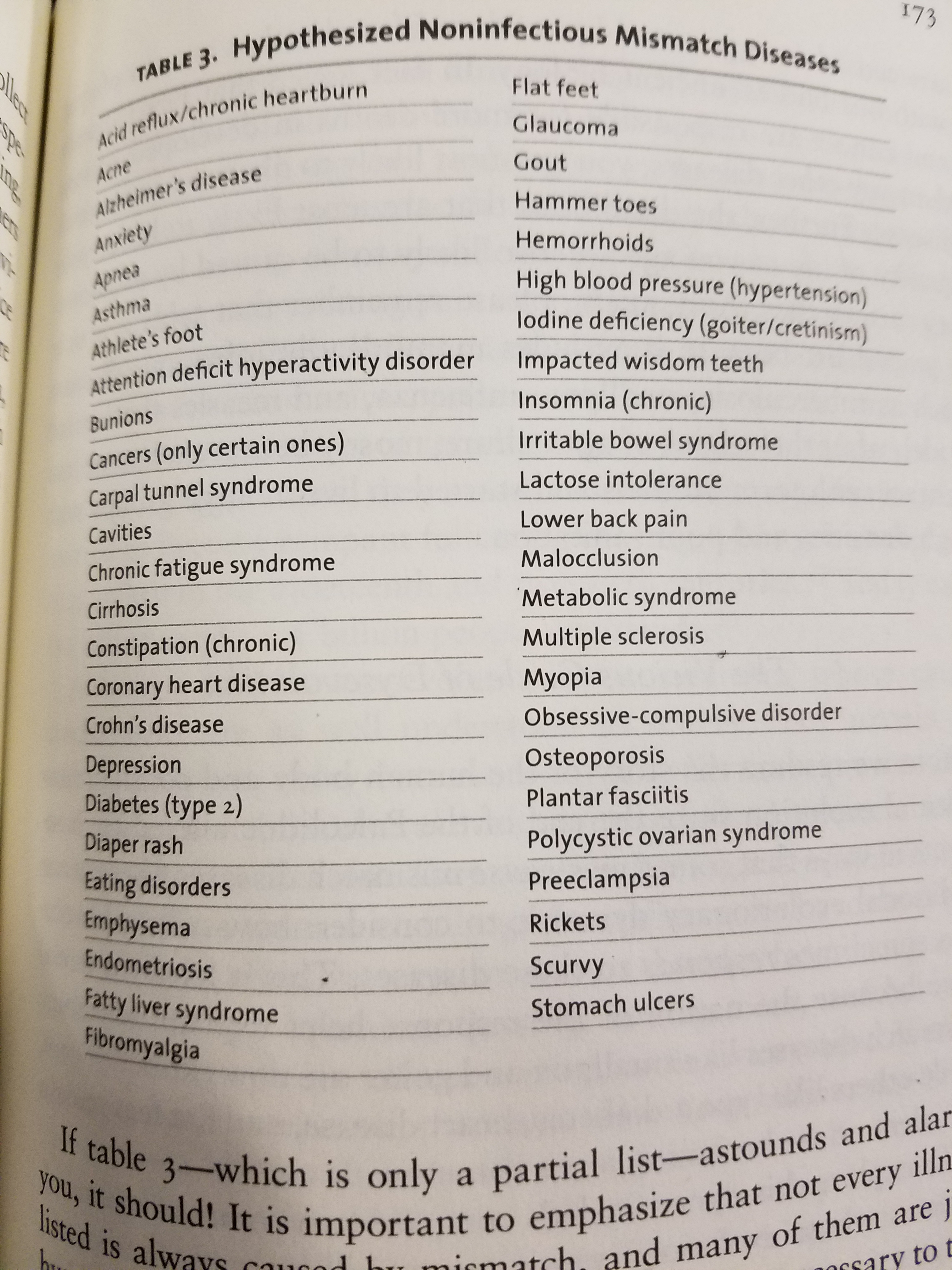
Above is table 3 from Lieberman (2013: 173). He notes hypothesized noninfectious mismatch diseases. Notice how most—if not close to all—are completely preventable with the right environmental interventions.
Though, of course, we have no idea what the health of our ancestors was like. But, as noted in the beginning of this article, since hunter-gatherers had extremely low to nonexistent cases of diseases that we have in first-world societies, that’s a huge clue that the environment we have constructed for ourselves (our obesogenic environment) directly contribute to the diseases we have today.
Finally, Jared Diamond asks an important question: “Is farming worth it?“. Of course he goes the Marxist route stating that “with agriculture came the gross social and sexual inequality, the disease of despotism, that curse our existence.” Though in my opinion what ‘curses our existence’ is the advent of farming that brought numerous mismatch diseases to humans which has decreased quality of life in first world countries.
In conclusion the advent of farming and society had good and bad things to it, though in my opinion—due to excess disease—it wasn’t really worth it. This is why I romanticize the hunter-gatherer’s diet. As shown in reports from the early 20th century, their disease burden (compared to ours) is low on nonexistent. This implies that what causes these mismatch diseases are differing environments from where our ancestors evolved and to stop these mismatches we must change our obesogenic environments and eat a more ‘natural’ diet (trying hard not to commit the naturalistic fallacy, but for this conversation it is apt). JayMan is wrong that mismatch diseases are caused by us living longer and that has been rebutted long ago. Most of what he writes in that article has to do with environmental mismatches.
The evidence that our built food environment with highly processed foods that drive these diseases is extremely compelling. Comparing hunter-gatherer societies with first-world societies leaves us a large clue that what drives these diseases are mismatches with our guilt environment. Only by changing the environment will we ameliorate these diseases and go back to living a relatively disease-free life.
This is why I romanticize the hunter-gatherer’s diet.
(12 22 17 Edit: Also see Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study by Dehghan et al, 2017 who write: “High carbohydrate intake was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an inverse association with stroke. Global dietary guidelines should be reconsidered in light of these findings.”
However, saturated fat consumption is not related to ischemic stroke. See Saturated Fat Consumption and Risk of Coronary Heart Disease and Ischemic Stroke: A Science Update by Nettleton et al, 2017 who write: “SAFA reduction had little direct effect on stroke risk. Cohort studies suggest that the food matrix and source of SAFA have important health effects.” Saturated fat consumption is also not linked to all cause mortality (de Souza et al, 2015). The PURE study buttresses my arguments that high processed carbohydrate intake have negative effects on all populations that consume them.)
Stress and Race Redux: A ‘Hispanic’ Paradox?
1500 words
American Renaissance published an article the other day titled “Is ‘Racism’ Killing Black People?” and, for the most part, I largely agree with it. However, there are a few faults in it that I need to address.
First, off, as the article rightly noted, it’s not only perceived ‘racism’ that is the cause for these health disparities, but stress from other blacks as well. Gregory Hood (the author of the AmRen article) cites a new study showing that blacks who move out of the ‘hood’ see a subsequent decrease in BP (Kershaw et al, 2017). They followed 2,290 people 974 were men and 1,306 were women. This is data collected from the CARDIA study which has helped us to understand racial disparities in all types of different health outcomes. Blacks who lived in high segregation neighborhoods had higher levels of SBP (systolic blood pressure), and saw a decrease in their SBP when they moved to less segregated neighborhoods. The authors conclude that “policies that reduce segregation may have meaningful health benefits.” What kind of policies will ‘reduce segregation’? Most races/ethnic groups group together in an area, so I don’t see how this would happen.
In regards to the argument on black maternal mortality and ‘racism’, I think it’s much more nuanced. Black women are 2 to 6 times more likely to die giving birth than white women; while the leading causes of maternal death in black women is pregnancy-induced hypertension, and embolism (Chang et al, 2003), though reasons for the mortality rate are not explainable at present (Flanders-Stepans, 2002). Further, in regards to preeclampasia, women who get pregnant at younger ages are more likely to acquire the disease while pregnant, and blacks and other non-whites are more likely to get pregnant at younger ages than whites (Main et al, 2015).
However, there are ways to reduce maternal mortality in black women. In a RCT undertaken between the years of 1990-2011 in Memphis, Tennesee, black women were followed with their live-in children and placed into one of four groups: “treatment 1 (transportation for prenatal care [n = 166]), treatment 2 (transportation plus developmental screening for infants and toddlers [n = 514]), treatment 3 (transportation plus prenatal/postpartum home visiting [n = 230]), and treatment 4 (transportation, screening, and prenatal, postpartum, and infant/toddler home visiting [n = 228])” (Olds et al, 2014). They conclude that pre- and post-natal care greatly reduces maternal/infant mortality in black women, “living in highly disadvantaged settings.”
Further, the racial disparity in post-term neonates is largely driven by “CHD among term infants with US-born mothers is driven predominately by the postneonatal survival disadvantage of African-American infants” (Collins et al, 2017). Though, as can be seen in the study by Olds et al (2014), pre- and post-natal care can greatly reduce both infant and maternal mortality.
Stress can also be measured in pregnant women by measuring the level of blood cortisol (Gillespie et al, 2017). They show that, independent of adulthood stress, stress during childhood may shape birth timing, with cortisol being the biological mediator. This may be an explanation for what Gregory Hood notes. He states in his article that there has to be an explanation for why black women birth earlier, and while I am sympathetic to biological models ala Rushton (1997), Gillespie et al (2017) drive a hard argument that stress during childhood using cortisol as a biological mediator makes a lot of sense.
There are a few studies that attest to pre- and post-natal care having a large effect on the morality of black women, and that having the carers being black women seems to have a positive effect (Guerra-Reyes and Hamilton, 2017). They conclude that “Recognition, support, and increasing the number of African-American midwives and birth assistants is vital in tackling health inequalities.” In regards to infant mortality rate (IMR), 18 states will achieve racial equality by 2050 if current trends from 1999-2013 hold (Joedrecka et al, 2017).
Now for the main reason I decided to write this: the ‘Hispanic’ paradox. This paradox is that for the past twenty years, ‘Hispanics’ with low SES have similar or better health outcomes than whites (Franzini, Ribble, and Keddie, 2001). However, more recent analyses show that the ‘Hispanic’ paradox does not exist, mostly due to methodological problems and migrant selectivity (Crimmins et al, 2007; Teruya and Bazargan-Hezeji, 2013) and was not noticed in Chile either (Cabiesies, Tunstall, and Pickett, 2013). There is no migrant selectivity in regards to smoking, however (Fenelon, 2013, 2016).
Teruya and Bazargan-Hezejie (2013) write:
Studies which advocate the validity of the Immigrant Paradox are countered by those which report specific, negative physical and mental health outcomes, and higher rates of substance use, especially among immigrant adolescents. Findings may also be compromised by fundamental methodological concerns such as migrant health selectivity, and approaches that consider only selectively healthy groups. Moreover, the Immigrant Paradox’s benefits do not appear to extend evenly and consistently to all races, ethnicities and subgroups. Similarly, the Hispanic Paradox does not protect consistently across all Latino ethnicities, age groups and genders, with Puerto Ricans and Cubans in particular found to enjoy fewer health advantages.
This is good evidence that the people who migrate to America are healthier, and that the symptoms of low SES show in their children, but not in them because they are a self-selected population. There is no ‘Hispanic’ paradox (Smith and Bradshaw, 2006; Schoenthaler, 2016). Even a new meta-analysis on this ‘paradox’ states “Immigrant children and youth suffer from an immigrant mortality disadvantage” (Shor, Roelfs, and Vamg, 2017).
Lastly, Gregory Hood brings up stress and suicide, stating that if blacks were really more stressed than whites then blacks would have higher rates of suicide, but some studies show that whites have a higher rate of suicidal ideation, while others do not show this (Perez-Rodriguez et al, 2010). Though, as Balis and Postolache (2010) show, studies show that while there is conflicting evidence in regards to racial/ethnic differences in suicide, whites still attempt it the most. However, suicide for young black Americans is on the rise. Ahmedani et al (2016) show that “Nearly 27% of White individuals made a mental health visit versus less than 20% of Asian, Hawaiian/Pacific Islander, and Black individuals in this period. Within 4 weeks, all visits and mental health visits remained most common for White individuals (67.3% and 47.4%, respectively) and least common among Asian individuals (52.8% and 31.9%, respectively). Within 52-weeks, more than 90% made any visit. Alaskan Native/Native American (81.5%) and White individuals (79.5%) made mental health visits 10–25% more often than other groups.” However, at least in Fulton County, Georgia, black suicide decedents were less likely to report depression than white suicide decedents (Abe et al, 2008).
However, for whites, as noted in this 1982 New York Times article, suicidal feelings “reflects feelings of loneliness and hopelessness, which can be greater factors as one grows older; for instance, after loved ones have died” whereas for older white men, loss of status may be a cause, which would not be that prevalent in lower SES ethnicities. The article seems to implicate loss of status as a main cause for higher rates of suicide in white Americans, and states that as other, lower SES ethnies attain higher status, that suicide rates would rise for them as well.
Another cause could be prescription drugs, for instance in the Northeast which has been hit hard by the opiate/heroin crisis which leads to more white deaths. Robert Putnam puts this on “the links between poverty, hopelessness and health” and states that the suicide rate has declined for two groups, black males and males over the age of 75. Further, “divorce, economic strain, or political repression are often characterized as suicide risks.” Cheng et al (2010) show that “A high level of identification with one’s ethnic group was associated with lower rates of suicide attempts.” So, it seems that if one keeps their status, and has a high level of identification with their ethnic group, whites would then be protected against suicidal ideation. Nonmetropolitan counties also have higher rates of suicide than metropolitan counties (Ivey-Stephenson et al, 2017). People who livee in rural counties are less likely to seek help for mental problems (Carpenter-Song and Snell-Rood, 2016). Whites are also more likely to live in rural areas. This could explain higher rates of suicide in whites, along with loss of status, depression and drug use.
In conclusion, the ‘Hispanic’ paradox doesn’t exist; whites attempt/commit suicide more due to loss of status and since most whites live in rural areas, they do not seek help for their mental health problems which then leads to suicide. In regards to black maternal mortality/infant mortality rates, if they have midwives present during and after the birth, mortality rates have decreased. If these trends continue, there will be racial equality in terms of maternal/infant mortality in 18 states. The AmRen article was good and well written, but there were a few huge flaws. The author assumed that since the ‘Hispanic paradox’ exists, that this should have one disregard the effects of, say, stress on blood pressure in black Americans, as I have discussed in the past. But since the ‘Hispanic’ paradox does not exist, then you cannot say that (perceived) discrimination and ‘racism’ is not a cause for higher rates of mortality in blacks compared to whites.
Blood Pressure, Stress, and the Social Environment: On Black-White Differences in Blood Pressure
1800 words
Blood pressure (BP) is a physiological variable. Therefore since it is a physiological variable then it can be affected by environmental and social changes. How do racial differences come into play here, for instance? Since blacks face more (perceived) discrimination, then they should, on average, have higher BP levels than whites. This is what we find—but the effect is mostly seen in low-income blacks. How do psychosocial factors come into play here in the black-white BP gap?
BP is regulated by cardiac output, vascular resistance of blood flow, blood volume, arterial stiffness, and, of course, the individual’s emotional state which can decrease or increase BP. Neural mechanisms also exist which regulate BP (Chopra, Baby, and Jacob, 2011). Knowing how and why BP increases or decreases will have us better understand the social contexts of increased BP in low SES blacks.
BP is a complex physiological trait. It can go up and down due to what occurs in the immediate environment. Values of 120/80 mmHg are cited as ‘average’ values, but we have no idea what an ‘average’ BP is. Nevertheless—like most/all physiological variables—there is a wide range of what is considered ‘normal’. Due to the variance in human physiological systems, what is ‘normal’ for one individual is not ‘normal’ for another. Variation in BP (like, say, 120 SBP (systolic blood pressure) to 140 SBP) is ‘normal’. I believe even around 110 for SBP is within that range. For DPB (diastolic blood pressure) between 75 and 90 is within normal diurnal fluctuations due to activity/eating/etc (Taylor, Wilt, and Welch, 2011). BP, like testosterone, is one of those tricky variables to measure and so must be measured upon waking to see if there are any problems. So even for a trait like BP, there seems to be a ‘normal range’.
About 33 percent of blacks have hypertension (HTN) (Peters, Arojan, and Flack, 2006). Urban blacks are more likely to have higher BP levels than whites, but “At present, there is no complete explanation for these differences and further research is required” (Lindhorst et al, 2007). Low SES is correlated with higher levels of BP in black Americans—especially those with darker skin—but not Africans in Africa (Fuchs, 2011), suggesting that this is an American phenomenon that needs to be addressed. One good explanation, in my view, is the social environment. Physiological traits are extremely malleable due to the need to be able to ‘change gears’ in an instant, for instance to either fight or flight. Though, in our modernized world, these responses—mostly—have no need and so (due to our supposed civilized behavior), one’s BP rises due to social stress and other environmental factors and it is due to the urban environment.
What is the cause of high BP in blacks?
One explanation that has been given to explain higher rates of BP in blacks when compared to whites is discrimination. However, studies show mixed evidence on whether or not so-called discrimination raises BP (Couto, Goto, and Bastos, 2012). The same American effect (American blacks having higher BP than American whites) is seen even in the UK London area (Agyemang and Bhopal, 2003). This, yet again, is more evidence that the social environment drives these differences—again, regardless of whether or not any of the discrimination is real or imagined. Say most of it were imagined: it’d be irrelevant because the imagined discrimination leads to very real physiological outcomes in BP.
The country of birth also has an effect on BP. In one study, it was noted that Africans had significantly higher BP when compared to Asians (which is identical/lower) and native French living in France (Bahous et al, 2015). Ethnic differences in BP increase due to similar sodium intake is lower than what is usually cited (Graudal and Jurgens, 2015). However, other authors have pointed out that basing conclusions off of observational studies have problems, like the estimation of sodium intake being inaccurate since it’s a one-time measure; (Gunn et al, 2013; Cobb et al, 2014)
There is also evidence—along with pathways—that show how certain social activities work to lower stress and BP, including participation at church (Livingstone, Devine, and Moore, 1991). Black Americans can make other lifestyle changes in order to decrease BP, such as exercise and other lifestyle interventions. Redman, Baer, and Hicks state that “gene-environment interactions, job-related stress, racism, and other psychosocial factors to racial/ethnic disparities” need to be explored as causes for higher rates of HTN in blacks compared to whites. And with the knowledge of how all physiological systems work in terms of stress and other factors, should be explored as causes for this disparity.
Grim et al (1990) state that factors that influence high BP in blacks compared to whites are inherited and that is the major source of variation between these populations. However, the other mounting social/physiological evidence deserves an explanation; that is not inherited, and what we know about how our physiology responds to stress and discrimination—whether real or imagined—are extremely important and lead to extremely real, and important, outcomes in these populations. It is also argued that since blacks en route to America during the slave trade died from salt-depletive diseases, that blacks with a higher genetic propensity to absorb salt survived and this is why blacks have a higher propensity to absorb salt and are more ‘salt-sensitive’, which also could explain higher rates of HTN in American blacks compared to their cousins in Africa (Wilson and Grim, 1991). However, Curtin (1992) disputes this because “There is no evidence that diet or the resulting patterns of disease and demography among slaves in the American South were significantly different from those of other poor southerners”.
However, in regards to the social environment, Williams (1992) drives one of the best arguments I have encountered in this literature so far, stating that while genetic factors play a small part in regards to the BP gap between blacks and whites, social factors are arguably more important than genetic ones (and with our homeodynamic physiology, this does make sense). Dressler (1990) for instance, argues that skin color is a proxy for both social class and discrimination and these factors explain a large amount of the variation. Psychosocial variables can also explain heightened BP (Marmot, 1985; Cuffee et al, 2014). Yan et al (2003) also note how “time urgency/impatience” and “hostility” “were associated with a dose-response increase in the long-term risk of hypertension.” Henry (1988) also argues that calcium, obesity and genetic factors cannot be the aetiology of HTN in blacks, while also proposing that high sodium intakes are due to psychosocial stress (Williams, 1992: 136).
Obesity also leads to hypertension (Re, 2009) while blacks are more likely to be obese than whites, however, black American men with more African ancestry are less likely to be obese (Klimentidis et al, 2016). This would imply that the greater amount of African ancestry in American blacks both protects against obesity and along with it HTN. Williams (1992) makes a convincing argument that environmental and social factors are the cause for the black-white BP gap. And while genetic factors are important, no doubt, environmental and social factors are arguably more important to this debate.
Kulkarni et al (1998) show that increased stress leads to subsequent BP elevations which, over time, will lead to HTN. In a 2009 meta-analysis, Gasparin et al show how “individuals who had stronger responses to stressor tasks were 21% more likely to develop blood pressure increase when compared to those with less strong responses.”
Further, in support for the ‘perceived stress’ hypothesis in regards to blacks ‘perceiving’ stress and discrimination, “stress denial in combination with abdominal obesity, alcohol consumption, and smoking may be proxy for a high stress level” (Suter et al, 1997). Carroll et al (2001) also show how there are is “modest support for the hypothesis that heightened blood pressure reactions to mental stress contribute to the development of high blood pressure.” Sparrenberger et al (2009) also did a systematic review of observational studies, finding that “Acute stress is probably not a risk factor for hypertension. Chronic stress and particularly the non-adaptive response to stress are more likely causes of sustained elevation of blood pressure.”
Lastly, Langford (1981) shows that when SES is controlled for, the black-white BP disparity vanishes, implying that social and environmental—not genetic—factors are the cause for elevated HTN levels in black Americans. Sweet et al (2007) showed that for lighter-skinned blacks, as SES rose BP decreased while for darker-skinned blacks BP increased as SES did while implicating factors like ‘racism’ as the ultimate causes. This is solid evidence that both skin color and SES are predictors of higher prevalence of BP in black populations, and since other studies show that this is not noticed in higher class blacks, nor is this noticed in blacks in Africa, then the main causes of this disparity are social and environmental in nature.
(Non, Gravlee, and Mulligan, 2012). Their study suggests that educating black Americans on the dangers and preventative measures of high BP will reduce BP disparities between the races. This is in-line with Williams (1992) in that the social environment is the cause for the higher rates of BP. One hypothesis explored to explain why this effect with education was greater in blacks than whites was that BP-related factors, such as stress, poverty and racial discrimination (remember, even if no racial discrimination occurs, any so-called discrimination is in the eye of the beholder so that will contribute to a rise in physiologic variables) and maybe social isolation may be causes for this phenomenon. Future studies also must show how higher education causes lower BP, or if it only serves as other markers for the social environment. Nevertheless, this is an important study in our understanding of how and why the races differ in BP and it will go far to increase our understanding of this malady. This is a very convincing argument that education and not genetic ancestry cause disparities in BP between blacks and whites.
WebMD states that, of course, both environmental and genetic factors are at play in regards to black’s increased propensity for acquiring HTN. Fuchs (2011) also states that “They [environmental and behavioral factors] could act directly or by triggering mechanisms of blood pressure increase that are dormant in blacks living in Africa” and explain why black Americans have higher rates of BP than Africans in Africa. Further, race and ethnicity are independent predictors of HTN (Holmes et al, 2013).
Conclusion
Blacks and whites do differ in BP, and its aetiology is both complex and hard to untangle Genetic factors probably don’t account for a lot of this variance since Africans in Africa have low levels of BP compared to their black American cousins. Numerous lines of evidence shows that social and environmental factors are the cause, and so to change this, all people—especially blacks—should be educated on how to change these problems in our society. Whether discrimination is real or imagined, the effects of it lead to real physiological outcomes that then lead to increased health disparities between these populations.
