
2650 words
One of the first things that pops into people’s minds when they hear about hunter-gatherers is most likely the myth of the ‘Noble Savage’—the belief that those who do not have civilization are ‘good’, whereas civilization corrupts Man. This myth, though, has been put to bed numerous times, like in Steven Pinker’s 2003 book The Blank Slate and more recently @EvolvingMoloch’s article Romanticizing the Hunter-Gatherer. (H/t to @EvolvingMoloch for the title.) However, I’m not too worried about claims about their ‘good nature’ from anthropologists; what I find much more interesting is their low rates of so-called diseases of civilization—diseases that seemed to appear after a society reaches a certain ‘tipping point’ if you will. These diseases that are prevalent in first-world societies are low to non-existent in these types of societies. Why?
All you need to do when thinking about the why of diseases of civilization is simple: think about the introduction of processed carbohydrates along with the introduction of a lot of high sugar, highly processed, high salt food. Though, people who do not eat these types of foods—especially on a societal level—do not have the same types of diseases that we have in the first-world. Since this seems to be true—that societies don’t have what I term ‘the Western scourge’, our Western diet—then it would seem that civilization had one negative effect on our lives, and that is the reason why I romanticize the hunter-gatherers’ diet.
My two main sources on diseases of civilization are Gary Taubes’ 2008 book Good Calories, Bad Calories and Daniel Lieberman’s 2013 book The Story of the Human Body: Evolution, Health, and Disease. Taubes’ book has a singular chapter—chapter 5—on diseases of civilization whereas Lieberman’s book goes much more in-depth on the hows and whys. Though Taubes’ whole book—along with his follow-up Why We Get Fat: And What to Do About It and his new book published in December of 2016 titled The Case Against Sugar—are pretty much critiques of the Western diet and explain the biochemical and physiological processes and reasons of how and why we get fat and how our first-world lifestyles are the cause of it. There are numerous testimonies from doctors from the early 19th century that attest to the great health and non-existent diseases that plague us in our societies.
The following are quotes from Taubes’ (2008) book Good Calories, Bad Calories:
In 1914, Hoffman himself had surveyed physicians working for the Bureau of Indian Affairs. “Among some 63,000 Indians of all tribes,” he reported, “there occurred only 2 deaths from cancer as medically observed from the year 1914.” (Taubes, 2008: 92)
“There are no known reasons why cancer should not occasionally occur among any race of people, even though it be below the lowest degree of savagery and barbarism,” Hoffman wrote. (Taubes, 2008: 92)
“Granting the practical difficulties of determining with accuracy the causes of death among the non-civilized races, it is nevertheless a safe assumption that the large number of medical missionaries and other trained medical observers, living for years among native races throughout the world, would long ago have provided a substantial basis of fact regarding the frequency of malignant disease among the so-called “uncivilized” races, if cancer were met with among them to anything like the degree common to practically all civilized countries. Quite the contrary, the negative evidence is convincing that in the opinion of qualified medical observers cancer is exceptionally rare among the primitive peoples.” (Taubes, 2008: 92)
These reports, often published in the British Medical Journal, The Lancet or local journals like the East African Medical Journal, would typically include the length of service the author had undergone among the natives, the size of the local native population served by the hospital in question, the size of the local European population, and the number of cancers involved in both. F.P. Fouch, for instance, district surgeon of the Orange Free State in South Africa, reported to the BMJ in 1923 that he had spent six years at a hospital that served fourteen thousand natives. “I never saw a single case of gastric or duodenal ulcer, colitis, appendicitis, or cancer in any form in a native, although these diseases were frequently seen among the white or European population.” (Taubes, 2008: 92)
As a result of these modern processed foods, noted Hoffman, “far-reaching changes in bodily functioning and metabolism are introduced which, extending over many years, are the causes or conditions predisposing to the development of malignant new growths, and in part at least explain the observed increase in cancer death rate of practically all civilized and highly urbanized countries.” (Taubes, 2008: 96)
Is it any coincidence that these diseases are so prevalent in European populations but not hunter-gatherer’s? I think not.
The same has been noted with the Pima Indians: before the introduction of the scourge we call a ‘diet’, they had low to non-existent rates of obesity and other types of metabolic diseases. Then, when our diet made its way to their societies, their lives changed:
For perhaps two millenia, the Pima have lived as both hunter-gatherers and agriculturalists. Game was abundant in the region, as were fish and clams in the Gila River. When the Jesuit missionary Eusebio Kino arrived among the Pima in 1787, the tribe was already raising corn and beans on fields irrigated with Gila River water. In the decades that followed, they took to raising cattle, poultry, wheat, melons, and figs. They also ate mesquite beans, the fruit of the saguaro cactus and a mush of what Russell later called “unidentified worms.” In 1846, when a U. S. Army battalion passed through Pima lands, the battalion’s surgeon John Griffin describes the Pima as “sprightly” and in “fine health.” He also noted that the Pima has “the greatest abundance of food, and take care of it well, as we saw many of their storehouses full of pumpkins, melons, corn, etc.” (Taubes, 2007: 237)
Hrdlicka also noted that by 1905 the Pima diet already included “everything obtainable that enters into the dietary of the white man,” which raises the possibility that this might have been responsible for the obesity. (Taubes, 2007: 238)
Obesity and diabetes (diabesity) was low to nonexistent in the Pima and perhaps the only reason for this was that they did not live off of highly processed carbohydrates and other Western foods. When these foods were introduced to these people, then the modern diseases of civilization then appeared.
This is noticed everywhere the Western diet goes. This is even occurring in China, which had historically low rates of obesity. However with the introduction of the Western ‘diet’, this is now changing. China now has the largest overweight population in the world, along with the largest number of obese children in the world. Another coincidence?
Though these civilizational diseases weren’t noticed in ancient peoples like the Maya, the Romans, the Chinese, the Egyptians, or Indians (Betlejewski, 2007). This implies that it’s something in our immediate environments—our obesogenic environments—which we have constructed for ourselves since the industrial revolution which then gave us the ability to over-consume highly processed carbs and other things not found in our natural diets that our ancestors evolved eating. There are also “astonishing [differences] in acne incidents between nonwesternized and fully modernized societies [that] cannot be solely attributed to generic differences among populations but likely results from differing environmental factors” (Cordain et al, 2002).
This also implies that our modern diets and lifestyles—our civilization— “may be depriving us of something our bodies require if we are able to be healthy” (Oschman, 2011). In fact, one of the biggest drivers of diseases of civilization is prolonged sitting (Chau et al, 2013; Biddle et al, 2016). It is correlated with numerous negative maladies, which could be alleviated if a person becomes physically active; even 30 minutes a day 5 days a week is enough stave off negative outcomes.
All of these are caused by what is termed the ‘environmental mismatch’, which Lieberman (2013) discusses in depth. The basic line of reasoning is this: we are evolved for our past environments, not any possible future ones. Our current lifestyle diseases and diseases of civilization are caused by sedentary activities along with highly processed food which we have not evolved to process correctly. What then follows are high rates of disease and mortality due to the lifestyle that our bodies cannot cope with.
Though some people, like JayMan, state that the rise of diseases or civilization are due to just simply living longer lives than hunter gatherers who had an average life expectancy of around 45 years of age. This hypothesis, however, has been rebutted for decades. The only thing that can explain the huge uptick in these diseases, along with their appearance in other societies which did not have these diseases until the introduction of our Westernized diet, is the built food environment which is full of process carbohydrates.
JayMan even says that “we don’t know what causes heart disease” but this is bullocks. We definitely know the cause, and it’s not dietary fat which has been believed since the 70s when dietary fat was demonized and carbohydrates were championed. What causes heart disease? Carbohydrates and decreased physical activity.
JayMan writes:
Contrary to what health experts might lead you to believe, fundamentally, we have no idea what causes heart disease.
This is straight bullshit. We have a great idea of what causes heart disease along with CVD (cardiovascular disease), it’s not dietary fat that causes heart disease—which I agree with JayMan on—but, and this goes with the theme of this article, carbohydrates:
Dr. Dariush Mozaffarian, dean of the Friedman School of Nutrition Science & Policy at Tufts University, who was not involved in the research, described the work as a well-controlled interventional study confirming that dietary refined carbohydrate is the primary driver of circulating saturated fatty acids in the blood stream.
“White bread, rice, cereals, potatoes, and sugars — not saturated fat — are the real culprits in our food supply,” he Mozzafarian [sic].
JayMan then takes another jab at the Look AHEAD trial, stating that diet and exercise did nothing to decrease the incidence of heart disease and mortality in obese subjects with type II diabetes and uses the trial as evidence that dieting and exercise doesn’t work. However, as I have noted in two replies to JayMan on this matter (Diet and Exercise: Don’t Do It? and Diet and Exercise: Don’t Do It? Part II), the results of Look AHEAD don’t rail against diet and exercise interventions for obese people with type II diabetes (Annuzzi et al, 2014). Keep in mind that type II diabetes is a mismatch disease and, clearly, changing the environment will change how many people are afflicted by type II diabetes.
Nevertheless, these problems are due directly to our sedentary lifestyles which stem from civilization and the types of foods we make and consume that then drive these diseases. JayMan then goes on to say that “the health beliefs that most people today are basically religion” and while I don’t disagree since the general population is clueless on nutrition science, this doesn’t hold for people who know their stuff and the causes of diseases of civilization.
Lieberman (2013: 169) writes:
There are many mismatch diseases, but all of them are caused by environmental changes that alter how the body functions. The simplest way to classify mismatch diseases is by how a given environmental stimulus has changed. Broadly speaking, most mismatch diseases occur when a common stimulus either increases or decreases beyond levels for which the body is adapted, or when the stimulus is entirely novel and the body is not adapted for it at all. Put simply, mismatches are caused by stimuli thst are too much, too little, or too new. For example, as cultural evolution transforms people’s diets, some mismatch diseases occur from eating too much fat, others from eating too little fat, and yet others from eating new kinds of fat that the body cannot digest (such as partially hydrogenated fats).
So clearly, with this knowledge, the easiest way to acquire a mismatch disease is migration into a new location. A good example is when light-skinned people migrate to more tropical climates and then get skin cancer. Their skin isn’t adapted for the strong UV rays coming from the sun.
Though the main driver for mismatch diseases is cultural evolution. Cultural evolution has outstripped Darwinian evolution through natural selection, and since we’ve not had time to adapt to these new ways of life, deleterious consequences soon followed. Lieberman (2013: 171) further writes:
In the absence of better information we can only hypothesize that many diseases, such as multiple sclerosis, attention deficit hyperactivity disorder (ADHD), and pancreatic cancer, as well as afflictions such as generalized lower back pain, are causes of evolutionary mismatch.
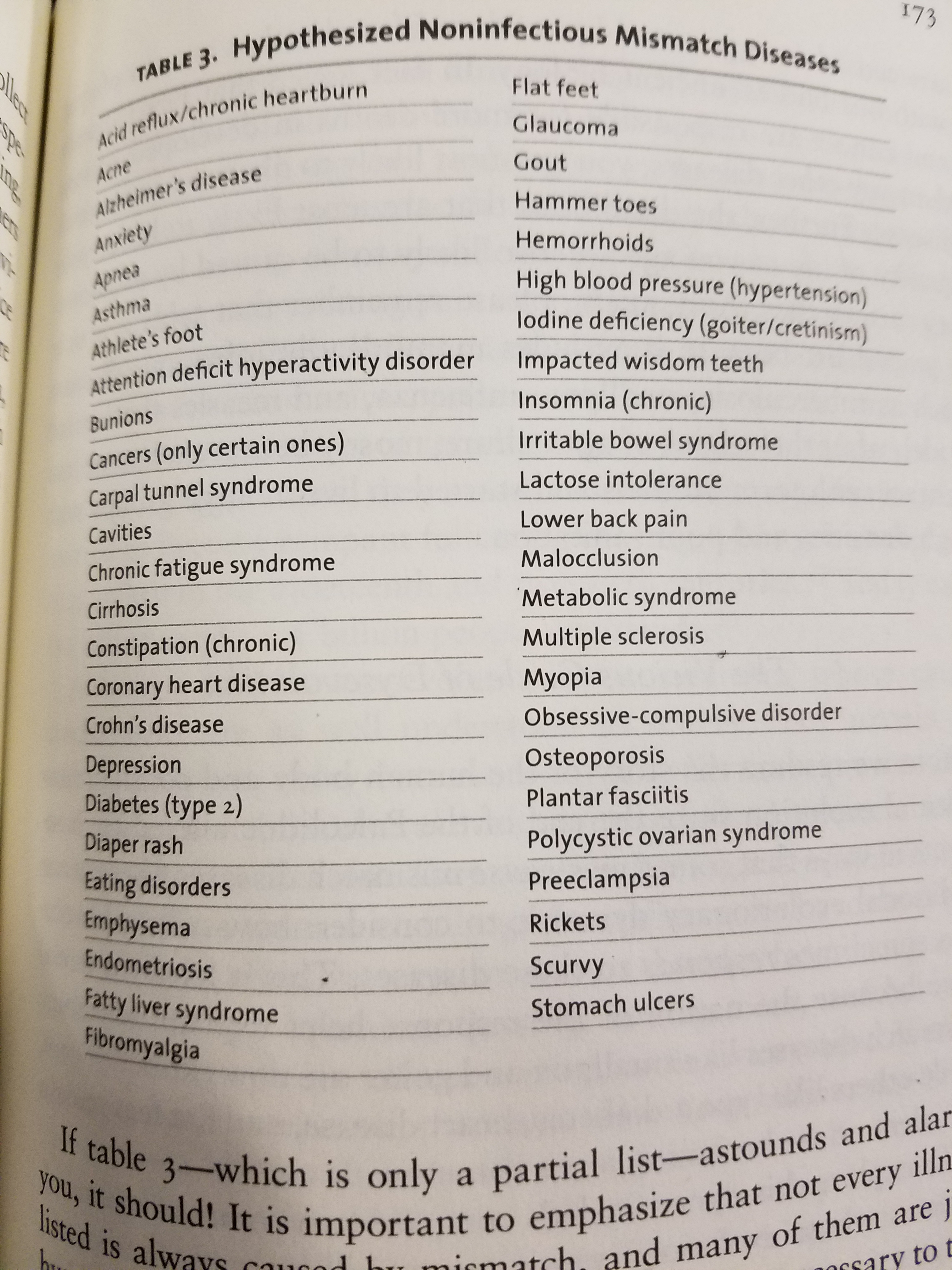
Above is table 3 from Lieberman (2013: 173). He notes hypothesized noninfectious mismatch diseases. Notice how most—if not close to all—are completely preventable with the right environmental interventions.
Though, of course, we have no idea what the health of our ancestors was like. But, as noted in the beginning of this article, since hunter-gatherers had extremely low to nonexistent cases of diseases that we have in first-world societies, that’s a huge clue that the environment we have constructed for ourselves (our obesogenic environment) directly contribute to the diseases we have today.
Finally, Jared Diamond asks an important question: “Is farming worth it?“. Of course he goes the Marxist route stating that “with agriculture came the gross social and sexual inequality, the disease of despotism, that curse our existence.” Though in my opinion what ‘curses our existence’ is the advent of farming that brought numerous mismatch diseases to humans which has decreased quality of life in first world countries.
In conclusion the advent of farming and society had good and bad things to it, though in my opinion—due to excess disease—it wasn’t really worth it. This is why I romanticize the hunter-gatherer’s diet. As shown in reports from the early 20th century, their disease burden (compared to ours) is low on nonexistent. This implies that what causes these mismatch diseases are differing environments from where our ancestors evolved and to stop these mismatches we must change our obesogenic environments and eat a more ‘natural’ diet (trying hard not to commit the naturalistic fallacy, but for this conversation it is apt). JayMan is wrong that mismatch diseases are caused by us living longer and that has been rebutted long ago. Most of what he writes in that article has to do with environmental mismatches.
The evidence that our built food environment with highly processed foods that drive these diseases is extremely compelling. Comparing hunter-gatherer societies with first-world societies leaves us a large clue that what drives these diseases are mismatches with our guilt environment. Only by changing the environment will we ameliorate these diseases and go back to living a relatively disease-free life.
This is why I romanticize the hunter-gatherer’s diet.
(12 22 17 Edit: Also see Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study by Dehghan et al, 2017 who write: “High carbohydrate intake was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an inverse association with stroke. Global dietary guidelines should be reconsidered in light of these findings.”
However, saturated fat consumption is not related to ischemic stroke. See Saturated Fat Consumption and Risk of Coronary Heart Disease and Ischemic Stroke: A Science Update by Nettleton et al, 2017 who write: “SAFA reduction had little direct effect on stroke risk. Cohort studies suggest that the food matrix and source of SAFA have important health effects.” Saturated fat consumption is also not linked to all cause mortality (de Souza et al, 2015). The PURE study buttresses my arguments that high processed carbohydrate intake have negative effects on all populations that consume them.)

So I got a buddy who thinks you could eat anything you wanted(McDonalds,sweets etc) to at least once a week and you will not suffer any unhealthy repercussions. Is this true?
LikeLike
Yes. Moderation is OK, but excess isn’t. I follow the 80/20 rule: 80 percent of my diet on point with 20 percent ‘junk food’ though it’s mostly 90/10 whole food/junk food. And if it’s within reason.
Have you ever seen the documentary Supersize Me? The guy eats nothing but McDonald’s for a month and his sex drive lowered, he gained a lot of weight and had horrible blood markers.
There are great arguments that the hunter-gatherer’s diet should be romanticized, we’d then be ameliorating numerous diseases and other maladies brought on by our obesogenic environments.
LikeLike
Yeah, stop romanticising, and start looking at fields other than yours.
https://www.biorxiv.org/content/early/2017/06/02/145193
If anything, we’re getting healthier and healthier.
LikeLike
Thanks for the paper. I’ll read it tonight and respond in full.
So, we’re getting healthier and healthier, is this why obesity and metabolic diseases like type II diabetes is increasing in the first world? Why are we getting sicker and sicker, fatter and fatter? Why do we have so many diseases that are absent in hunter gatherer populations? Buy the books I cited and read them because that’s what I based my arguments off, not neanderthals. (Though I’m hesitant to accept that because genes aren’t destiny. Just because you have a certain ‘gene for’ X doesn’t mean that you’ll get X.)
LikeLike
This has nothing to do with Neanderthals.
They explicitly compared Hunter Gatherers, the First Farmers, Indo-European Pastoralists and Modern peoples.
Why all of these diseases? I blame ‘diversity’ increasing the statistics – not that I deny that are malign food.
LikeLike
Good read. But 1) genes aren’t destiny. 2) genes wouldn’t necessarily do the same things in different environments. 3) the GRS (genetic [disease] risk scores) are also not deterministic. I waited the whole paper to read this. From the last page:
We note that genomic health does not necessarily equate to phenotypic health. Genetic risk scores are not deterministic, instead they merely indicate whether an individual has a predisposition to a particular disease. In addition, alleles that contribute to disease in modern environments may not have had the same effects in past environments.
Someone could be ‘genetically predisposed’ to be an alcoholic but if they never drink alcohol will they become an alcoholic?
A new paper was published in Cell, this year that said that “many GWAS hits have no specific biological relevance to disease and wouldn’t serve as good drug targets. Rather, these ‘peripheral’ variants probably act through complex biochemical regulatory networks to influence the activity of a few ‘core’ genes that are more directly connected to an illness.”
See Boyle and Pritchard (2017): An Expanded View of Complex Traits: From Polygenic to Omnigenic
The paper doesn’t undermine what was written. Surely you’re aware of what is cited above
So the uptick in diseases of civilization is due to immigration, not just our obesogenic environments? You’re wrong.
LikeLike
there’s no romanticizing the diet, because the diet is more than its composition.
the diet is also so many calories vs level of physical activity.
savages sometimes fast out of laziness rather than out of necessity. because for them getting food requires physical exertion.
read dan everett’s book.
and smoke toad.
LikeLike
The diet is more than the number of calories.
CICO?
Or they can’t find food. And it’s fine. There’s nothing wrong with fasting.
What’s it called.
LikeLike
everett’s book is mostly about linguistics.
Don’t sleep, there are snakes: life and language in the Amazonian jungle (2008). Pantheon Books, New York.
LikeLike
savages lived as long or longer (and in better health) than farmers or pastoralists…
until vaccines and antibiotics./
now savages have a much lower life expectancy than civilized people.
and this is NOT due to higher infant mortality.
that’s another myth propagated by morons like jayman.
savages die from infectious diseases at all ages.
but there are plenty of very old savages, and they don’t suffer from atherosclerosis or cancer or diabetes or whatever.
one possibility is that they don’t suffer from these diseases precisely because they are always infected with something…
and they ARE always chock-a-block infected…with something…including worms.
in which case the prevention is worse than the disease.//
LikeLike
of course i could never adopt the paleo diet.
it used to be called “the drinking man’s diet”.
that’s my diet.
but drinking is very UN-paleo.
LikeLike