
Dorothy Roberts on Race as a Political Entity
2050 words
I recently bought Dorothy Roberts’ Fatal Invention: How Science, Politics and Big Business Re-create Race in the Twenty-First Century (2011) (it was $1.99 in the nook store, couldn’t pass it up), which, how the title of the book explains, discusses how race is recreated today using methods of the past as well as methods of the future. One of her main claims is that race is a political entity. Now, while I don’t disagree here (there are of course social aspects to what we call “races”), she completely rides against biological racial realism (eg Spencer, 2014; Hardimon, 2017). Her concept, though, is similar to Hardimon’s (2017) socialrace concept, and it is already a part of Spencer’s Blumenbachian partitions (since race is both biologically and socially constructed in the American view of race). While I do not believe that you need genes to delineate race, Roberts also goes on the attack on Rosenberg et al (2002), who both Hardimon and Spencer cite to buttress their arguments on the reality of biological races.
Race is not a biological category that is politcally charged. It is a political category that has been disguised as a biological one. (Roberts, 2011: 14)
Note how this is extremely similar to Hardimon’s socialrace concept. In Hardimon’s concept, socialraces have a biological correlate: minimalist races. Hardimon’s concept says, for example, that “Hispanics/Latinos” are socialraces but they are a group that do not have a corresponding minimalist race—because “Hispanics/Latinos” are a mixture of different races. Race IS a biological category that has been politically charged: Groups look different; groups that look different share geographic ancestry; groups that look different that share geographic ancestry are derived from the same geographic location; therefore race is a biological category and is therefore politically charged (one reason) since people do not like the out-group—people that look different from themselves.
This distinction is important because many people misinterpret the phrase “race is socially constructed” to mean that the biological category of race has a social meaning, so that each society interprets differently what is means to belong to a biological race. According to this view, first we are born into a race, and then our society determines the consequences of this natural inheritance. There is, then, no contradiction between seeing race as both biological and socially constructed. (Roberts, 2011: 14)
There, actually, IS NO CONTRADICTION between seeing race as socially and biologically constructed. Racial categories pick out real kinds in nature—which is what “biological racial realism” means. Since our racial categories pick out real kinds in nature, then, when it comes to society and social construction, whatever is believed about certain races in that society will be socially constructed. You can’t, for example, call a Nigerian Caucasian (see more on this below) because it does not make any sense.
Roberts then goes on (p. 14-15) about how “human beings do not fit the zoological definition of race” since a “biological race is a population of organisms that can be distinguished from other populations in the same species based on differences in inherited traits.” And so, since no human groups have this high degree of genetic differentiation, there are no human races, but only one human race.
Though Hardimon (2017: 99) articulates the best definition of race I have come across:
A race is a subdivision of Homo sapiens—a group of populations that exhibits a distinctive pattern of genetically transmitted phenotypic characters that corresponds to the group’s geographic ancestry and belongs to a biological line of descent initiated by a geographically separated and reproductively isolated founding population.
So we know that (1) populations exhibit distinctive features; (2) these populations that exhibit these distinctive features correspond to that population’s geographic ancestry, (3) these populations that exhibit these distinctive features which correspond to geographic ancestry belong to a biological line of descent which was initiated by reproductive isolated and geographically separated founding populations; so (4) race exists.
We know race is a political grouping because it has its political roots in slavery and colonialism, it has served its political function over the four hundred years since its inceptio, and its boundary lines—how many there are and who belongs to each one—have shifted over time and across nations to suit those political purposes. Who qualifiies as white, black, and Indian has been the matter of countless rule changes and judicial decisions. These racial reclassifications did not occur in response to scientific advances in human biology, but in response to sociopolitical imperatives. They reveal that was is being defined, orgainzed, and interpreted is a political relationship and not an innate classification. (Roberts, 2011: 15)
We can take this two ways here: (1) point out that Roberts is conflating minimalist/populationist races with socialraces (which is exactly what she is describing to the tee). Yes, since race is partly social, then, based on the social attitudes of people which do change over time. Then, in that society, certain groups who were barred from being in another group may be allowed “into” the group. This does not mean that race is not biological. “Oh the Irish were considered “not white” at one point in time, therefore race doesn’t exist since groups can exit group A and become group B based on sociopolitical inclinations.” This, of course, goes over the distinctive phenotypic differences between groups with peculiar geographic ancestry. THAT is what defines race; what Roberts is discussing is important, since race is partly political, but it is not the whole story.
In addition to the grotesque lynchings that terrorized blacks throughout the South, an especially brutal form of reenslavement was the false imprisonment of thousands of black men who were then leased to white farmers, entrepreneurs, and corporations as a source of cheap labor.
It is in this accute distinction that between the political status of whites and blacks, this way of governing the power relationship between them, that we find the origins of race. Colonial landowners inherited slavery as an ancient practive, but they invented race as a modern system of power. They employed Aristotle’s concept of natural slaves and natural rulers to define permanent features of black and white people. Race separated human beings into two fundamentally distinct groups: those who were indelibly born to be lifelong servants and those who were born to be their masters. Race radically transformed not only what it meant to be enslaved, but what it meant to be free. (Roberts, 2011: 23)
Let’s accept Roberts’ argument here that the political status of whites and blacks was a way to govern the power relationship between them: so what? That group A subjugated group B and attempted to justify it with X, Y, and Z doesn’t mean that group A and group B are not biological races—it just means that group A subjugated group B and, in the future, there were social repercussions (which is also a part of the phenomenon of race as a partly social construct).
Roberts then discusses the Census (p. 31-35) and how ever-changing racial definitions undermine the claim that biological racial realism is true. In Spencer’s argument, the US meaning of “race” is just a referent, “specifically the referent of US racial discourse” (Spencer, 2014: 1027). This is because, in America, race-talk is tied to the census. We Americans are familiar with the racial groupings on the census since they are not only in use on the census but numerous other institutions. Spencer (2014) then discusses how we can use “phonetic cues alone (e.g., African American Vernacular English), surnames alone (e.g., “Chen”), first names alone (e.g., “Lakisha”), and visual cues alone (e.g., a person’s face)” (Spencer, 2014: 1027) to know someone’s race. Therefore, according to Spencer, the discourse used in the census is the discourse used nation-wide.
But the census does not set what “race” means on these forms: the OMB (Office of Management Budgeting) does. The OMB refers to race as a “set” of populations, and so this leads Spencer to believe that the “sets” of populations that the OMB is referring to are whites, blacks, Asians, Pacific Islanders, and American Indians. So race is a particular, not a kind as Hardimon argues.
Roberts then argues against the “new racial science”, most forcefully, against Rosenberg et al (2002). She brings up the usual discourse “…the number of genetic clusters is dictated by the computer user, not the computer program” (Roberts, 2011: 74). Roberts says that the clusters are “arbitrary.” Roberts says that Rosenberg et al’s (2002) study failed to verify 18th-century racial typology, but it did confirm what we have known since Lewontin’s (1972) analysis: that there is more genetic variation within races than between them. About 93-95 percent of human genetic variation was found to be within race whereas 5-7 percent of human genetic variation was found to be between groups.
Roberts says that the clusters are “arbitrary.” This is a common critique, but it is irrelevant. The five populations found by Structure are genetically structured—they are meaningfully demarcated on the basis of genetic markers (Hardimon, 2017: 88). Roberts also discusses the K = 6 run, which identified the Kalash people.
The fact that structure represents a population as genetically distinct does not entail that the population is a race. Nor is the idea that populations corresponding to the five major geographic areas are minimalist races undercut by the fact that structure picks out the Kalash as a genetically distinct group. Like the K=5 graph, the K=6 graph shows that modulo our assumption, continental-level races are genetically structured” (Hardimon, 2017: 88).
The five clusters identified by Rosenberg et al (2002) represent continental-level minimalist races so the five populations which correspond to the major geographic locations throughout the world are continental-level minimalist races. So it is, in fact, possible to place individuals into different their continental-level minimalist race without knowing anything about the race or ancestry of the individuals from which the microsatellites were drawn. Rosenberg et al (2002) studied the populations based on language, culture, and geography, not skin color or race.
It is true that Rosenberg et al (2002) found 4.3 percent of the overall human genetic variation to be between races—but this does not ride against claims from biological racial realists. The genetic variation is enough to say that we have partitions at K = 5.
“People are born with ancestry that comes from their parents but are assigned a race” is how Camara Jones, a research director at the Centers for Disease Control (CDC) explains it. (Roberts, 2011: 77)
People are assigned races based on the ethnicity/ancestry of the parents. A Nigerian would not be assigned to the Asian race, since the Nigerian has none of the features which make “Asians” Asian.
This is very simple: if both parents belong to race R, then the child will be race R as well. If parent 1 belongs to R1 and so does parent 2, then the child will belong to R1 as well (since the parents have distinct physical features which correspond with geographic ancestry and their ancestors derived from a distinct geographic location. So, since people are born with ancestry that comes from their parents, then they are assigned their PARENT’S race; they are not assigned A race, as if one can assign any individual to any race. But what if one parent belongs to R1 and the other belongs to R2? Hardimon’s minimalist concept is vague here; it only shows that races exist, it does not say which populations are races. If an individual’s parents belong to R1 and R2, then that individual is mixed race. The existence of mixed race people, of course, does not rail against the existence of biological races.
In sum, Roberts does make some good points (in what I have read of the book so far), but she gets it wrong on race. Hardimon and Spencer have both defended the methodology/concepts used by Rosenberg et al (2002) and in doing so, they successfully argued for the existence of biological races—though their two viewpoints differ. That race is, in part, socially (politically) constructed is irrelevant. What Roberts does not understand is that these socially constructed groups (“white”, “black”) still, very much so, capture biological differences between them. That they are socialraces does not mean that they DO NOT have different physical features which correspond to geographic ancestry. The socialrace concept (which Roberts espouses in her book) is separate from Hardimon’s other scientific race concepts. But it is already inherent in Spencer’s, since his Blumenbachian partitions are social constructs of a biological reality. You don’t need genes to delineate races and minimalist races exist and are biologically real.
(I will cover other things from her book as I get to them. I will discuss race and medicine at length.)
Just-So Stories: The Slavery Hypertension Hypothesis
1800 words
Blacks have higher BP on average than whites. Why? One popular explanation is the Slavery Hypertension Hypothesis (SHH). The SHH is a hypothesis which posits 2 things: (1) that those living in the African climate were subject to limited water and salt, and dehydration so, a higher sodium-retention mechanism evolved in those populations to retain salt, which also leads to hypertension; and (2) during the Middle Passage there were high amounts of vomiting, diarrhea, heat, and little salt and so surviving slaves were “selected for” salt conserving water and salt. Then, when they reached the plantations, due to low water, copious sweating, and intense work, there were additional selective pressures which “selected for” water and salt conservation.
This hypothesis is so popular, that it was even pushed by Oprah, when Dr. Mehmet Oz asked Oprah why blacks have higher BP than whites. Lujan and DiCarlo (2018) write:
During a May 2007 Oprah show, Dr. Mehmet Oz asked Oprah, “Do you know why African-Americans have high blood pressure?” Oprah promptly replied that Africans who survived the slave trade’s Middle Passage “were those who could hold more salt in their bodies.” To which Dr. Oz exclaimed, “That’s perfect!” (64, 71). According to Dr. Oz and Oprah, African-Americans today are afflicted by hypertension at higher rate than whites because of genes passed on by their ancestors, genes that favored salt retention and that, in turn, cause high blood pressure (Fig. 1) (71). [They are implying that genetic ancestry is associated with BP; see below.]
Lujan and DiCarlo (2018) state that when individuals were “salt-loaded”, normal salt-resistant individuals retained just as much sodium in their bodies as salt-sensitive individuals. Salt-resistant individuals retain as much salt as salt-sensitive individuals—but they did not develop hypertension.
Furthermore, available evidence suggests that the difference in salt-sensitivity between African-Americans and Caucasians (European-Americans) is significantly smaller than what the Slavery Hypertension Hypothesis suggests. In fact, Chrysant and colleagues (14) were unable to find differences in the blood pressure response to salt by race, age, sex, or body weight. Thus salt sensitivity is not a racial problem, but rather a human problem, and the generalization that blacks are salt sensitive and whites are not should be discarded (14). It is important to note that measurements of salt retention in humans have come into serious question (50).
The hypothesis, as explained above, explains the data it purports to explain and only the data it purports to explain and is, therefore, a just-so story. Using the definition from Sterelny and Griffiths (1999: 61), a just-so story is “an adaptive scenario, a hypothesis about what a trait’s selective history might have been and hence what its function may be.”
So, the just-so story goes, that Africans in Africa—and those who survived the Middle Passage—had genes which favored better salt retention, and so, they were “selected for” which lead to an increased chance of survival in the low-salt, low-water, high-heat environment. The hypothesis is clearly ad hoc – notice that African-descended people have higher rates of blood pressure and then work backward. What in their recent or past history, could have lead to these high rates of hypertension in today’s societies.
This method is the usual EP reverse engineering method—strongly criticized by philosophers of science Robert Richardson (2007) and David Buller (2005)—which is “the inference from function to cause” (Richardson, 2007: 51). The just-so storytellers then work backward from a data point and “reason” how the trait became fixated in a particular population. So the formulators of the SHH wanted to infer function from cause—what the function of higher African BP was.
So the just-so story in question was formulated, which leads to genetic essentialist and determinist views—that genes are “causing” and were “selected for”—to explain the data they wanted to explain. But it makes no testable predictions, so it’s a just-so story. The hypothesis is inherently ad hoc—the “justification” for the hypothesis was reasoned backward from a fact we know today—that blacks have higher BP—and the “speculation” was provided as if it were true—which has permeated into the media, as can be seen above.
There are more sensible explanations for differences in hypertension between blacks and whites (I use those terms since they are socialraces). Genetic determinists would always go to the genes as an explanation for differences in any trait X. However, there is no reason to posit genetic differences between population groups as evidence for the differences in the causes of the trait in question. There are more sensible explanations for the BP disparity between blacks and whites.
Williams (1992) cites social factors as much more important than genetic factors in the etiology of hypertension – stress, social support, coping patterns, health behavior, sodium, calcium, and potassium consumption, alcohol consumption, and obesity. Citing these environmental factors that raise BP is critical—the human body’s physiology is adaptive and so, it can adapt to differing environments based on the reactions of the individual in that environment. This, of course, holds for nutrition as well. Nutrition most definitely affects BP – nutrition also affects rates of obesity (obviously). Blacks are more likely to be lower SES. Since blacks are more likely to be lower SES, they have higher rates of obesity which lead to higher rates of BP, too.
But one of the most important factors here is education. If people don’t know something, then they won’t do it. If they are taught ways to reduce symptom X, there is a higher chance of them reducing symptom X because they are better-armed with the knowledge against it. Knowing that all of these different environmental factors influence BP, then this points to a main culprit: education. Non, Gravlee, and Mulligan (2012) argue that it’s not ancestry that explains hypertension, but differences in education.
Non, Gravlee, and Mulligan (2012) analyzed both environmental and genetic factors which lead to hypertension. Thy found that in the black sample, systolic BP and mean arterial pressure (MAP) were higher among those who had a HS diploma or lower, but found no differences by education in the white sample.
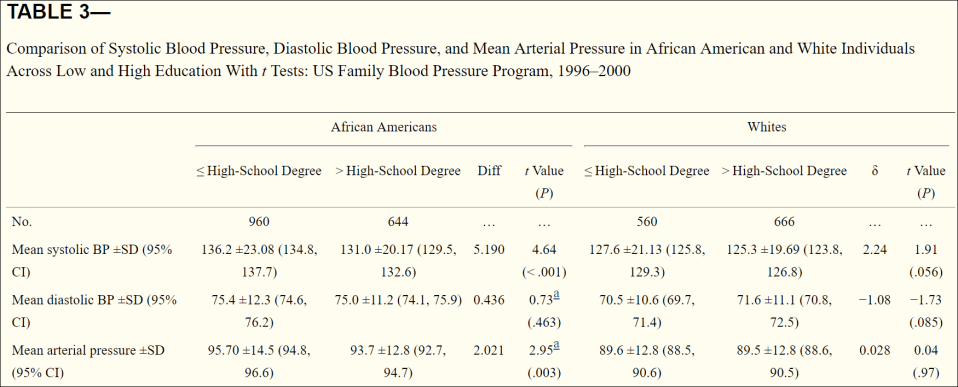
So black men were predicted to have a higher SBP, then white men, black women and finally white women, across all levels of education. SBP declined most sharply in black men and women compared to white men and women.
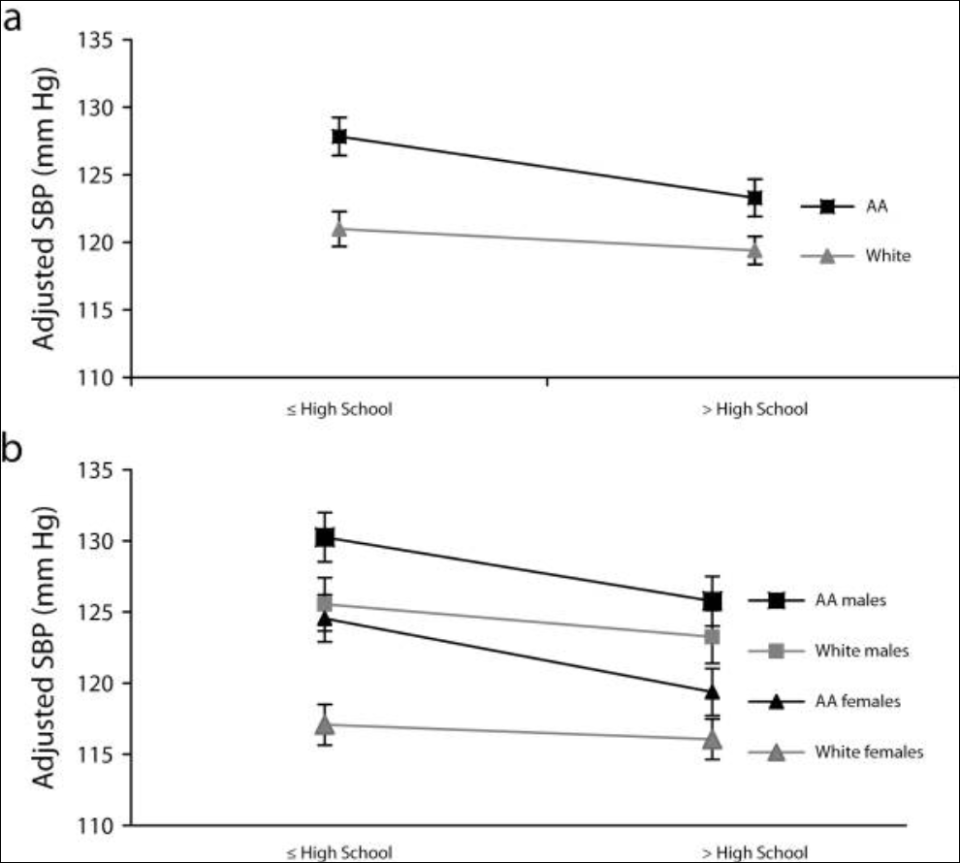
Genetic ancestry was not associated with BP among black Americans, but there was a significant association between education and BP. Education is, of course, not too good a measure of the social environment. Even using this measure, significant reductions in BP were found. Genetic ancestry is supposed to be associated BP in virtue of the ancestral environment of black Americans, along with supposed selection pressures which occurred on the Middle Passage. So if genetic ancestry isn’t associated, then the hypothesis is discarded.
Non, Gravlee, and Mulligan’s (2012) results support the “minority poverty hypothesis” because “the worst blood pressures were predicted for people who faced the double burden of being less educated and identifying as African American.” The minority poverty hypothesis is “The idea is that black people who live in poverty are uniquely disadvantaged in attaining good health because of the combination of poverty and race” (Hall, Humphreys, and Ruseski, 2015: 5).
Because genetic ancestry was estimated from only 294 loci, and a large set of populations across Africa, which may not be best for representing the West African ancestry of black Americans (Note how this is the population in question in the theory we are discussing). So an analysis focusing just on West African populations may change the relationship. Education was their only measure of the social environment, but other measures of the social environment, like “residential segregation, psychosocial stress, and everyday discrimination” may fully account for higher levels of BP in black Americans. Of course, further there needs to be further study to see whether it is the education per se that causes the differences in BP or if education serves only as a marker for other aspects of the social environment.
The evidence that education accounts for a lot of the variation in differences in BP between blacks and whites is strong. If it is other aspects of the social environment, and not education per se, then there is something in that environment that does not elicit the physiological response that leads to higher BP. We can also, of course, liken this to the Mazur’s (2016) honor culture hypothesis—the hypothesis “that young men’s participation in the honor culture of poor black neighborhoods has the effect of elevating T.” This is due to the adaptiveness of our physiological systems and how it adapts to the environment based on environmental cues.
There was one recent study where they found that “Among black male barbershop patrons with uncontrolled hypertension, health promotion by barbers resulted in larger blood-pressure reduction when coupled with medication management in barbershops by specialty-trained pharmacists” (Victor et al, 2018). This, of course, makes sense. If one is made aware of anything wrong with them, then they will be more likely to seek help for their ailments.
Victor et al (2018) write:
Because black men with hypertension often have multiple cardiovascular risk factors,37 marked reductions in blood pressure — if sustained with the use of our approach and then initiated more widely — might reduce the high rates of hypertension-related disability and death among black men with hypertension in the United States.11
Since three out of four black men have high blood pressure by the time they are 55, then if this can and does hold for the long-term, then this would help many individuals.
Seventy-eight barber shops enrolled in the program. The n was 319 men who had a SBP of 140 mm or higher from 52 black-owned barber shops. The intervention increased doctor visits and anti-hypertensive medications (which I disagree with). Pharmacists were placed in the shop and checked the BP of black men who entered (barbers were also trained to measure BP). Reductions of 21.6 and 14.9 SBP and DBP respectively were seen. 63 percent of those who participated achieved a normal BP whereas 12 percent of those in the control group did so. This, clearly, is another way in which education can lower BP in this population.

This is a great idea—and if further study confirms that this works, it should begin to be implemented elsewhere. The most important factor is outreach—getting the information to people and teaching them how to reduce it on their own through lifestyle modifications. And since outreach is related to educating people on a certain topic, then this, too, falls under the—somewhat large—umbrella of “education.”
In sum, the SHH is a just-so story and doesn’t explain why blacks have higher rates of BP than whites. Genetic ancestry seems to not explain hypertension rates between blacks and whites. Social environment changes and outreach can lower BP disparities between populations. If one understands the intricacies of physiology, then they would understand the physiological responses to different environmental/social stimuli.
