
Home » Posts tagged 'Biology'
Tag Archives: Biology
Not Feeling Pain: What is CIPA (Congenital Insensitivity to Pain with Anhydrosis)?
1750 words
“Congenital Insensitivity to Pain” (CIPA, or congenital analgesia: CIPA hereafter) is an autosomal recessive disease (Indo, 2002) and was first observed in 1932 (Daneshjou, Jafarieh, and Raeeskarami, 2012). It is called a “congenital disorder” since it is present from birth. Since the disease is autosomal recessive, the closer the two parents are in relatedness, the more likely it is they will pass on a recessive disorder since they are more likely to have and pass on autosomal recessive mutations (Hamamy, 2012). First cousins, for example, 1.7-2.8% higher risk of having a child with an autosomal recessive disease (Teeuw et al, 2013). Consanguinity is common in North Africa (Anwar, Khyatti, and Hemminki, 2014) and the Bedouin have a high rate of this disease (Schulman et al, 2001; Lopez-Cortez et al, 2020; Singer et al, 2020). Three mutations in the TrkA (AKA NTRK1) have been shown to induce protein mis-folding which affect the function of the protein. Different mutations in the TrkA gene have been shown to have be associated with different disease outcomes (Franco et al, 2016). Since the mutated gene in question is needed for nerve growth factors, the pain signals cannot be transferred to the brain since there are hardly any of them there (Shin et al, 2016).
Individuals unfortunate enough to be inflicted with CIPA cannot feel pain. Whether it’s biting their tongues, feeling pain from extreme temperatures. People with CIPA have said that while they can feel the difference between extreme temperatures—hot and cold—they cannot feel the pain that is actually associated with the temperatures on their skin see (Schon et al, 2018). When they bump into things, they may not be aware of what happened and injuries may occur which heal incorrectly due to no medical attention and only noticing the fractures and other things that occur due to CIPA years later after they see doctors for what is possibly factors due to having the disease. People with CIPA are thought to be “dumb” because they constantly bump into things. But what is really happening is that, since they cannot feel pain, they have not learned that bumping into things could be damaging to their bodies, as pain is obviously an experience-dependent event. So these people learn, throughout their lives, to fake being in pain as to not draw suspicion to people who may not be aware of the condition. Children with the disease are thought, most of the time, to be victims of child abuse, but when it is discovered that the child who is thought to be a victim of abuse is inflicted with CIPA (van den Bosch et al, 2014; Amroh et al, 2020), treatments shift toward managing the disease.
About twenty percent of people with CIPA live until three years of age (Lear, 2011), while 20 percent of those who die at age 3 die from complications due to hyperpexia (an elevated body temperature over 106. degrees Fahrenheit) (Rosemberg, Marie, and Kliemann, 1994; Schulmann et al, 2001; Indo, 2002; Nabyev et al, 2018). Since they cannot feel the heat and get themselves to cool down, Due to a low life expectancy (many more live until about 25 years of age), this disease is really hard to study (Inoyue, 2007; Daneshjou, Jafarieh, and Raeeskarami, 2012). People hardly make it past that age since they either don’t feel the pain and do things that normal people, through experience, know not to do since we can feel pain and know to not do things that cause us pain and discomfort or they commit suicide since they have no quality of life due to damaged joints. Furthermore, since they cannot feel pain, people with this disease are more likely to self-mutilate since they cannot learn that self-mutilation causes pain (since pain is a deterrent for future action that may in fact cause pain to an individual). They also cannot sweat, meaning that control of the body temperature of one afflicted with CIPA is of utmost precedence (since they could overheat and die). Thus, these cases of deaths of individuals with CIPA do not occur due to CIPA per se, they occur due to, say, not feeling heat and then sweating while not attempting to regulate their body temperature and cool down (whether by naturally sweating due to being too hot or getting out of the extreme hot temperature causing the elevated body temperature). This is known as “hyperpyrexia” and this cause of death affects around 20 percent of CIPA patients (Sasnur, Sasnur, and Ghaus-ul, 2011). Furthermore, they are more likely to have thick, leathery skin and also show little muscular definition.
Not sweating is associated with CIPA and if one cannot sweat, one cannot have their body temperature regulated when they get too hot. So if they get too hot they cannot feel it and they will die of heat stroke. The disease, though, is rare, as only 17-60 people in America currently have it, while there are about 600 cases of the disease worldwide (Inoyue, 2007; Lear, 2011). This disease is quite hard to identify, but clinicians may be able to detect the presence of the disease through the following ways: Infants biting their lips, fingers, cheeks and not crying or showing any instance of being in pain after the event; repeated fractures in older children; a history of burns with no medical attention; observing that a child has many healed joint injuries and bone fractures without the child’s parents seeking medical care; observing that the patient does not react to hot or cold events (though they can say they can feel a difference between the two) they make errors in distinguishing in whether something is hot or cold (Indo, 2008).
Children who have this disease are at a higher risk of having certain kinds of bodily deformations, since they cannot feel the pain that would make them be hesitant to perform a certain action in the future. Due to this, people with this disease must constantly check themselves for cuts, abrasions, broken bones, etc to ensure that they cannot feel when they actually occur to them. They don’t cry, or show any discomfort, when experiencing what should be an event that would cause someone without CIPA to cry. CIPA-afflicted individuals are more likely to have bodily deformations since their joints and bones do not heal correctly after injury. This then leads to their walking and appearance to be affected. This is one of many reasons why the parents of people with CIPA must constantly check their children for signs of bodily harm or unintentional injuries. One thing that needs to be looked out for is what is termed Charcot joint—which is a degenerative joint disorder (Gucev et al, 2020).
A specific form of CIPA—called HSAN-IV—was discovered in a village in southern Finland called Vittangi, where it was traced to the founder of the village itself in the 1600s. Since the village was remote with such a small population, this meant that the only people around to marry and have children with were people who were closely related to each other. This, then, is the reason why this village in Finland has a high rate of people afflicted with this disease (Norberg, 2006; Minde, 2006). This, again, goes back to the above on consanguinity and autosomal recessive diseases—since CIPA is an autosomal recessive disease, one would reason that we would find it in populations that marry close relatives, either due to custom or population density.
Many features have been noted as showing that an individual is afflicted with CIPA: absent pain sensation from birth, the inability to sweat; and mental retardation, lower height and weight for their age (Safari, Khaledi, and Vojdani, 2011; Perez-Lopez et al, 2015). Children with CIPA have lower IQs than children without CIPA, so there is an inverse relationship between IQ and age; the older the age of the child with CIPA, the lower their IQ, while the reverse is true for individuals who are younger (Erez et al, 2010). One girl, for example. had a WISC-III IQ of 49, and she self-mutilated herself by picking at her nails until they were no longer there (Zafeirou et al, 2004). Another girl with CIPA was seen to have an IQ of 52, be afflicted with mental retardation, have a low birth weight, and was microcephalic (Nolano et al, 2000). Others were noted to have IQs in the normal range (Daneshjou, Jafarieh, and Raaeskarami, 2012). People with a specific form of this disease (HSN type II) were observed to have IQs in the normal range (though it is “caused by” a different set of genes than CIPA, HSN type IV; Kouvelas and Terzoglou, 1989). However, it has been noted that the cut-off of 70 for mental retardation is arbitrary (see Arvidsson and Granlund, 2016). While running a full gamut of tests on an individual thought to have CIPA, we can better attempt to ensure a higher quality of life in individuals afflicted with the disease. In sum, IQ scores of CIPA individuals do not reflect that the mutations in TrkA “cause” IQ scores; it is an outcome of a disrupted system (in this case, mutations on the TrkA gene).
There is currently no cure for this disease, and so, the only way to manage complications stemming from CIPA is to work on the injuries that occur to the joints that occur as they happen, to ensure that the individual has a good quality of life. Treatment for CIPA, therefore, is not actually curing the disease, but it is curing what occurs due to the disease (bone breaks, joint destruction), which would then heighten the quality of life of the person with CIPA (Nabiyev, Kara, and Aksoy, 2016). Naloxone may temporarily relieve CIPA (Rose et al, 2018), while others suggest treatments such as remifentanil (Takeuchi et al, 2018). We can treat outcomes that arise from the disease (like self-mutilation), but we cannot outright cure the disease itself (Daneshjou, Jafarieh, and Raaeskarami, 2012). The current best way to manage the disease is to identify the disease early in children and to do full-body scans of afflicted individuals to attempt to cure the by-products of the disease (such as limb/joint damage and other injuries). Maybe one day we can use gene therapy to help the afflicted, but for now, the best way forward is early identification along with frequent check-ups. By managing body temperature, having frequent check-ups, modifying the behavior of the child as to avoid injuries, wearing a mouth guard so they do not grind their teeth or bite their tongue, avoiding hot or cold environments or food, (Indo, 2008; Rose et al, 2018).
CIPA is a very rare—and very interesting—disease. By better understanding its aetiology, we can better help the extremely low number of people in the world who suffer from this disease.
Polygenic Scores and Causation
1400 words
The use of polygenic scores has caused much excitement in the field of socio-genomics. A polygenic score is derived from statistical gene associations using what is known as a genome-wide association study (GWAS). Using genes that are associated with many traits, they propose, they will be able to unlock the genomic causes of diseases and socially-valued traits. The methods of GWA studies also assume that the ‘information’ that is ‘encoded’ in the DNA sequence is “causal in terms of cellular phenotype” (Baverstock, 2019).
For instance it is claimed by Robert Plomin that “predictions from polygenic scores have unique causal status. Usually correlations do not imply causation, but correlations involving polygenic scores imply causation in the sense that these correlations are not subject to reverse causation because nothing changes the inherited DNA sequence variation.”
Take the stronger claim from Plomin and Stumm (2018):
GPS are unique predictors in the behavioural sciences. They are an exception to the rule that correlations do not imply causation in the sense that there can be no backward causation when GPS are correlated with traits. That is, nothing in our brains, behaviour or environment changes inherited differences in DNA sequence. A related advantage of GPS as predictors is that they are exceptionally stable throughout the life span because they index inherited differences in DNA sequence. Although mutations can accrue in the cells used to obtain DNA, like any cells in the body these mutations would not be expected to change systematically the thousands of inherited SNPs that contribute to a GPS.
This is a strange claim for two reasons.
(1) They do not, in fact, imply causation since the scores derived from GWA studies which are associational and therefore cannot show causes—GWA studies are pretty much giant correlational studies that scan the genomes of hundreds of thousands of people and look for genes that are more likely to be in the sample population for the disease/”trait” in question. These studies are also heavily skewed to European populations and, even if they were valid for European populations (which they are not), they would not be valid for non-European ethnic groups (Martin et al, 2017; Curtis, 2018; Haworth et al, 2018).
(2) The claim that “nothing changes inherited DNA sequence variation” is patently false; what one experiences throughout their lives can most definitely change their inherited DNA sequence variation (Baedke, 2018; Meloni, 2019).
But, as pointed out by Turkheimer, Plomin and Stumm are assuming that no top-down causation exists (see, e.g., Ellis, Noble, and O’Connor, 2011). We know that both top-down (downward) and bottom-up (upward) causation exists (e.g., Noble, 2012; see Noble 2017 for a review). Plomin, it seems, is coming from a very hardline view of genes and how they work. A view, it looks like to me, that derives from the Darwinian view of genes and how they ‘work.’
Such work also is carried out under the assumption that ‘nature’ and ‘nurture’ are independent and can therefore be separated. Indeed, the title of Plomin’s 2018 book Blueprint implies that DNA is a blueprint. In the book he has made the claim that DNA is a “fortune-teller” and that things like PGSs are “fortune-telling devices” (Plomin, 2018: 6). PGSs are also carried out based on the assumption that the heritability estimates derived from twin/family/adoption studies tell us anything about how “genetic” a trait is. But, since the EEA is false (Joseph, 2014; Joseph et al, 2015) then we should outright reject any and all genetic interpretations of these kinds of studies. PGS studies are premised on the assumption that the aforementioned twin/adoption/family studies show the “genetic variation” in traits. But if the main assumptions are false, then their conclusions crumble.
Indeed, lifestyle factors are better indicators of one’s disease risk compared to polygenic scores, and so “This means that a person with a “high” gene score risk but a healthy lifestyle is at lower risk than a person with a “low” gene score risk and an unhealthy lifestyle” (Joyner, 2019). Janssens (2019) argues that PRSs (polygenic risk scores) “do not ‘exist’ in the same way that blood pressure does … [nor do they] ‘exist’ in the same way clinical risk models do …” Janssens and Joyner (2019) also note that “Most [SNP] hits have no demonstrated mechanistic linkage to the biological property of interest. By showing mechanistic relations between the proposed gene(s) and the disease phenotype, researchers would, then, be on their way to show “causation” for PGS/PRS.
Nevertheless, Sexton et al (2018) argue that “While research has shown that height is a polygenic trait heavily influenced by common SNPs [7–12], a polygenic score that quantifies common SNP effect is generally insufficient for successful individual phenotype prediction.” Smith-Wooley et al (2018) write that “… a genome-wide polygenic score … predicts up to 5% of the variance in each university success variable.” But think about the words “predicts up to”—this is a meaningless phrase. Such language is, of course, causal when they—nor anyone else—has shown that such scores are indeed casual (mechanistically).
Spurious correlations
What these studies are indexing are not causal genic variants for disease and other “traits”, they are showing the population structure of the population sampled in question (Richardson, 2017; Richardson and Jones, 2019). Furthermore, the demographic history of the sample in question can also mediate the stratification in the population (Zaidi and Mathieson, 2020). Therefore, claims that PGSs are causal are unfounded—indeed, GWA studies cannot show causation. GWA studies survive on the correlational model—but, as has been shown by many authors, the studies show spurious correlations, not the “genetics” of any studied “trait” and they, therefore, do not show causation.
One further nail-in-the-coffin for hereditarian claims for PGS/PRS and GWA studies is due to the fact that the larger the dataset (the larger the number of datapoints), there will be many more spurious correlations found (Calude and Longo, 2017). When it comes to hereditarian claims, this is relevant to twin studies (e.g., Polderman et al, 2015) and GWA studies for “intelligence” (e.g., Sniekers et al, 2017). It is entirely possible, as is argued by Richardson and Jones (2019) that the results from GWA studies “for intelligence” are entirely spurious, since the correlations may appear due to the size of the dataset, not the nature of it (Calude and Longo, 2017). Zhou and Zao (2019) argue that “For complex polygenic traits, spurious correlation makes the separation of causal and null SNPs difficult, leading to a doomed failure of PRS.” This is troubling for hereditarian claims when it comes to “genes for” “intelligence” and other socially-valued traits.
How can hereditarians show PGS/PRS causation?
This is a hard question to answer, but I think I have one. The hereditarian must:
(1) provide a valid deductive argument, in that the conclusion is the phenomena to be explained; (2) provide an explanans (the sentences adduced as the explanation for the phenomenon) that has one lawlike generalization; and (3) show the remaining premises which state the preceding conditions have to have empirical content and they have to be true.
An explanandum is a description of the events that need explaining (in this case, PGS/PRS) while an explanans does the explaining—meaning that the sentences are adduced as explanations of the explanans. Garson (2018: 30) gives the example of zebra stripes and flies. The explanans is Stripes deter flies while the explanandum is Zebras have stripes. So we can then say that zebras have stripes because stripes deter flies.
Causation for PGS would not be shown, for example, by showing that certain races/ethnies have higher PGSs for “intelligence”. The claim is that since Jews have higher PGSs for “intelligence” then it follows that PGSs can show causation (e.g., Dunkel et al, 2019; see Freese et al, 2019 for a response). But this just shows how ideology can and does color one’s conclusions they glean from certain data. That is NOT sufficient to show causation for PGS.
Conclusion
PGSs cannot, currently, show causation. The studies that such scores are derived from fall prey to the fact that spurious correlations are inevitable in large datasets, which also is a problem for other hereditarian claims (about twins and GWA studies for “intelligence”). Thus, PGSs do not show causation and the fact that large datasets lead to spurious correlations means that even by increasing the number of subjects in the study, this would still not elucidate “genetic causation.”
Musicogenic Epilepsy
1800 words
I was watching the program Diagnose Me on Discovery Health and a woman kept having seizures whenever she heard a certain type of music—“alternative high-pitched female singing”, according to the woman—but her doctors didn’t believe her. So her and her husband began looking for specialists who specialize in hard-to-treat epilepsy. He recommended an endocranial EEG (images of such a surgery can be found below), which meant that the top part of her skull would be removed and electrodes would be placed onto the top of her brain. After the electrodes were placed on the brain. they played the music she said triggered her epilepsy—which was “high-pitched female singing”—and she began to seize. The doctor was shocked and he couldn’t believe what he saw. They ended up finding out that a majority—not all—of her seizing was coming from the right temporal lobe. So her and her husband had a choice—live with the seizures (which she couldn’t because she did not know where she would hear the music) or get part of her brain removed. She chose to have part of her right temporal lobe removed and when it was removed she no longer seized from hearing the music that formerly triggered her symptoms.
The condition is called “musicogenic epilepsy” which is a rare form of what is called “reflex epilepsy”—of which, another similar form involved hitting something which then causes seizing in the patient. (It’s called “reflex epilepsy” since the epileptic events occurs after an event—music, hitting something with your foot, seeing something on the television, etc.) This occurs when certain types of music are heard, certain musical notes can trigger electrical brain activity. The cure is to remove the part of the brain that is affecting the patient. (It is worth noting that many individuals throughout the past 100 years have had large sections of their brains removed and had no loss-of-functioning, staying pretty much the same as they were.) It is important to note that the music is not causing the seizures, it is triggering them—it brings them out. Most of the seizing is localized in the right temporal lobe (Kaplan, 2003), further being localized in Heschl’s gyrus (Nagahama et al, 2017). This has been noted by a few researchers since last century (Shaw and Hill, 1946; Fujinawa and Kawai, 1978) while the Joan of Arc was said to have her perception scrambled while hearing church bells; a Chinese poet stated that he became “absent-minded” and “sick” when hearing the flute-playing from the street vendor (Murray, 2010: 173).
The condition was first noted by a doctor in 1937, with the first known reference to this form of epilepsy being observed in the 1600s (Kaplan, 2003: 465). It affects about 1 in 10,000,000 people (Ellis, 2017). Critical reviews state not to underestimate the power of anti-epileptic drugs in the treatment and management of musicogenic epilepsy (Maguire, 2012), but in the case described above, such drugs did nothing to cure the woman’s seizures that occurred each time she heard a certain kind of music. The effect of music on seizing, it seems, is dichotomous with certain kinds of music either helping manage or causing seizing. The same melody, however, could be played in a different key and not cause seizing (Kaplan and Stoker, 2010) and so, it seems that certain types of sound frequencies influence/screw up the electrical activity in the brain which then leads to seizures of this kind. A specialist in epilepsy explains:
In people with reflex epilepsy, the trigger is extremely specific, and the seizure happens soon thereafter. “It can be a specific song by a particular person or even a specific verse of the song,” says Dr. So, who is a past president of the American Epilepsy Society. For some people, the trigger is a touch or motion. “If patients are interrupted in a particular way, if they are walking along and someone steps in front of them, they may have a seizure,” says Dr. So. In Japan, seizures caused by video games have been reported, he says, but they are highly unusual.
Dr. So evaluated a woman from Tennessee who began having seizures during church when she heard highly emotional hymns. She would blank out and drop her hymn book. At other times, Whitney Houston’s “I Will Always Love You” triggered seizures. The woman had a history of small seizures, but having one while hearing music was a new development. She said the seizures would typically begin with a sense of dread and the feeling that someone was lurking by her side. Dr. So and his Mayo Clinic team attached electrodes to the woman’s scalp to study electrical activity while she listened to different types of music. An electroencephalogram (EEG) showed that slow, emotional songs triggered seizure activity in her brain’s temporal lobe, while faster tunes did not. Dr. So diagnosed the woman with musicogenic epilepsy, a type of reflex epilepsy where seizures are caused by specific music or types of music, and prescribed antiseizure medication. He says he’s had another patient whose seizures were triggered by Rihanna’s “Disturbia” and Pharrell Williams’ “Happy.”
Though musicogenic epilepsy is extremely rare, it may be slightly underreported since many people with the disease may not put two and two together and link their seizing with the type of music or sounds they hear in their day-to-day life. One individual with epilepsy also recounts his experience with this type of rare epilepsy:
… but I still find that certain music, high pitched noise set’s off a kind of aura, I feel spaced out, have intense fear and it sounds almost like water rushing and I hear voices.
One case report exists of a man in which his later seizures were induced by music which prompted stress and a bad mood, implying that the aetiology of musicogenic epilepsy involves an association between the seizing and the patient’s mental state (Cheng, 2016).
We can see how the endocranial EEG looks and how it gets done (WARNING: GRAPHIC) by referring to Nagahama et al (2019):
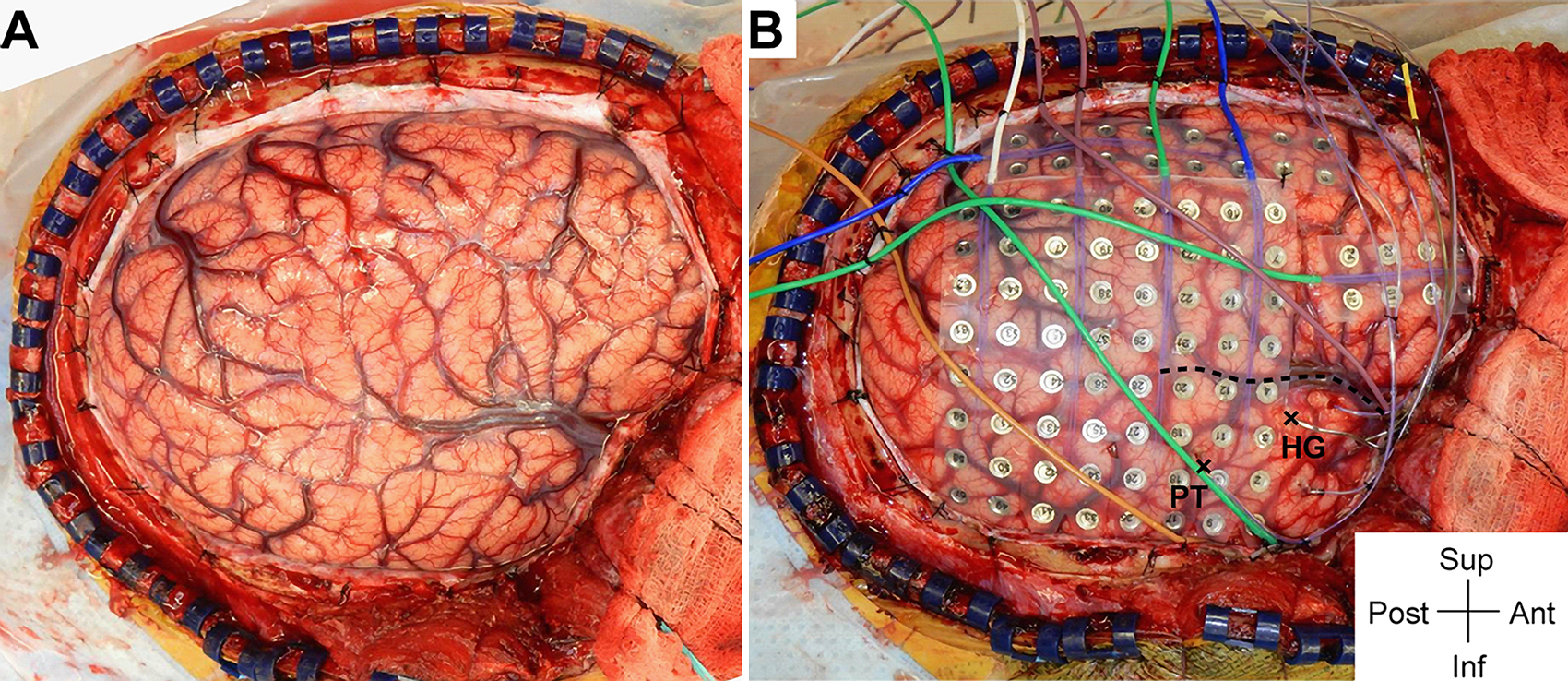
Intraoperative photographs demonstrating exposure and intracranial electrode placement. A right frontotemporoparietal craniotomy (A) allowed proper exposure for placement of grid, strip, and depth of electrodes (B), including the HG depth electrode. The sylvian fissure is marked with a dashed line. The HG depth electrode and PT depth electrose are marked with X symbols anteriorly and posteriorly, respectively, at their entry points at the cortical surface. Ant = anterior; inf = inferior; post = posterior; sup = superior.
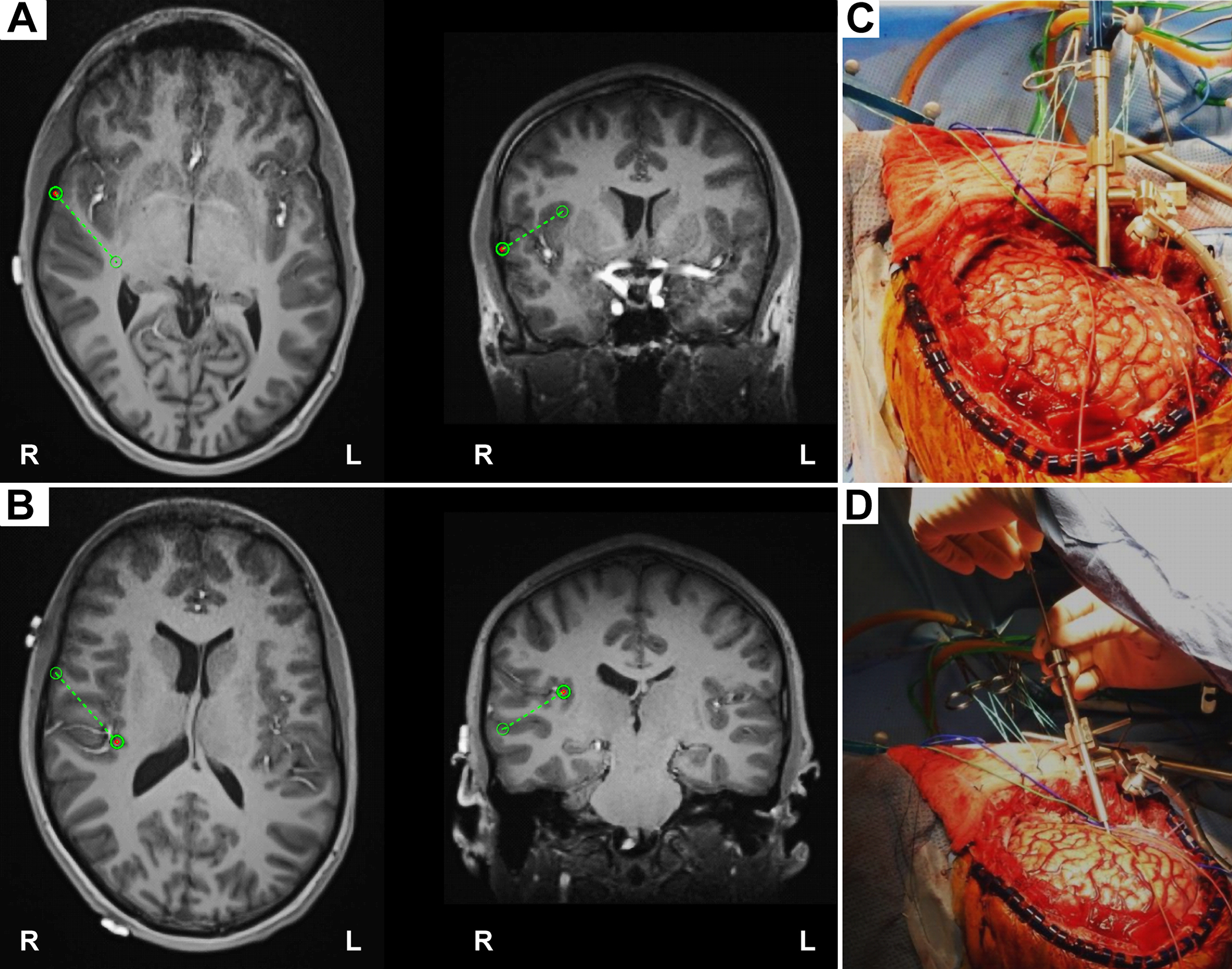
Intraoperative placement of the HG depth electrode. A: The planning view on the frameless stereotactic system (Stealth Navigation, Medtronic) showing the entry point and the trajectory (green circles and dotted lines). B: The similar planning view showing the target and the trajectory. C and D: Intraoperative photographs showing placement of the HG depth electrode. A Stealth Navigus probe was used to select the appropriate trajectory of a guiding tube positioned over the entry point (C). An electrode-guiding cannula was advanced through the tube to the previously determined depth (D). An actual depth electrode was subsequently passed through the cannula, followed by removal of the guiding tube/cannula system. Note the unique anterolateral-to-posteromedial trajectory within the STP for placement of the HG depth electrode.
The average age of onset of musicogenic epilepsy is 28 (Wieser et al, 1997) while the first cases are not reported until around one’s mid-to-late 30s due to the fact that most people are unware that music may be causing their seizures (Pittau et al, 2008; Generalov et al, 2018). This may be due to the fact that seizing may begin several minutes after hearing the music that affects the patient in question (Avanzini, 2003). While the specific tempo and pitch of music seems to have no effect on the beginnings of seizing (Wieser et al, 1997), many patients report that their specific triggers are due to hearing certain lines in songs (Tayah et al, 2006) which implies that it is not the music itself which is causing the seizing, but the emotional response that occurs to the patient after hearing the music and this is supported by the fact that many patients who report such symptoms are interested in music or are musicians themselves (Wieser et al, 1997).
See table 1 from Kaplan (2003: 466) for causes of musicogenic epilepsy in the literature:
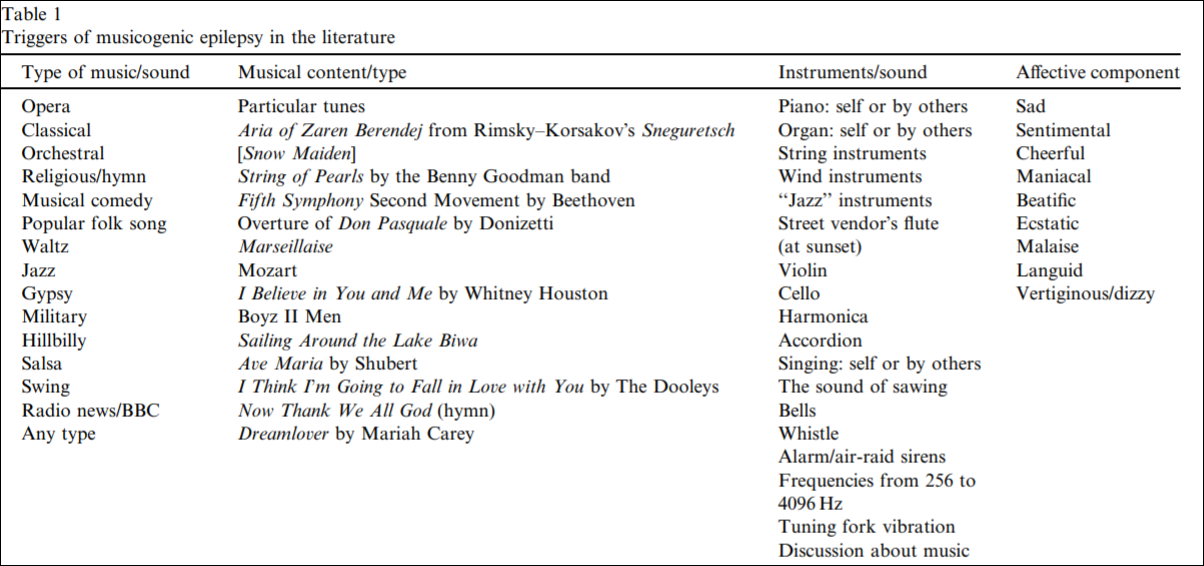
As can be seen by the above table, the mood component is related to the musical type; so the music elicits some sort of emotional state in the individual which would, it seems, to be part of the cause which then triggers the seizure—though the music/emotions are not causing the seizing itself, it is bringing them out.
Going to the shops was fraught with danger. Turning on the television was like playing russian roulette. Even getting into a lift was a gamble. For 23 years my life was hugely restricted because I had epileptic fits whenever I heard music.
If it was more than a few notes, a strange humming would start in my head, immediately followed by a seizure. I didn’t fall to the ground and twitch, but would wander around in a daze, my heart racing, my mind a blank. I also experienced hallucinations: people around me appeared microscopic and it felt as if I had been captured by an invisible force field. It was a terrifying experience and I felt drained for hours afterwards. (Experience: Music gave me seizures)
One woman describes her experience with musicogenic epilepsy for The Guardian. She did everything she could think of to stop the music-induced seizures—from sticking cotton balls into her ears to stop hearing sounds, to staying inside of the house (in case a car driving by played the type of music that triggered her seizing), to having a silent wedding with no music. She ended up getting referred to a specialist and she got her brain checked out. Come to find out, she had scarring on her right temporal lobe and so, surgery was done to fix it. She was cured from her condition and she could then attend social functions in which music was played.
The brain has the capacity to produce electricity, and so, in certain individuals with certain things wrong with the structure of their brains (like in their right temporal lobe), if they hear a certain kind of music or tune, they may then begin seizing. While the condition is rare (around 150 cases have been noted), strides are being made in discovering how and why such things occur. The only cure, it seems, is to remove the affected part of the brain—the right temporal lobe in a majority of cases. Such operations, however, do not always have the same debilitating effects (i.e., causing loss of mental capacity). That the brain’s normal functioning can be affected by sound (music) is very interesting and speaks to the fact that our brains are an enigma which is just beginning to be unraveled.
