Speech should have limits. Growing up in America, this of course sounds like crazy talk. But the fact that we agree that actions that cause harm to others should be restricted then leads to a contradiction—and it’s due to this contradiction that we should—and in some cases do—not let anyone say whatever is on their minds without consequence. Think of defamation laws, harassment and violence-incitement. Social media amplifies hate speech—especially now where, although it’s not fully a “free speech platform”, Twitter has turned into a cesspool of hate speech (see here for examples). So if we agree that certain actions that cause harm to others should be restricted, then there is a logical contradiction—mainly that allowing speech that causes harm contradicts the principle that we should avoid harm causing actions. There is a moral imperative to restrict racist speech acts.
(1) We agree that certain actions that cause harm to others should be restricted.
Knowing this:
(2) Assume that we shouldn’t restrict any forms of speech. (3) This implies that speech that causes harm shouldn’t be restricted. (4) But we know that certain kinds of speech acts cause harm, leading to negative mental and physiological health outcomes and violence. (5) But allowing speech that causes harm contradicts the principle that actions which cause harm should be restricted. (6) So the assumption that speech should have no restrictions—including speech that causes harm—leads to a contradiction with (1), since actions that cause harm to others should be restricted. (8) Therefore, some forms of speech—particularly speech that causes harm—should be restricted to prevent negative consequences.
Put simply: (1) Actions causing harm should be restricted. (2) Since some speech acts cause tangible harm, then unfettered speech acts contradict the principle that actions which cause harm should be restricted. (C) So speech restrictions are justified.
Or:
(1) If speech causes tangible harm, then it should be restricted to prevent that harm. (2) Some forms of speech—including incitement to violence, defamation, and true threats—cause tangible harm. Therefore, (C) these forms of speech should be restricted.
The argument I have constructed against free speech I have constructed is valid, and I will argue for it’s soundness. I will then discuss how we can identify racist speech (though I think it is pretty obvious), then I will argue that such speech causes tangible harm. I will show that then racist then is caught in a contradiction that he cannot see himself out of—namely that they presumably think that crime is bad based on talking about all types of racial crime differences but then contradict that by engaging in action which lead to crime.
Defending the argument
The argument assumes Mill’s harm principle (HP)—where Mills stated that “the only purpose for which power can be rightly exercised over any member if a civilized community, against his will, is to prevent harm to others.” Even in America, where we have the First Amendment, certain speech acts are restricted—like defamation, incitement to violence and true threats. So while free expression is meaningful, it’s clearly not absolute, and I argue that we should extend that to hate speech, since hate speech causes tangible harm.
The HP also lines up with the ethical view that one’s actions should not infringe upon the well-being and rights of others. Therefore, speech should be judged on the impact it has towards others. We can then extend this to not only individual harm but broader, societal harm. Speech acts that promote systemic discrimination—like hate speech—can and should be restricted since they contribute to an environment in which certain groups are systematically disadvantaged or harmed which then gels well with the notion that harm would include social and psychological impacts.
We can then extend the HP to include psychological and emotional harm. Speech that systematically targets individuals or groups can cause significant emotional distress and could lead to significant mental health issues should be considered under the HP. Certain speech acts can contribute to systemic harm by perpetuating or reinforcing structures of oppression, like racist, sexist, or anti-same-sex speech.
Thus, the HP should be extended to include preventative measures against potential harm. So in cases where speech is likely to incite violence or discrimination, preventative restrictions should be in place, especially where there are historical or contemporary tensions.
For instance, look at the RFK’s idiotic view that vaccines cause autism. This is a view that should not be amplified, since it could lead to lower rates of vaccination and along with it, physical (and mental) harm. What RFK is saying is outright misinformation, since we have large trials which definitively show that vaccines do not cause autism (and the study that RFK is presumably referring to is even retracted; (Allen and Ivers, 2010; Eggertson, 2010, see Wakefield et al, 1998).
Identifying racist speech
To identify racist speech, we can just look at the language used. Racist speech denies the humanity, dignity or worth of individuals based on their race. It makes sweeping generalizations or assumptions about a group based on preconceived notions or biases. It demonizes a group, portraying them as evil, dangerous, or threatening. It excludes or ignores experiences or concerns of a group. It uses derogatory language like slurs and epithets which are intended to degrade and offend. It advocates for discrimination or violence against a group. And it perpetuates systemic racism by justifying discriminatory policies practices or institutions which exacerbate inequalities. So:
A speech act is a racist speech act, iff
(1) it dehumanizes, stereotypes, demonizes, marginalizes, or uses derogatory language against individuals or groups based on their race, ethnicity or national origin; or (2) it promotes hate, discrimination or harm against individuals based on their race, ethnicity, or national origin; or (3) it perpetuates systemic racism by reinforcing or justifying discriminatory practices, policies, or institutions that perpetuate racial inequalities.
Racist speech acts are those that dehumanize, demean, or discriminate aya7shr individuals or groups based on race. Language has both explicit and implicit meanings, and its racial B can be identified through the explicit use of racial slurs or derogatory terms which are historically and universally recognized as demeaning to specific racial groups. So the context in which words are used significantly influences their racist nature where one stereotypes and makes generalizations about racial groups including individualw to a set of prejudiced assumptions. The intent should also be considered, but the impact often outweighs good intentions.
Speech from those in positions of power or privilege which targets marginalized groups amplifies the racist impact due to the existing power balance in society. But even if the speech in question is intended to not be racist, if it reinforces racial hierarchies, promotes discrimination, or causes harm, then it could be considered racist in its effects (this is why I think the “HBD”-hereditarian movement is racist). So historical and cultural references also inform the racist nature of certain speech acts.
Thus, to identify racist speech acts, one must analyze not just the words one uses but the context in which they’re said, intent, impact, power dynamics, and the historical and cultural weight they carry. This goes beyond what is on the surface of the words that one speaks or writes and allows us to recognize when a speech act is a racist one.
The moral contradiction of the racist
Now we come to the issue of racist hate speech. We know that racism and stereotypes which lead to self-fulfilling prophecies cause the black-white crime gap (based on considerations of the theory of African American offending). We also know that racism causes “weathering” in black women (Geronimus et al 2006, 2011; Sullivan, 2015) So since we know that racism leads to crime in the black American population, and we know that it leads to differences in physical and mental health, we know that racism is morally wrong. So the HP should be extended to include racist speech acts, since they have tangible effects. Racist speech acts promote harmful stereotypes, and contribute to crime through marginalization which then cause physiological and psychological harm. In the argument that I made here, I showed that since crime is bad and racism causes crime then racism is bad—this is a simple, yet powerful argument. So since racist speech acts can lead to tangible harms, both directly (through incitement or psychological stress) and indirectly (contributing to systemic issues like crime rates in African Americans), such views should be restricted. I assume that racists think that crime is bad, but since we know that racism and stereotypes which lead to self-fulfilling prophecies cause crime for African Americans, it seems that their racist speech acts lead to a real-world contradiction.
(1) Crime is bad. (2) Racism causes crime. (C) Thus, racism is morally wrong. (1) is self-evident based on people not wanting to be harmed. (2) is known upon empirical examination, like the TAAO and it’s successful novel predictions. (C) then logically follows.
…
B stands for “crime is bad”, C stands for “racism causes crime”, D stands for racism is objectively incorrect, so from B and C we derive D (if C causes B and B is bad, then D is morally wrong). So the argument is “(B ^ C) -> D”. B and C lead to D, proving validity.
So: (1) If actions causing harm should be restricted ((B ^ C) –> D), and racist speech acts cause harm both directly and indirectly, then racist speech acts should be restricted. (2) Actions causing harm should be restricted (B is true based on ethical principles) and racist speech acts cause harm (C is true based on empirical evidence). Therefore, (C) racist speech acts should be restricted (D is true).
This is the moral conundrum of the racist. Racists agree that crime is bad (which can be seen by there hyper-focus on black-on-white, black-on-black, and black-on-Asian crime). But their speech acts contribute to the very actionsthey condemn. This is a contradiction. If racists believe that crime is bad, and if we accept the evidence that racism and stereotypescontribute to crime for African Americans (and we should since the TAAO makes successful novel predictions), then by promoting racism through their speech acts, racists are inadvertently contributing to what they claim to despise! If one holds to the claim that crime is bad, then one should therefore have a moral responsibility to not contribute to its causes. So by promoting racism, racists are directly contributing to crime. Racists, then, have an inconsistency between their beliefs and actions.
Conclusion
Most agree that we shouldn’t have ultimate free speech, which I take to be saying whatever you want whenever you want to whomever you want. Of course, in private, two people could express views to each other that would be seen as negative to society at large, but they would not be harm-causing speech acts since they are only expressing such views to themselves and not going on social media and airing their racism for millions to see. Using and extending Mills’ harm principle then allows us to restrict certain speech that causes harm. So since we know that racist speech acts lead to psychological and physiological harm and since we know (based on TAAO studies) that racism and stereotypes which lead to self-fulfilling prophecies lead to crime in black Americans, such racist hate speech must be regulated.
I showed when a speech act is a racist speech act, by stating some conditions. Racists today distribute racism in the form of memes and “jokes” on social media. It is pretty obvious when speech is meant to convey a racist tone and be applied toward a group, and the conditions I have paid out pave the way for that.
I showed that racist hate speech leads to increased rates of ctime in black Americans. The TAAO not only shows how racism is linked to crime, it also shows how racist speech acts perpetuate harmful stereotypes which then lead to self-fulfilling prophecies which then cause crime among African Americans. So this suggests that since racism leads to crime (which is universally seen as bad) among African Americans, then racist speech (as a form of action) should then be seen as morally reprehensible and therefore potentially restrictable under the HP. And since we know that racist speech acts lead to weathering and increased allostatic load, this is yet another reason to restrict such speech. Such speech acts contribute to these health disparities by creating environments of chronic stress and marginalization. Thus, by recognizing these health outcomes as tangible harms, we can further justify applying the HP to racist speech.
The ethical flaw of the racist was discussed. They claim to oppose crime (as seen by their continual discussions of inter-racial and intra-racial crime), yet their speech promotes conditions which increase crime rates among the very groups they discriminate against. So the racist in fact contributes to crime, which then undermines their own moral stance against crime!
This is why we should not have a kind of free-reign free speech—because it’s quite cleat that racism leads to crime in the black American population and that racism leads to negative psychological and physiological health outcomes. Therefore, knowing this, “free speech” shouldn’t be a thing. We should restrict it not only for the societal health of the country but for the psychological and psychological health and well-being of groups and individuals.
(Note: I don’t believe in an afterlife and I’m not a theist.)
What do Americans think about the existence of an afterlife and what are the differences between races?
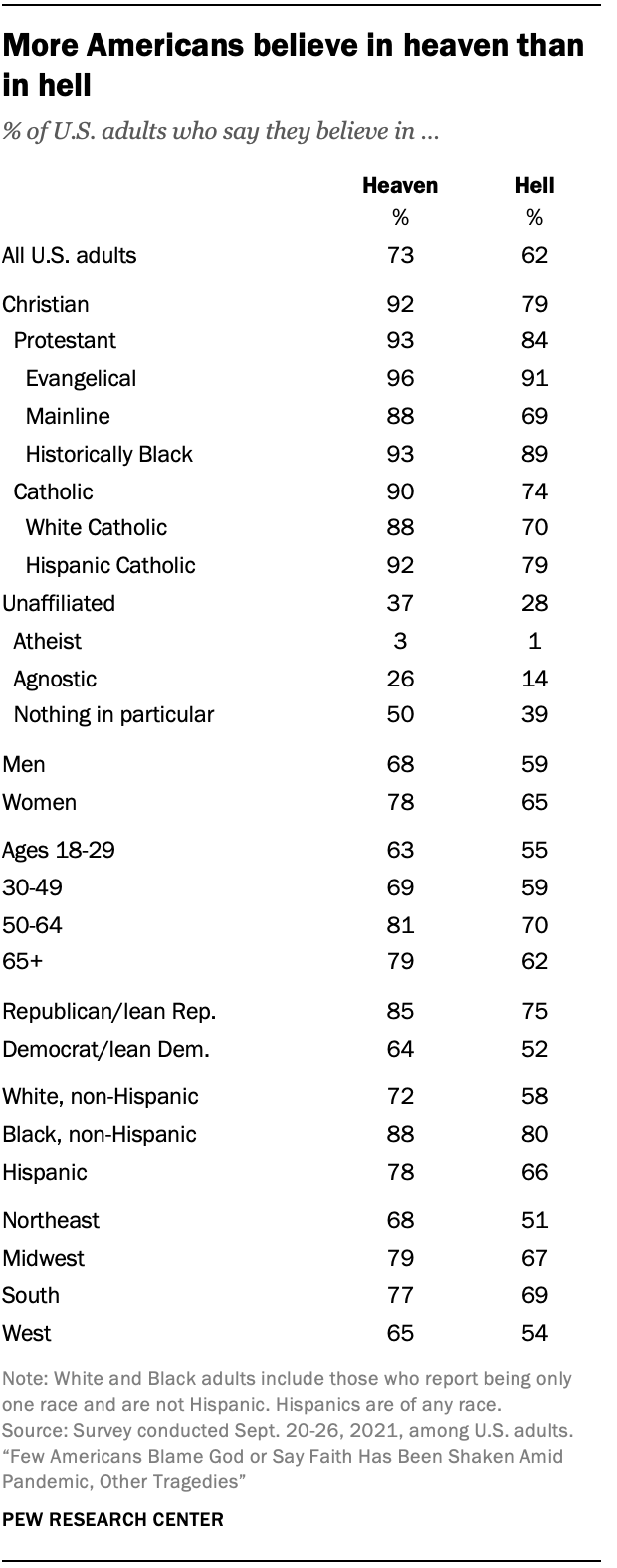
What do Americans think about the existence of an afterlife—of heaven and hell? The existence of an afterlife to American citizens is clear—more Americans believe in heaven but not in hell, per Pew. But 26% of the respondents didn’t believe in either heaven or hell. But those who did not believe in heaven or hell but did believe in an afterlife were asked to describe their views:
Respondents who believe in neither heaven nor hell but do still believe in an afterlife were given the opportunity to describe their idea of this afterlife in the form of an open-ended question that asked: “In your own words, what do you think the afterlife is like?”
Within this group, about one-in-five people (21%) express belief in an afterlife where one’s spirit, consciousness or energy lives on after their physical body has passed away, or in a continued existence in an alternate dimension or reality. One respondent describes their view as “a resting place for our spirits and energy. I don’t think it’s like the traditional view of heaven but I’m also not sure that death is the end.” And another says, “I believe that life continues and after my current life is done, I will go on in some other form. It won’t be me, as in my traits and personality, but something of me will carry on.”
Blacks were slightly more likely to believe in heaven over whites, though a super majority of both races do believe in heaven, while way more blacks than whites believed in the existence of hell. Others professed less-widely-held views on the afterlife, like existing as a spirit, consciousness, or energy in the afterlife. Those who believe state that heaven is free from earthly matters, such as suffering while in hell it is the opposite—hell is nothing but eternal suffering, not due to any fire and brimstone, but because it is eternal separation from God. America is, to my surprise, still a very superstitious country when it comes to God and Satan and the existence of heaven and hell. People believe that their prayers can be answered and that interactions between the living and the dead are possible. Black Americans are more likely to believe that their prayers can be directly answered in comparison to white Americans (83 percent compared to 65 percent, respectively) , while 67 percent of Americans think it’s possible. Black Americans also believe that revelations from a higher power are possible in comparison to white Americans (85 percent and 66 percent, respectively), while black Americans are more likely to believe that they have experienced contact from a higher power compared to white Americans (53 percent compared to 25 percent, respectively).
Moreover, black men over age 50 who attend church had a 47 percent reduction in all-cause mortality compared to those who did not attend (Bruce et al, 2022), so there seems to be a protective effect that occurs due to attending church services (Assari and Lankarani, 2018; Carter-Edwards et al, 2018; Majee et al, 2022). It has been found that blacks consistently report lower odds of having depression, and the answer is probably due to attending religious services (Reese et al, 2012). However, when it comes to church attendance, for white women their attendance at church is either nonexistent or protective when it comes to body mass while for black women consistent relations between church attendance and body mass have been shown (Godbolt et al, 2018). Given the fact that black women have been consistently more likely to be obese than white women since at least the late 80s and 90s (Gillum, 1987; Kumanyika, 1987; Allison et al, 1997) and today (Tilghman, 2003; Johnson et al, 2012; Agyemang and Powell-Wiley, 2014; Tucker et al, 2021), this finding is not surprising. But the effects of racism can not only explain the higher rates of obesity in black women (Cozier et al, 2014), it could also explain the higher rates of “weathering” of black women’s bodies (Geronimus et al, 2006).
Nevertheless, blacks are more likely to be religious and report religious experiences in comparison to whites, and blacks are also more likely to be religious in comparison to the general US population. Why may blacks be more religious than whites? This is a question I will try to answer in the future.
The ultimate answer to your question is found in Revelation 21-22 which describes the new heaven and earth. In Revelation 21:24 we are told that people from the various nations will be in heaven. That is, those who believe in Jesus Christ and follow Him will live there for eternity. But the culture of heaven will be God’s culture. Everything is new. Heaven and earth will be new. The old will have disappeared and the new will have come. Sin will be gone and racial prejudices and alliances will be gone.
The difference between heaven and hell is that in heaven—that is, in the new heaven and new earth—there will be perfect racial and ethnic harmony, but in hell, racial and ethnic animosities will reach their fullest fury and last forever.
So what is RACE? In my view, race is a suite of physical characteristics which are demarcated by geographic ancestry, as argued by Hardimon and Spencer. So if race is physical, then if a thing isn’t physical—that is, if a thing is immaterial—then there would be no way to identify which racial group they were a part of while they were alive. If we take the afterlife to be a situation in which a person has died but they then exist again as a disembodied soul/mind, then there can’t possibly be races in heaven, since what identified the person as part of a racial group (the physical) doesn’t exist anymore.
In the book The Myth of an Afterlife, Drange (2015: 329-330) articulates what he calls the nonidentificationargument, where it is inconceivable for a person to be identified if they are bodiless, and if they are bodiless and race is a property of physical bodies, then it would follow that there wouldn’t be races in heaven since disembodied souls, by definition, lack physical bodies—there would be no way for the identities of people to be established, and so if people’s identities cannot be established, then it follows that their racial identities cannot be established either.
Bodiless people would have no sense organs and no body of any sort.
Therefore, they could not feel anything by touch or see or hear anything (in the most common senses of “see” and “hear”).
Thus, if they were to have any thoughts about who they are, then they would have no way to determine for sure that the thoughts are (genuine) memories, as opposed to mere figments of imagination.
So, bodiless people would have no way to establish their own identities.
Also, there would be no way for their identities to be established by anyone else.
Hence, there would be no way whatever for the identities of bodiless people to be established.
But for a person to be in an afterlife at all, it is conceptually necessary for his or her identity to be capable of being established.
It follows that a totally disembodied personal afterlife is not conceivable.
Drange’s argument is against a certain conception of the afterlife, mainly if it is one where souls are disembodied, it follows that there would be no way to identify them, and so it follows that there would be no races in heaven, since race is a physical property of humans and their bodies. But there are different ways of looking at the possibility of races in heaven, depending on which theory of race one holds to.
Nathan Placencia (2021) argues that whether or not races exist in heaven depends on which philosophy of race you hold to, but he does make the positive claim that there may be racial identities in heaven. For racial constructivists, since race exists merely due to social conventions and racialization, then race wouldn’t exist. For the racial skeptic, since race doesn’t exist as a biological category, then races don’t exist. That is, since racial naturalism is false, then races of any kind cannot exist, where racial naturalism is basically like the hereditarian conception (or non-conception, if you will) of race (see Kaplan and Winther, 2015). Racial naturalists argue that race is grounded in genetically-mediated biological differences. I am of course sympathetic to the view, though I do hold that race is a social construct of a biological reality and I am a pluralist about race. The last conception that Placencia discusses is that of deflationary realism, where race is genetically-grounded but not itself normatively important (Hardimon, 2017). So Placencia claims that for the racial constructivists and skeptics, races won’t exist in heaven while for the deflationary realist, the “answer is maybe” on whether or not race will exist in heaven which then of course depends on what the resurrected heavenly bodies would look like.
Believers in heaven state that Believers will have new, physical bodies in heaven. But Jesus wasn’t immediately recognizable to his followers, though they did come to know that it was actually him after spending time with him. So theists of course then believe that we get new physical bodies in heaven but that we would look different than we did while we had a physical, earthly existence. Certain chapters in Revelations (21:4, 22:4) talk about God wiping away tears and a name appearing on their foreheads, so this then implies that there would be new, physical bodies in heaven. But now the question is, would heavenly bodies fall under racial lines as we currently understand them in this life? The question is obviously unanswerable, but certain texts in the Bible after Jesus’ resurrection state that he did look different than he did while he was alive in earth.
Baker-Hytch (2021: 182) argues that “the new creation is depicted as an everlasting reality whose human inhabitants from all nations will have resurrection bodies that—after the pattern of Jesus’ resurrection body—neither age nor die and that will partake in shared pleasures such as eating and drinking together.” So there is a trend in Christian and theistic thought that in heaven, we will all have new heavenly bodies and not exist as mere disembodied souls. But talk of new heavenly bodies faces an issue—if they are bodies in the sense that we think of bodies now, the bodies that we inhabit now, then would they grow old, decay and eventually die? Would God then give us new heavenly bodies? It would stand to reason that, if God is indeed all-powerful and all-knowing, then he would have thought these issues through and so heavenly bodies wouldn’t have the same properties as physical, earthly bodies and so they wouldn’t get older, die and eventually decay.
Conclusion
If the afterlife is completely disembodied, then it follows that race wouldn’t exist in the afterlife, since there would be no way for the identities of persons to be established, and thusly there would be no way for the race of the disembodied soul to be established. Most theists contend that we will have new, heavenly bodies in heaven, but whether or not they would look the same as the former earthly bodies is up in the air, since Jesus after his resurrection apparently looked different, since it states in the Bible that it took some time for Jesus’ followers to recognize him. So, if Heaven exists, will there be races? The concept RACE is a physical one. So if there are disembodied souls in heaven, and they have no physical bodies, then races won’t exist in heaven.
I obviously am a realist about race who holds to radical pluralism about racial kinds—there can be many concepts of race which are true and are context-dependent. Though I do not believe in an afterlife, I do believe that if an afterlife is nothing but disembodied souls living in heaven wkth God, then it follows that there won’t be races in heaven since there are no physical bodies on which to ground racial ontologies. On the other hand, if what most theists contend is true—that we get new heavenly bodies after our death and entrance into the afterlife—whether or not race would exist in heaven is questionable and it depends on which concept of RACE one holds to. If one is a constructivist or skeptic (AKA eliminativist or anti-realist) about race, then race wouldn’t exist in heaven as race is due to social conventions and the concept of racialization of groups as races. But if one is a deflationary realist about race (which I myself am), then the answer to the question of whether or not races would exist in heaven is maybe.
Nevertheless, whether or not one believes in the existence of an afterlife is slightly drawn on racial lines, with blacks being more likely to believe in an afterlife compared to whites, while are more likely to believe that their prayers can be directly answered and that they can talk to a higher power in comparison to whites.
So depending on how races get squared away in heaven upon receiving new heavenly bodies, it is unknown whether or not races will exist in heaven.
In their fight to get “critical race theory” (CRT) (or what they call CRT) banned from schools, James Lindsay and Christopher Rufo have twisted the terms “equity” and “equality” so they can better “beat” their opponents. But, unfortunately for them, there is a distinction between the two and the distinction between the two matters for issues of social justice. Although they don’t really understand the concepts they attempt to discuss, their readings into CRT/social justice have been repeated as if they have any meaning at all. By attempting to change the definition of equity, they are attempting to shift the discussion to what equity IS NOT, thereby attempting to side-step social justice issues. (Which is actually their goal.) This article will discuss what equity and equality are and aren’t, and how we can achieve equity not only in health but for all facets of our society.
What equity is; what equity isn’t
Lindsay, for example, makes the claim that “equity means “adjusting the shares in order to make citizens A and B equal” which would make “equity…something like a kind of “social communism”“. Lindsay’s confusion here will become apparent by the end of this article, as he is clearly strawmanning what “equity” means.
critical race theorists, on the other hand, have embraced a philosophy of European-style pessimism, dismissing equality under the law as “mere nondiscrimination.” They would replace it with a system of “equity” that treats individuals unequally in order to arrive at equal group outcomes.
Lindsay and Rufo are two of the spearheads leading the charge against “CRT” (what they call “CRT” is up to their discretion; it’s basically anything they don’t like) and they—quite clearly—have no idea what “equity” truly means. By equivocating on the term, they can then begin to redefine it and, when people hear the term, they won’t think of the original meaning, they will think of the new meaning that they have manufactured. (This is pretty much what Rufo has done with CRT.)
There is a distinction between “equity” and “equality.” For instance, to continue with the public health example, take public health equality and public health equity. In this instance, “equality” means giving everyone the same thing whereas “equity” means giving individuals what they need to be the healthiest individual they can possibly be. “Strong equality of health” is “where every person or group has equal health“, while weak health equity “states that every person or group should have equal health except when: (a) health equality is only possible by making someone less healthy, or (b) there are technological limitations on further health improvement” (Norheim and Asada, 2009). But we should not attempt to “level-down” people’s health to achieve equity; we should attempt to “level up” people’s health, though. That is, it is impossible to reach a strong health equality (making all groups equal), but we should—and indeed, have a moral responsibility to—attempt to lift up those who are worse-off. Poverty is what is objectionable, inequality is not. It is impossible to achieve true equality between groups, but we can—and indeed we have a moral obligation to—lift up those who are in poverty, which is, also a social determinant of health (Braveman and Gottlieb, 2014; Frankfurt, 2015; Islam, 2019).
We achieve health equity when all individuals have the same access to be the healthiest individuals they can be; we achieve health equality when all health outcomes are the same for all groups. Health equity is, further, the absence of avoidable differences between different groups (Evans, 2020). One of these is feasible, the other is not. But racism does not allow us to achieve health equity.
So, basically, the distinction is that equality means giving people the same things whereas equity means ensuring people are not held back to be the best they can be. We can say that health inequities are differences in health that are unjust, avoidable, and unfair (Sudana and Blas, 2013) and they are systematic, unfair, and avoidable differences between social groups (McCartney et al, 2019). Social justice efforts that attempt to bring down barriers that impede people from becoming the best they can be is imperative to a fair and equitable society, but this does not mean that efforts to make society more equitable toward social groups is an effort to make society more equal—it’s about making society more equitable where making society more equal is just a byproduct of making society more equitable. So, in the end, “inequities” refer to differences between groups that are avoidable, unjust, and unfair (see also Benjamins and De Maio, 2021).
In her new book, behavioral geneticist Paige Harden (2021: 120-125) has a discussion on “equity” where quotes Conley and Fletcher who claim that “heritability” estimates are a necessary but not sufficient measure of fairness (that is, a measure of an equitable society) in a society. I’ll discuss this in my review of the book, but for now, I will discuss her figure 8.2 on page 123. She shows a photograph of her daughter’s pre-K sign which states “Fair isn’t everybody getting the same thing. Fair is everybody getting what they need to be successful.” This perfectly embodies what equity is and how it is distinct from equality. The key phrase here is “what they need to be successful” and we can liken that to social advantage/disadvantage—certain social groups do not have what is needed to be successful, which, in this case, would be being the healthiest person they can be. Since they lack what they need to be successful and the lack of what they need is systemic (think food deserts/swamps), then they do not have what they need to be successful, meaning that this is an inequity. (This may well be one of the only good things I have to say about this book.)
Equity means fairness (7-10) or justice (8-10). Because these terms are open to interpretation, an operational definition is needed to guide measurement in diverse settings. In operational terms, pursuing equity in health can be defined as striving to eliminate disparities in health between more and less-advantaged social groups, i.e. groups that occupy different positions in a social hierarchy (8). Health inequities are disparities in health or its social determinants that favour the social groups that were already more advantaged. Inequity does not refer generically to just any inequalities between any population groups, but very specifically to disparities between groups of people categorized a priori according to some important features of their underlying social position. For example, individuals may be grouped by their income or material possessions, or by characteristics of their occupations, education, or geographic location, or by their gender, race/ethnicity, or religious group. What all of these factors have in common is that they often are strongly associated with different levels of social advantage or privilege as characterized by wealth, power, and/or prestige (8).
From these definitions and the discussion I have given, it is clear that equity is conceptually distinct from equality.
Achieving equity
Since racism is a cause of health problems, then by eliminating racism, we can then ensure health equity. CRT is a “race-equity methodology” (Ford and Airhihenbuwa, 2010), and so, by applying CRT to issues of public health, and by attempting to ameliorate racist attitudes which can and do get “under the skin” to cause differences in physiology (see Sullivan, 2015), then if we eliminate racist attitudes, then we can begin to achieve racial equity. We know that experiencing racism causes accelerated biological aging (i.e., shorter telomere length; Shammas, 2012) and we know that black women in the 47-55 age group were 7.5 years “biologically older” than white women (Geronimus et al, 2011). Thus, racism is a driver of racial health disparities and if we are to achieve racial equity, then we need to eliminate racism. We can use the framework of CRT (which accepts race as a social construct) to understand how and why racist attitudes are had and how and why they are driven by ignorance. Experiencing racist attitudes changes physiology and makes it more likely for the one experiencing the racist attitude to acquire disease states in the future, which would have been a direct outcome of experiencing racist attitudes.
If systemic biases are removed against certain groups (like how doctors are hold unconscious biases against blacks; Hoberman, 2012, and like how medical students believe that blacks have a higher threshold for pain; Hoffman et al, 2012), then we can achieve health equity. If health EQUITY is the ABSENCE OF systemic health disparities (differences in health between and within groups that are unfair, avoidable, and unjust), then we achieve health equity by eliminating systemic health disparities—that is, disparities caused by racism and disparities caused by social determinants of health (Braveman and Gruskin, 2003). Once all groups are not impeded by social goings-on (like living in food deserts/swamps which predict obesity; Cooksey-Stowers, Schwartz, and Brownell, 2017) that force them to not be their best, then we will have achieved ‘equity.’
When public health researchers speak of health equity, they are not operating under the assumption that they will equalize outcomes within and between groups. They are operating under the assumption that they will need to bring down the barriers that impede one to be the healthiest person they can be. In all of my years reading public health research, I have never once read a call for EQUALITY in health; this is just not a feasible position. But EQUITY in health is, and once we begin to change what causes INEQUITIES (health, educational—any kind), then people are no longer held back by (social) circumstances outside of their control, impeding their health, education, etc.
Conclusion
Therefore, the distinction between “equity” and “equality” is: “equality” is making everyone the same or ensuring they get the same things, whereas “equity” is ensuring that people are not held back to be the best person they can be. The distinction between the two concepts that I have drawn up here is very clear. Achieving equity—real equity and not the Lindsay-Rufo strawconcept—is a moral imperative and we, indeed, should attempt it. But achieving equality is just not possible; we would pretty much need to level-down higher groups. The point is, social factors (like racism) should not impede people to be their best and so, we need to eliminate factors that lead to INEQUITIES of ANY kind—be it in public health, education—to achieve a just society. Really loosely, equity can be said to be about fairness but it is more complicated than that, as Braveman’s conceptual discussions show.
All in all, we live in a racist society and racist attitudes affect health which lead to health inequities—that is, differences that cannot be said to be biological; they are differences between social groups that are unfair, unjust, and avoidable and to change these health inequities between social groups (i.e., races, social classes), then people’s attitudes need to change, as the one who is affected by the attitudes physiology can change based on how they take certain statements. Differences between groups that have arisen as part of their position in society that then cause differences in social outcomes are completely avoidable, like differences in obesity between social classes and races (their access to food is impeded by societal factors). And so, to achieve equity—that is, social justice—then we must eliminate any and all systemic barriers that cause said health inequities within and between groups. Equity in health and education are good things, and to strive to reach these goals, we need to change our attitudes as a society towards certain groups. We need to do what we can to achieve feasible goals to ensure that everyone is as healthy as physically possible and that people are not unhealthy due to systemic reasons.
An amputation is a preventative measure. It is done for a few reasons: To stop the spread of a gangrenous infection and to save more of a limb after there is no blood flow to the limb after a period of time. Other reasons are due to trauma and diabetes. Trauma, infection, and diabetes are leading causes of amputation in developing countries whereas in developed countries it is peripheral vascular disease (Sarvestani and Azam, 2013). Poor circulation to an affected limb leads to tissue death—when the tissue begins turning black, it means that there is no or low blood flow to the tissue, and to save more of the limb, the limb is amputated just above where the infection is. About 1.8 million Americans are living as amputees. After amputation, there is a phenomenon called “phantom limb” where amputees can “feel” their limb they previously had, and even feel pain to it, and it is very common in amputees; about 60-80 percent of amputees report “feeling” a phantom limb (see Collins et al, 2018; Kaur and Guan, 2018). The sensation can occur either immediately after amputation or years after. Phantom limb pain is neuropathic pain—a pain that is caused by damage to the somatosensory system (Subedi and Grossberg, 2011). Amputees even have shorter lifespans. When foot-amputation is performed due to uncontrolled diabetes, mortality ranges between 13-40 percent for year one, 35-65 percent for year 3, and 39-85 percent in year 5 (Beyaz, Guller, and Bagir, 2017).
Race and amputation
Amputation of the lower extremities are the most common amputations (Molina and Faulk, 2020). Minority populations are less likely to receive preventative care, such as preventative vascular screenings and care, which leads to them being more likely to undergo amputations. Such populations are more likely to suffer from disease of the lower extremities, and it is due to this that minorities undergo amputations more often than whites in America. Minorities in America—i.e., blacks and “Hispanics”—are about twice as likely as whites to undergo lower-extremity amputation (Rucker-Whitaker, Feinglass, and Pearce, 2003; Lowe and Tariman, 2008; Lefebvre and Lavery, 2011; Mustapha et al, 2017; Arya et al, 2018)—so it is an epidemic for black America. Blacks are even more likely to undergo repeat amputation (Rucker-Whitaker, Feinglass, and Pearce, 2003). In fact, here is a great essay chronicling the stories of some double-amputee black patients.
Why do blacks undergo amputations more often than whites? One answer is, of course: Physician bias. For example, after controlling for demographic, clinical, and chronic disease status, blacks were 1.7 times more likely than whites to undergo lower-leg amputations (Feinglass et al, 2005; Regenbogen et al, 2007; Lefebvre and Lavery, 2011). What is a cause of this is inequity in healthcare—note that “inequity” here means differences in care that are avoidable and unjust (Sudana and Blas, 2013).
Another reason is due to complications from diabetes. Blacks have higher rates of diabetes than whites (Rodriguez and Campbell, 2007) but see Signorello et al (2007). Muscle fiber differences between races (see also here). Differences in hours-slept between blacks and whites, too, could also explain the severity of the disease. But what could also be driving differences in diabetes between races is the fact that blacks are more likely than whites to live in “food swamps.” Food swamps are where it is hard to find nutritionally-dense food, whereas food deserts are areas where there is little access to healthy, nutritious food. In fact, a neighborhood being a food swamp is more predictive of obesity status of the population in the area than is its being a food desert (Cooksey-Stowers, Schwartz, and Brownell, 2017). Along with the slew of advertisements in that are directed to low-income neighborhoods (see Cassady, Liaw, and Miller, 2015), we can now see how such things like food swamps contribute to high hospitalization rates in low-income neighborhoods (Phillips and Rogriguez, 2019). These amputations are preventable—and so, we can say that there is a lack of equity in healthcare between races which leads to these different rates in amputation—before even thinking about physician bias. Amputation rates for blacks in the southeast can be almost seven times higher than other regions (Goodney et al, 2014).
Our study demonstrates that such justifications may be unevenly applied across race, suggesting an underlying bias. This may reflect a form of racial paternalism, the general societal perception that minorities are less capable of “taking care of themselves,” even including issues related to health and disease management.23 Underlying bias may prompt more providers to consider amputation for minority patients. Furthermore, unlike in transplant surgery, there is currently no formal process for assessing patient compliance with treatment protocols or self-care in vascular surgery.24 Asking providers to make snap judgments about patient compliance, without a protocol for objective assessment, allows subconscious bias to influence patient care.
Physician bias is pervasive (Hoberman, 2012)—whether it is conscious or unconscious racial bias. Such biases can and do lead to outcomes that should not occur. By attempting to reduce disparities in healthcare that then lead to negative outcomes, we can then attempt to improve the quality of healthcare given to lower-income groups, like blacks. Such biases lead to negative health outcomes for blacks (such as the claim that blacks feel less pain than whites), and if they were addressed and conquered, then we could increase equity between groups until access to healthcare is equal—and physician bias is an impediment to access to equal healthcare due to the a priori biases that physicians may hold about certain racial/ethnic groups. Medical racism, therefore, drives a lot of the amputation differences between blacks and whites. Hospitals that are better equipped to offer revascularization services (attempting to save the limb by increasing blood flow to the affected limb) even had a higher rate of amputations in blacks when compared to whites (Durazzo, Frencher, and Gusberg, 2013).
Compared to Caucasian patients, several studies have found that African-Americans with PAD are more likely to be amputated and less likely to have their lower limb revascularized either surgically or via an endovascular approach [3–9]. In an early analysis of data from acute-care hospitals in Florida, Huber et al. reported that the incidence of amputation (5.0 vs. 2.5 per 10,000) was higher and revascularization lower (4.0 vs. 7.1 per 10,000) among African-Americans compared to Caucasians, even though the incidence of any procedure for PAD was comparable (9.0 vs. 9.6 per 10,000) [4]. Other studies have reported that the probability of undergoing a revascularization or angioplasty was reduced by 28–49 % among African-Americans relative to Caucasians [3 6]
There is evidence of both healthcare provider racism and unconscious racial biases. Green et al. found significant pro-White bias among internal medicine and emergency medicine residents, while James SA supported this finding, indicating a “pro-white” unconscious bias in physician’s attitudes towards, and interactions with, patients [43,44]. In a survey assessing implicit and explicit racial bias by Emergency Department (ED) providers in care of NA children, it was discovered that many ED providers had an implicit preference for white children compared to those who identified as NA [45]. Indeed, racism and stigmatization are identified as being many American Indians’ experiences in healthcare.
One major cause of the disparity is that blacks are not offered revascularization services at the same rate as whites. Holman et al (2011: 425) write:
Finally, given that patients’ decisions are necessarily confined to the options offered by their physicians, racial differences in limb salvage care might be attributable to differences in physician decision making. There are some data to suggest lower vein graft patency rates in black patients compared to whites.18,19 A patient’s race, therefore, may influence a vascular surgeon’s judgment about the efficacy of revascularization in preventing or delaying amputation. Similarly, a higher proportion of black patients in our sample were of low SES, which correlates with tobacco use,20-22 and we know that continued tobacco use increases the risk of lower extremity graft failure approximately three-fold.23 It is possible that a higher proportion of black patients in our sample were smokers who refused to quit, in which case vascular surgeons would be much less likely to offer them the option of revascularization. While Medicare data include an ICD-9 diagnosis code for tobacco use, the prevalence in our study sample was approximately 2%, suggesting that this code was grossly unreliable as a means of directly measuring and adjusting for tobacco use.
Smoking, of course, could be a reason why revascularization would not be offered to black patients. Though, as I have noted, smoking ads are more likely to be found in lower-income neighborhoods which increases the prevalence of smokers in the community.
With this, I am reminded of two stories I have seen on television programs (I watch Discovery Health a lot—so much so that I have seen most of the programs they show).
In Untold Stories of the ER, a man came in with his hand cut off. He refused medical care. He would not let the doctors attempt to sew his hand back on. Upon the police entering his home to check for evidence (where his hand was found), they searched his computer. It seems that he had a paraphilia called “acrotomophilia” which is where one is sexually attracted to people with amputations. Although he wanted it to be done to himself—he had inflicted the wound on himself. After the doctor tried to reason with the man to have his hand sewed back on, the man would not let up. He did not want his hand sewed back on. I wonder if, years down the line, the man regretted his decision.
In another program (Mystery Diagnosis), a man had said that as a young boy, he had seen a single-legged war veteran amputee. He said that ever since then, he would do nothing but think about becoming an amputee. He lived his whole life thinking about it without doing anything about it. He then went to a psychiatrist and spoke of his desire to become an amputee. After some time, he eventually flew to Taiwan and got the surgery done. He, eventually, found happiness since he had done what he always wanted to.
While these stories are interesting they speak to something deep in the minds of the individuals who mutilate themselves or get surgery to otherwise healthy limbs.
Conclusion
Blacks are more likely than whites to receive amputations in affected limbs than whites and are less likely to receive treatments that may be able to save the affected limb (Holman et al, 2011; Hughes et al, 2013; Minc et al, 2017; Massada et al, 2018). Physician bias is a large driver of this. So, to better public health, we then must attempt to mitigate these biases that physicians have that lead to these kinds of disparities in healthcare. Medical and other kinds of racism have led to this disparity in amputations between blacks and whites. Thus, to attempt to mitigate this disparity, blacks must get the preventative care needed in order to save the affected limb and not immediately go for amputation. Thankfully, such disparities have been noticed and work is being done to decrease said disparities.
So race is a factor in the decision on whether or not to amputate a limb, and blacks are less likely to receive revascularization services.
‘Health inequalities are the systematic, avoidable and unfair differences in health outcomes that can be observed between populations, between social groups within the same population or as a gradient across a population ranked by social position.’ (McCartney et al, 2019)
Health inequities, however, are differences in health that are judged to be avoidable, unfair, and unjust. (Sudana and Blas, 2013)
Asking “Is X racist?” is the wrong question to ask. If X is factual, then making the claim cannot be racist (facts themselves cannot be racist). But, one can perform a racist action—either consciously or subconsciously—on the basis of a fact. Facts themselves cannot be racist, but one can use facts to be racist. One can hold a belief and the belief can be racist (X group is better than Y group at Z), but systemic racism would be the result (the outcome) of holding said belief. (Some examples of systemic racism can be found in Gee and Ford, 2011.) Someone who holds the belief that, say, whites are more “intelligent” than blacks or Jews are more “intelligent” than whites could be said to be racist—they hold a racist belief and are making an invalid inference based on a fact (blacks score 15 points lower in IQ tests compared to whites so blacks are less intelligent). Truth cannot be racist, but truth can be used to attempt to justify certain policies.
I have argued that we should ban IQ tests on the basis that, if we believe that the hereditarian hypothesis is true and it is false, then we can enact policies on the basis of false information. If we enact policies on the basis of false information, then certain groups may be harmed. If certain groups may be harmed, then we should ban whatever led to the policy in question. If the policy in question is derived from IQ tests, then IQ tests must be banned. This is one example on how we can use a fact (like the IQ gap between blacks and whites) and use that fact for a racist action (to shuttle those who perform under a certain expectation into certain remedial classes based on the fact that they score lower than some average value). Believing that X group has a higher quality of life, educational achievement, and life outcomes on the basis of IQ scores—or their genes—is a racist belief but this racist belief can then be used to perform a racist action.
I have also discussed different definitions of “racism.” Each definition discussed can be construed as having a possible action attached to it. Racism is an action—something that we perform on the basis of certain beliefs, motivated by “what can be” possible in the future. Beliefs can be racist; we can say that it is an ideology that one acts on that has real causes/consequences to people. Truth can’t be racist; people can can use the truth to perform and justify certain actions. Racism, though, can be said to be a “cultural and structural system” that assigns value based on race; further, actions and intent of individuals are not necessary for structural mechanisms of racism (e.g., Bonilla-Silva, 1997).
We can, furthermore, use facts about differences between races in health outcomes and say that certain rationalizations of certain outcomes can be construed as racist. “It’s in the genes!” or similar statements could be construed as racist, since it implies that certain inequalities would be “immutable” on the basis of a strong genetic determination of disease.
Racism is indeed a public health issue. For instance, physicians can hold biases on race—just like the average person. For instance, differences in healthcare between majority and minority populations can said to be systemic in nature (Reschovsky and O’Malley, 2008). This needs to be talked about since racism can and is a determinant of health—as many places in the country are beginning to recognize. Racism is rightly noted as a public health crisis because it leads to disparate outcomes between whites and blacks based on certain assumptions on the ancestral background of both groups.
Quach et al (2012) showed that not receiving referrals to a specialist is discriminatory—Asians, too were also exposed to medical discrimination, along with blacks. Such discrimination can also lead to accelerated cellular aging (on the basis of measured telomere lengths where shorter telomeres indicate a higher biological compared to chronological age; Shammas et al, 2012) in black men and women (Geronimus et al, 2006; 2011; Schrock et al, 2017; Forrester et al, 2019). We understand the reasons why such discrimination on the basis of race happens, and we understand the mechanism by which it leads to adverse health outcomes between races (chronic elevation in allostatic load leading to higher than normal levels of certain stress hormones which will, eventually, lead to differences in health outcomes).
The idea that genes or behavior lead to differences in health outcomes is racist (Bassett and Graves, 2018). This can then lead to racist actions—that their genetic constitution impedes them from being “near-par” with whites, or that their behavior is the cause of the health disparities (sans context). Valles (2018: 186) writes:
…racism is a cause with devastating health effects, but it manifests via many intermediary mechanisms ranging from physician implicit biases leading to over-treatment, under-treatment and other clinical errors (Chapman et al. 2013; Paradies et al. 2015) to exposing minority communities to waterborne contaminants because of racist political disenfranchisement and neglect of community infrastructure (e.g., the infamous Flint Water Crisis afflicting my Michigan neighbors) (Krieger 2016; Sherwin 2017; Michigan Civil Rights Commission 2017).
There is a distinction between “equity” and “equality.” For instance, to continue with the public health example, take public health equality and public health equity. In this instance, “equality” means giving everyone the same thing whereas “equity” means giving individuals what they need to be the healthiest individual they can possibly be. “Strong equality of health” is “where every person or group has equal health“, while weak health equity “states that every person or group should have equal health except when: (a) health equality is only possible by making someone less healthy, or (b) there are technological limitations on further health improvement” (Norheim and Asada, 2009). But we should not attempt to “level-down” people’s health to achieve equity; we should attempt to “level up” people’s health, though. That is, it is impossible to reach a strong health equality (making all groups equal), but we should—and indeed, have a moral responsibility to—attempt to lift up those who are worse-off. Poverty is what is objectionable, inequality is not. It is impossible to achieve true equality between groups, but we can—and indeed we have a moral obligation to—lift up those who are in poverty, which is, also a social determinant of health (Braveman and Gottlieb, 2014; Frankfurt, 2015; Islam, 2019).
We achieve health equity when all individuals have the same access to be the healthiest individuals they can be; we achieve health equality when all health outcomes are the same for all groups. Health equity is, further, the absence of avoidable differences between different groups (Evans, 2020). One of these is feasible, the other is not. But racism does not allow us to achieve health equity.
The moral foundation for public health thus rests on general obligations in beneficence to promote good health. (Powers and Faden, 2006: 24)
Social justice is not only a matter of how individuals fare, but also about how groups fare relative to one another whenever systemic racism is linked to group membership. (Powers and Faden, 2006: 103)
…inequalities in well-being associated with severe poverty are inequalities of the highest moral urgency. (Powers and Faden, 2006: 114)
Public health is directly a matter of social justice. If public health is directly a matter of social justice, and if health outcomes due to discrimination are caused by social injustice, then we need to address the causes of such inequalities, which would be for example, conscious or unconscious prejudice against certain groups.
Certain inequalities between groups are, therefore, due to systemic racism which is an action which can be conscious or unconscious. But which inequalities matter most? In my view, the inequalities that matter most are inequalities that impede an individual or a group from having a certain quality of life. Racism can and does lead to health inequalities and by addressing the causes for such actions, we can then begin to ameliorate the causes of structural racism. This is more evidence that the social can indeed manifest in biology.
Holding certain beliefs can lead to certain actions that can be construed as racist and negatively impact health outcomes for certain groups. By committing ourselves to a framework of social just and health, we can then attempt to ameliorate inequities between social class/races, etc. that have plagued us for decades. We should strive for equity in health, which is a goal of social justice. We should not believe that such differences are “innate” and that there is nothing that we can do about group differences (some of which are no doubt caused by systemically racist policies). Health equity is something we should strive to do and we have a moral obligation to do so; health equality is not obligatory and it is not even a feasible idea.
If we can avoid health certain outcomes for certain groups on the basis of beliefs that we hold, then we should do so.
I’m currently reading Health Disparities in the United States: Social Class, Race, Ethnicity and Healthby medical doctor and sociologist Donald Barr. In the book, he chronicles differences in health between races and ethnies, talks about the concepts of race used and cites well-known studies to people who read this blog, and he also shows that doctors are—either conscious or not—biased against minorities in certain medical contexts.
In Chapter 1 discusses the fact that, although Americans spend the most money on health care, Americans have a lower life expectancy and higher infant mortality rate than all other developed countries, showing the association in social inequality and health across all income levels and education. In Chapter 2, he asks the question “What is health?”, discussing many concepts of what “health” is. In Chapter 3, he defines “socioeconomic status” and shows the link between poor health and poor SES. In Chapter 4, he discusses the link between inequality and poor health, introducing the concept of “allostatic load”, which is the physiologic response to being in a spot of social disadvantage.
In Chapter 5, he looks at different race concepts, since it is a main premise of the book. In Chapter 6, he shows that minorities are more likely to be in a position of low SES. He asks, if minorities of the same SES as whites are consistently found to be of lower health than whites of the same SES, is it because those with poor health tend to be minorities, that they tend to have lower SES or both? In Chapter 7, he asks the same questions while focusing on children. In Chapter 8, he examines disparities in access to healthcare, showing that even when minorities have the same insurance and doctors that minorities still face worse health outcomes (he shows that they either do not receive appropriate healthcare or receive lower-quality care). In Chapter 9, he shows that physicians treat blacks and other minorities differently, albeit unconsciously. In Chapter 10, he discusses when—if ever—a physician would be justified in using racial/ethnic categories. And in Chapter 11, he states that not all of these disparities need to be eliminated.
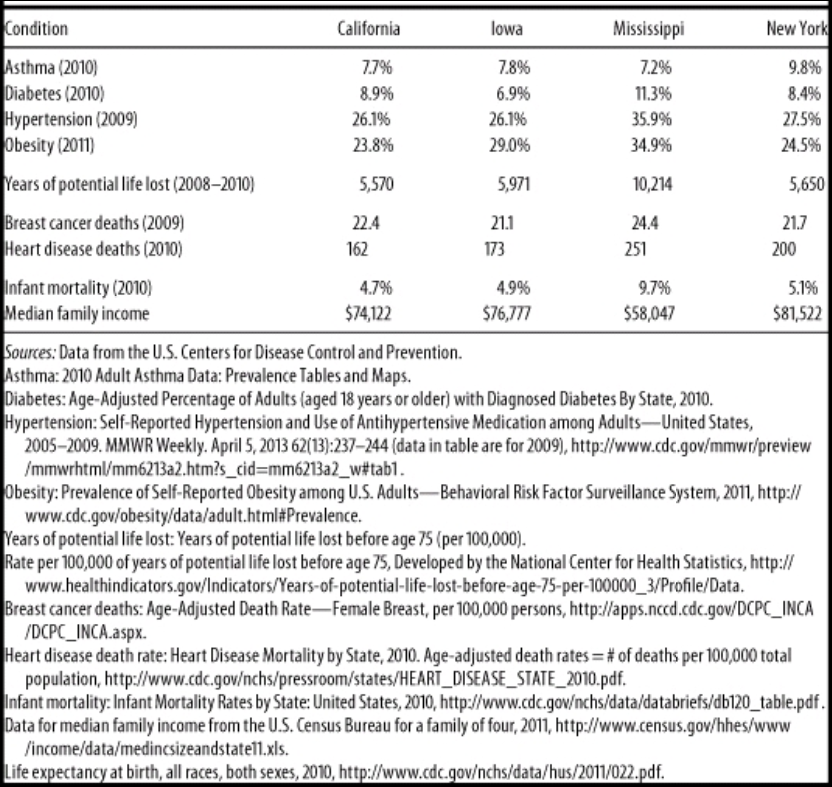
In Chapter 2, Barr (2014: 45) presents this table, showing rates of illness and selective rates of death between States in America. Obviously, the one to look at that is different than the others is Mississippi. Mississippi is 37.5% black.
Wow, I wonder why Mississippi has such a high rate of obesity, diabetes, and hypertension (high blood pressure). Must be all of those obesity, diabetes and hypertension genes (HBDer).
Obesity and diabetes
The first thing to look at is median income. It is substantially lower in Mississippi compared to California, Iowa, and New York. About 23 million people in America live one mile from a supermarket, while black Americans are about half as likely to have access to supermarkets while “Hispanics” are about a third likely to have access to them (New York Law School Racial Justice Project, 2012). So when it comes to those who have to travel more than a mile for fresh fruit and vegetables, they have poorer health (Stack, 2015). So combine lower median income, along with food deserts and one can start to see how minorities have poorer health due in part to their SES. In short, living in a food desert can affect public health.
Blacks are the most obese ethnic group in America, and this relationship is largely driven by black women. Now, it’s not weird that women have higher levels of body fat than men, since women it is needed for physiological functioning. Though, there is something weird here: Black American men with more African ancestry are less likely to be obese (Klimentidis et al, 2016). Since black women and black men in America are in the same economic bracket, there must be something in the West African male physiology that “protects” them against central adiposity, though variation in social, environmental and cultural factors may play a role as well. In any case, the more West African ancestry American blacks have, the less likely they are to be obese. Klimentidis et al’s (2016) study “suggests that there are specific genetic variants and physiological mechanism(s) that differ among West African and European populations.”
Obesity affects more ethnies in America than others: non-Hispanic blacks and “Hispanics” are more likely to be obese than non-“Hispanic” whites and Asians (Hales et al, 2017). This could be due to, in part, to the variation in supermarket access and access to good foods—the concept of food deserts. Look at any low-income area near you. You’ll see a majority of corner stores with cheap, garbage food. The lack of ability to buy good food (along with the education to know what to buy and when to buy it) can explain differences in obesity rates—obviously not all. Obesity is related with diabetes, and sinec the relationship is so strong, the term “diabesity” was coined.
Eating cheap, processed carbohydrates spikes insulin. Repeated insulin spikes over time leads to type II diabetes and, eventually, obesity too. One can be skinny and have diabetes (a phenomenon known as thin on the outside, fat on the inside “TOFI”). However, since both diseases are co-morbid, we need to look at them in similar contexts. The higher rates of obesity can help to explain the higher rates of diabetes and hypertension—since those who are obese have higher blood pressure (Aronow, 2017).
Minorities are more likely to develop type II diabetes (Tuchman, 2011), and the cause of this is access to high-quality foods. But racial differences in obeisty and SES do not fully explain the higher rates of type II diabetes in black Americans; being a black American is a strong, independent factor for developing type II diabetes and this is compounded by low SES (Brancati et al, 1996). Zizi et al (2016) showed that both long and short black sleepers have an increased risk of developing type II diabetes. There are racial differences in sleep, with blacks having higher durations of long and short sleep compared to whites (Adenekan et al, 2013).
Hypertension
Now let’s look at hypertension (blood pressure). Blood pressure is a physiological variable. Since it is a physiological variable, it can and does respond to social/environmental contexts. So blood pressure can be affected by social contexts, too. For example, Williams (1992) cites stress, socioecologic stress, social support, coping patterns, health behavior, sodium and more for reasons why blacks have higher BP than whites. Dressler (1991) shows that the struggle to maintain a middle-class lifestyle is related to higher levels of BP. Similarly, Keith and Herring (1991) show that skin color is a strong predictor of occupational status and that darker-skinned blacks in America are twice as likely to experience racial discrimination than lighter-skinned blacks. This, too, can help to account for higher levels of BP between the races. In any case, Williams (1992) shows, definitively, that the causes of black-white differences in BP lie in the social environment.
Similarly, Non, Gravlee, and Mulligan (2012) show that racial disparities in BP are explained by education, and not genetic ancestry. They show that the association between BP and education was much stronger for blacks than for whites. Their results also support “the minority poverty hypothesis because the worst blood pressures were predicted for people who faced the double burden of being less educated and identifying as African American.” People who face discrimination could, and do, have higher levels of BP due to the stress they feel due to the discrimination. (Note that I take no sides on whether the discrimination is real or imagined, because even if it were imagined, it still leads to real physiologic consequences.)
Do note that there is a just-so story to explain how and why blacks have higher levels of blood pressure than whites: The Slavery Hypertension Hypothesis (Lujan and Dicarlo, 2018). This has all of the hallmarks of a just-so story posited by evolutionary psychologists. The story goes like this: Black slaves who were on the way to America in the Middle Passage had genes that favored better salt retention. So it is noted that black Americans have higher rates of BP than whites, and then they work backward and attempt to posit the best story possible to explain the current-day observation. This is the usual method evolutionary psychologists use—the method of reverse engineering, the inference from function to cause. So (1) note that blacks have higher levels of BP than whites; (2) infer the function to cause (blacks with genes that favored salt retention were more likely to survive; so (3) this is why blacks have higher rates of BP than whites. Though the explanation fails, since education, and not genetic ancestry, explains the difference in BP between blacks and whites (Non, Gravlee, and Mulligan, 2012). One only needs to understand the intricacies of physiology and how our physiological systems respond to what occurs in the greater environment.
So, obesity can explain both the higher rates of diabetes and higher rates of blood pressure, with differences in the immediate social environment explaining the rest of the differences in blood pressure between blacks and whites. (Note that heart disease deaths are directly related to hypertension. Heart disease affects blacks more than whites.)
Black women are more likely to die from breast cancer, for example, and racism seems like it can explain a lot of it. They have less access to screening, treatment, care, they receive delays in diagnoses, along with lower-quality treatment than white women. But “implicit racial bias and institutional racism probably play an important role in the explanation of this difficult treatment” (Hardimon, 2017: 166). Furthermore, black women are more than twice as likely to acquire a type of breast cancer called “triple negative” breast cancer (Stark et al, 2010; Howlader et al, 2014; Kohler et al, 2015; DeSantis et al, 2019). Of course, this could be a relevant race-related genetic difference in disease.
Infant mortality
Now note the infant mortality rate between the states: the infant mortality rate in Mississippi is 9.7%. Smith et al (2018) show that black women are at a higher rate of having their infant die at birth. Pre-term births are related to low birth weights, and they both are related to infant mortality. Matoba and Collins (2017) write:
In the United States, African-American infants have significantly worse infant mortality than white infants. Individual risk factors alone do not explain this persistent gap, just as they did not explain the disparity in preterm birth and low birth weight. Recent studies in social determinants provide insight into the contribution of community and environmental factors to the racial disparity. Select community-level factors are potential, but partial, determinants of the racial disparity. Interpersonal and institutionalized racism is an important, and increasingly recognized, stressor for African-American women with damaging consequences to maternal and child health.
The Guardian ran a recent story on infant mortality and race, positing racism as a cause of the disparity. In any case, the social environment can and does play a part in everything discussed here today since the social can and does become biological. Part of the reason why Mississippi has a way higher rate of years of potential life lost (10,214 compared to 5500-5900 for Iowa, New York, and California) is that rates of infant mortality are higher in Mississippi. So the median age of death is 75. If an infant dies at one year of age, then that is 74 years of life lost. Therefore it is not surprising that the State with the highest level of infant mortalities has a higher number of years of potential life lost. Further, one 2017 review found that segregation was associated with increased risk of preterm birth and low birth weight for blacks (Mehra, Boyd, and Ickovis, 2017)
Note how Mississippi has lower rates of asthma. This is explained by the fact that Mississippi is more rural than, say New York. Rates of asthma are associated with living in a metropolitan area (Frazier et al, 2012; Malik, Kumar, and Frieri, 2012). (Note that blacks and other races have higher rates of asthma than other races.)
Physician bias
The lower one’s position is on the social hierarchy the lower their probability of staying healthy and having a high life expectancy; when people have the same type of health insurance and are treated for the same disease in the same hospital by the same doctor, that minority groups get worse health care, either not receiving it or receiving lower standards of quality in care. What could account for such disparities? I asked PumpkinPerson the question, and he said:
1) EGI: Doctors put more effort into saving coethnics: she looks like my italian grandma. I’ll make sure she gets the best medicine.
2) IQ: low IQ populations don’t understand the doctor’s advice and damage their health
3) r/K: some populations have faster life history so don’t live as long, even with good medical care
If (1), then the doctors need to be named, shamed, and have their medical licenses revoked. If (2), then they need better education (since IQ is just an index of middle-class knowledge). (3) is completely irrelevant, since it doesn’t make sense for humans and the concept is long-dead in ecology. In any case, PumpkinPerson danced around the true cause: differences in healthcare brought about by unconscious bias (of which (1) may be a cause). But positing (1) as a cause completely misses the point (and is the usual HBDer reductionism to genes causing most/if not all things). It’s the usual HBD/Rushtonian reductionism to genes. That’s all the HBD worldview reduces to: genes/IQ.
Our results indicate that the minority makeup of physicians’ patient panels is associated with greater reports from physicians of difficulties providing high-quality care. At least some of this relationship appears to be explained by the lower resources flowing to high-minority practices.
The results of this study suggest that racial and ethnic disparities in primary health care are in part systemic in nature, and the lower resources flowing to physicians treating more minority patients are a contributing factor.
Thus, bias—whether conscious or unconscious—by physicians can explain how and why there are differences in health outcomes between people that have the same health insurance and doctor. Barr (2014: 168) states that “for black Americans, where a person lives sems to be associated with access to primary care, the quality of available hospital care, and the quality of available home care.” Barr shows that blacks receive a different level of care for a wide-range of diseases and illnesses compared to whites. For instance, Smedley et al (2003) write that “some evidence suggests that bias, prejudice, and stereotyping on the part of healthcare providers may contribute to differences in care.” Quite clearly, there is racial bias against minorities and it does seem to affect healthcare, whether or not it is intended or unintended (conscious or unconscious) (Williams and Rucker, 2000). Bird and Clinton (2001: 255) write:
Race and class-based structuring of the U.S. health delivery system has combined with other factors, including physicians’ attitudes—perhaps legacies conditioned by their participation in slavery and creation of the scientific myth of black biological and intellectual inferiority—to create a medical-social, health system cultural, and health delivery environment which contributes to the propagation of racial health disparities, and, ultimately, the health system’s race and class dilemma.
Blacks are more likely to take the advice of physicians, and to use the needed services, such as preventative care and are less likely to delay seeking care when the physician is of their own race (Saha et al, 2000; LaVeist, Nuru-Jeter, and Jones, 2008).
Blacks are more likely to perceive racism in healthcare and when they are able to choose their own doctors, they are more satisfied with their level of care (Chen et al, 2005). Chapman, Kaatz, and Carnes (2013) show that increasing awareness of implicit bias in healthcare can lower such disparities, stating that having more black doctors will alleviate such problems since they are less likely to be biased. Having a black doctor lead to more effective care for black men. Quite clearly, the race of the doctor matters for implicit biases and minority doctors lead to more effective healthcare for minorities, since they are less likely to be affected by racial biases. Minorities trust the healthcare system less than whites (Boulware et al, 2003). Black and white physicians even agree that race is a medically relevant data point, but do not agree on why (Bonham et al, 2009).
Conclusion
The table presented by Barr is telling. He purported to show that on certain indices of health, certain states fair worse than others. Rates of illness and rates of death between different states (with differing ethnic compositions) were compared. Using national data, he showed that Mississippi has the highest rates of death and illness (sans asthma). Social factors can and do account for the differences in hypertension between blacks and whites (and States); food deserts (lack of access to good food) can explain higher rates of obesity and diabetes and also higher rates of blood pressure between the races (and States with a higher percentage of certain racial/ethnic groups). Of course, physiological variables are affected by the social environment, so we have to look at differences in the social environment between groups to see how and why there are differences in any physiological variable we look at.
Doctors, whether consciously or not, treat minority patients differently and there is evidence that this leads to differences in health outcomes between ethnic groups in America. PP’s hypotheses don’t cut it (the only one that does it his “EGIs”, but that explanation fails; the cause is bias by the doctors but “EGIs” have nothing to do with the bias). In any case, there are social and cultural reasons why there are such health disparities between States and races/ethnies. Understanding the causes behind them can and will lead to closing the gap between them. The social can and does become biological, and this is the perfect way to show this. There are ways to lower the disparities in a medical context, and education seems to be one of them—for both patient and doctor.
Some states are healthier than others based on objective measures of health and mortality, and understanding the reasons why can and will decrease these differences.