
1700 words
There are many superficial physical differences between the races. But differences in pain sensitivity would be one that is not really “superficial”, as you can’t really see it (you can see someone’s reaction to pain, but not see it). “Pain” is defined as physical discomfort caused by injury. There are some myths about pain differences between racial groups, that still persist today. And these myths have bad consequences.
For example, Hoffman et al (2016) state that “people assume a priori that blacks feel less pain than do whites.” Hoffman et al (2016) carried out two studies: (1) using a between-participants design, laymen were asked to assess the pain of white and black subjects and (2) again using a between-participants design, they asked students and medical doctors to assess pain between blacks and whites. In (2) they asked these 15 questions:
1. On average, Blacks age more slowly than Whites.
2. Black people’s nerve-endings are less sensitive than White
people’s nerve-endings.
3. Black people’s blood coagulates more quickly–because of
that, Blacks have a lower rate of hemophilia than Whites.
4. Whites, on average, have larger brains than Blacks.
5. Whites are less susceptible to heart disease like hypertension than Blacks.
6. Blacks are less likely to contract spinal cord diseases like
multiple sclerosis.
7. Whites have a better sense of hearing compared with Blacks.
8. Black people’s skin has more collagen (i.e., it’s thicker) than
White people’s skin.
9. Blacks, on average, have denser, stronger bones than Whites.
10. Blacks have a more sensitive sense of smell than Whites;
they can differentiate odors and detect faint smells better
than Whites.
11. Whites have more efficient respiratory systems than Blacks.
12. Black couples are significantly more fertile than White couples.
13. Whites are less likely to have a stroke than Blacks.
14. Blacks are better at detecting movement than Whites.
15. Blacks have stronger immune systems than Whites and are
less likely to contract colds.
(I’ll cover these questions in a future article.)
Here is the table showing the respondents’ answers to the questions:
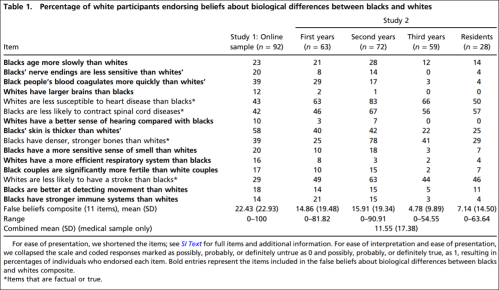
So they established that whites with no medical training hold false beliefs about black-white differences that then carry over to pain management. They showed in study 2 that medical students’ and residents’ apparently false beliefs about racial differences in the questions they answered showed bias in the accuracy of the recommended pain treatments. Hoffman et al (2016) conclude that:
The present work sheds light on a heretofore unexplored source of racial bias in pain assessment and treatment recommendations within a relevant population (i.e., medical students and residents), in a context where racial disparities are well documented (i.e., pain management). It demonstrates that beliefs about biological differences between blacks and whites—beliefs dating back to slavery—are associated with the perception that black people feel less pain than do white people and with inadequate treatment recommendations for black patients’ pain.
(See also the Psychology Today article on the matter.)
Similarly, Hollingshead et al (2016) reported that subjects, regardless of race, rated the white person more sensitive to pain and more likely to report pain than the black person. Whites reported that they were less pain sensitive and less likely to report pain than their peers. Blacks reported that they were more sensitive to pain while reporting more pain than their peers.
Interestingly, Trawalter, Hoffman, and Waytz (2012) state that black NFL players are more likely to play in a subsequent game than whites when injured, and that, as found in many other studies, blacks are more likely to feel less pain than whites. However, what the literature really shows is the opposite: blacks are more likely to feel pain than whites.
Kim et al (2017) showed that blacks, “Hispanics” and Asians had lower pain tolerance, higher pain ratings and greater temporal sensation of pain. They also showed that blacks had lower pain tolerance and higher pain ratings but no differences in pain threshold.
Blacks report greater pain regarding AIDs, glaucoma, migraine, headache, jaw pain, postoperative pain, joint pain and many other types of pain compared to whites (Green et al, 2003; Klonoff, 2009). Riley III et al’s (2002) results indicate that blacks show a stronger link between pain and emotions than whites. Obana and Davis (2016) showed that Native Hawaiian/Pacific Islander male and females reported higher pain scores than whites when it came to joint pain (but they were not significant). Bolen et al (2010) showed that work limitation, severe joint pain, and arthritis-attributable activity were higher for non-“Hispanic” blacks, “Hispanics” and multiracial people compared to non-“Hispanic” whites. Even American Indians, Alaskan natives, and Aboriginal Canadians had a higher prevalence of pain and pain symptoms than Americans (Jimenez et al, 2011).
Chan et al (2011) surveyed older Singaporeans. They found that Malay people had lower pain sensitivity compared to Chinese people, and that Indians reported greater pain sensitivity when compared with Malay and Chinese people. Australian women rated menstrual pain higher and lasting 36 percent longer than Chinese women (Zhu et al, 2010).
When it comes to potential mechanisms, physiological mechanisms are hypothesized by Campbell and Edwards (2012) who write:
For example, in comparison to non-Hispanic whites, African–Americans have reduced nociceptive flexion reflex thresholds [26]; the nociceptive flexion reflex is an electrophysiological, spinally mediated reflex, which is not amenable to voluntary control or subject to issues of response bias that plague self-report of pain experiences. This finding suggests that the observed ethnic differences in pain are unlikely to be fully explainable by sociocultural influences and hints that neurobiological processes may contribute to such differences.
Mossey (2011) shows that “Racial/ethnic minorities consistently receive less adequate treatment for acute and chronic pain than non-Hispanic whites, even after controlling for age, gender, and pain intensity.” Martinez et al (2014) showed that when it comes to colorectal and lung cancer, mixed-race individuals and blacks are more likely to report higher pain severity than whites. (Also see Shavers, Bakos, and Sheppard, 2010.)
All of the literature points in the opposite direction of the myths about pain sensitivity in regard to race: blacks feel more pain than whites and are more likely to have a lower pain tolerance. So the myths people hold about differences in pain between racial groups (mostly blacks and whites) are false. Pain is a subjective experience. And there will be differences in pain thresholds between individuals and racial groups and the causes may be both sociocultural and physiological in nature. However, this bias (in the wrong direction) speaks to what I wrote about last night: physician bias when it comes to blacks and other minorities.
Barr (2014: 183-184) writes:
Based to a certain extent on the attention given to his earlier publication, Todd moved to a faculty position with the Emory University School of Medicine, in Atlanta, Georgia. There he was able to essentially repeat his earlier study, this time examining persons coming tothe emergency room of a large, inner-city community hospital in Atlanta that was affiliated with Emory (Todd et al, 2000). He evaluated the medical records of 217 individuals coming to the emergency room over a 40-month period for treatment of an isolated long-bone fracture. Given the racial makeup of Atlanta, these included 127 blacks and 90 whites. They found that
- 54 of the blacks (43 percent) received no medication for pain during their treatment
- 23 of the whites (26 percent) received no medication for pain during their treatment
As with the earlier study in Los Angeles involving whites and Hispanics, in this study, the blacks were nearly twice as likely to receive no pain medication while in the emergency room. With this study, the authors were keenly aware of the importance of documenting the extent to which the patients expressed painful symptoms. By thoroughly reviewing the medical records of these patients, they found that 54 percent of blacks and 59 percent of whites had a notation in their medical record that they had expressed painful symptoms. The nearly twofold difference in withholding pain medication in blacks and whites was because the doctor didn’t order the medication, not because the patient didn’t want the medication.
This, again, speaks to physician bias when it comes to race in a medical context. Race is a useful tool in medicine, but to hold biases in the complete opposite direction that they exist in is wrong. This study—and many others—speak to the type of bias that physicians have against minorities in a medical context. Understanding that the differences in pain are actually the opposite from what is commonly believed by both laypeople and medical doctors is important: if blacks feel more pain than whites regarding the same injuries and they are not getting the care needed, then this speaks to physician bias. What Barr showed was that blacks were treated at the emergency room based on their ethnicity. This is wrong. Race/ethnicity is a useful tool in medicine, but to outright use it as an assumption for numerous factors makes no sense and could cause more harm than good.
Using race in a medical context is a good thing. But using race in a medical context using essentialist, outdated views about race is wrong and can lead to many horrible outcomes. Of course, using race in this context can and does lead to certain things being discovered over others. For instance, if one’s race is assumed to be “driving” one’s illness (i.e., that one has a disease that that race/ethny is more likely to have), then race can and is a good marker to use—specifically geographic ancestry. However, when it comes to things like pain management, this obviously leads to false ideas about how different groups manage and feel pain.
Views about racial differences in pain affect both laypeople and medical doctors. These views can be and are harmful. The literature points to the case being the opposite of what is believed by people: blacks have lower pain tolerance and higher pain ratings than whites. These types of differences are also found between many other races and ethnic groups. The causes could be both sociocultural and physiological. A person’s response to pain depends on their unique physiology, life experiences, ethnicity and other factors. Understanding how and why physicians are biased toward how blacks feel pain is important, along with addressing the other biases that they have about other minorities when it comes to a medical context. Race and ethnicity are important tools for medicine, but these are some of the ways that the concepts can be used with nothing good coming out of it.

The bias that is truest is the most rejected by the PC respondents.
LikeLike