
Home » Prostate Cancer
Category Archives: Prostate Cancer
Race and Vitamin D Deficiency
1600 words
Vitamin D is an important “vitamin” (it is really a steroid hormone). It is produced when the skin (the largest organ in the body) is exposed to the sun’s UVB rays (Nair and Maseeh, 2012). So this is one of the only ways to get natural levels of UVB. We can then think that, if a population is outside of its natural evolutionary habitat (the habitat where that skin color evolved), then we should note numerous problems caused by the lack of vitamin D in whichever population is studied outside of a location that doesn’t get the correct amount of UVB rays from the sun.
Black Americans are more likely than other ethnies to be deficient in vitamin D (Harris, 2006; Cosman et al, 2007; Nair, 2012; Forest and Stuhldreher, 2014; Taksler et al, 2014). But, paradoxically, low vitamin D levels don’t cause weaker bones in black Americans (O’Conner et al, 2014). However, like with all hypotheses, there are naysayers. For example. Powe et al (2013) argue that vitamin D tests misdiagnose blacks, that blacks have a form of the vitamin that cells can use called 25-hydroxyvitamin D. They conclude: “Community-dwelling black Americans, as compared with whites, had low levels of total 25-hydroxyvitamin D and vitamin D–binding protein, resulting in similar concentrations of estimated bioavailable 25-hydroxyvitamin D. Racial differences in the prevalence of common genetic polymorphisms provide a likely explanation for this observation.” Though there are a whole host of problems here.
The limitations of Powe et al (2013) striking: it was cross-sectional and observational (like most nutrition studies) so they were unable to predict effects of vitamin-D binding protein on bone fractures; no data on the consumption of vitamin D supplements; measurement of bone turnover markers, urinary calcium excretion and levels of 1,25-dihydroxyvitamin D may explain the effect of VDBP (vitamin D-binding protein) on mineral metabolism; and they relied on a calculation, rather than a measurement of 25-hydroxyvitamin D levels.
Powe et al’s (2013) findings, though, have been disputed. Using different measurement tools from Powe et al (2013), Henderson et al (2015) conclude that “Counter to prior observations by immunoassay, VDBG concentrations did not vary by race.” While Bouillon (2014) writes: In our view, black Americans, as compared with white Americans, have lower levels of not only total 25-hydroxyvitamin D but also free or bioavailable 25-hydroxyvitamin D.” And finally, Hollis and Bikle (2014) write: “Specifically, for any given physically measured level of bio-available 25-hydroxyvitamin D, the authors are overestimating bio-available 25-hydroxyvitamin D by 2 to 2.5 times owing to underestimation of vitamin D–binding protein in blacks.”
Either way, even if what Powe et al (2013) conclude is true, that would not mean that black Americans should not supplement with vitamin D, since many diseases and health problems are associated with low vitamin D intake in blacks, including osteoporosis, cardiovascular disease, cancer, diabetes, and other serious conditions (Harris, 2006). An indirect relationship between low levels of vitamin D and hypertension is also noted (Mehta and Agarwal, 2017). Since there is an indirect relationship between vitamin D levels and hypertension, then we should keep an eye on this because black Americans have some of the highest levels of hypertension in the world (Ferdinand and Armani, 2007; see also Fuchs, 2011).
Vitamin D is, of course, important for skeletal and nonskeletal health (Kennel et al, 2010). So if vitamin D is important for skeletal and nonskeletal health, we should see more diseases in black Americans that imply a lack of this steroid in the body. Although blacks have stronger bones even when deficient in vitamin D, it is still observed that black children who break their forearms have less vitamin D circulating in their blood (Ryan et al, 2011). This observation is borne out by the data, since black children are more likely to be deficient in vitamin D compared to other ethnies (Moore, Murphy, and Hollick, 2005). Since black skin predicts vitamin D deficiency (Thomas and Demay, 2000), it seems logical to give vitamin D supplements to children, especially black children, on the basis that it would help lower incidences of bone fractures, even though blacks have stronger bones than whites.
Furthermore, physiologically “normal” levels of vitamin D differ in blacks compared to whites (Wright et al, 2012). They showed that it is indeed a strong possibility that both whites and blacks have different levels of optimum vitamin D. Wright et al (2012) showed that there is a relationship between 25(OH)D levels and intact parathyroid hormone (iPth); for blacks, the threshold in which there was no change was 20 ng/ml whereas for whites it was 30 ng/ml which suggests that there are different levels of optimal vitamin D for each race, and the cause is due to skin color. Thus, physiologically “normal” levels of vitamin D differ for blacks and whites.
There is also a high prevalence of vitamin D deficiency/insufficiency and asthma in black inner-city youth in Washington DC (Freishtat et al, 2010). We can clearly see that, even though black Americans have stronger bones than white Americans and vitamin D predicts bone strength, the fact that blacks have stronger bones than whites even while being deficient in vitamin D on average does not mean that black Americans should not supplement with vitamin D, since it would ameliorate many other problems they have that are related to vitamin D deficiency.
There are also racial differences in prostate cancer (PCa) acquisition too, and vitamin D deficiency may also explain this disparity (Khan and Partin, 2004; Bhardwaj et al, 2017). I have heavily criticized the explanations that testosterone influences PCa, while having indicated that environmental factors such as diet and vitamin D deficiency may explain a large amount of the gap (Batai et al, 2017; but see Stranaland et al, 2017 for a contrary view). Since low vitamin D is related to prostate cancer, by supplementing with vitamin D, it is possible that levels of PCa may decrease. Kristal et al (2014) show that both high and low levels of vitamin D are associated with PCa.
Evidence also exists that vitamin D levels and hypertension are related. Rostand (2010) proposes a unified hypothesis: an important role exists in vitamin D deficiency and the pathogenesis and maintenance of hypertension in blacks (Rostand, 2010).
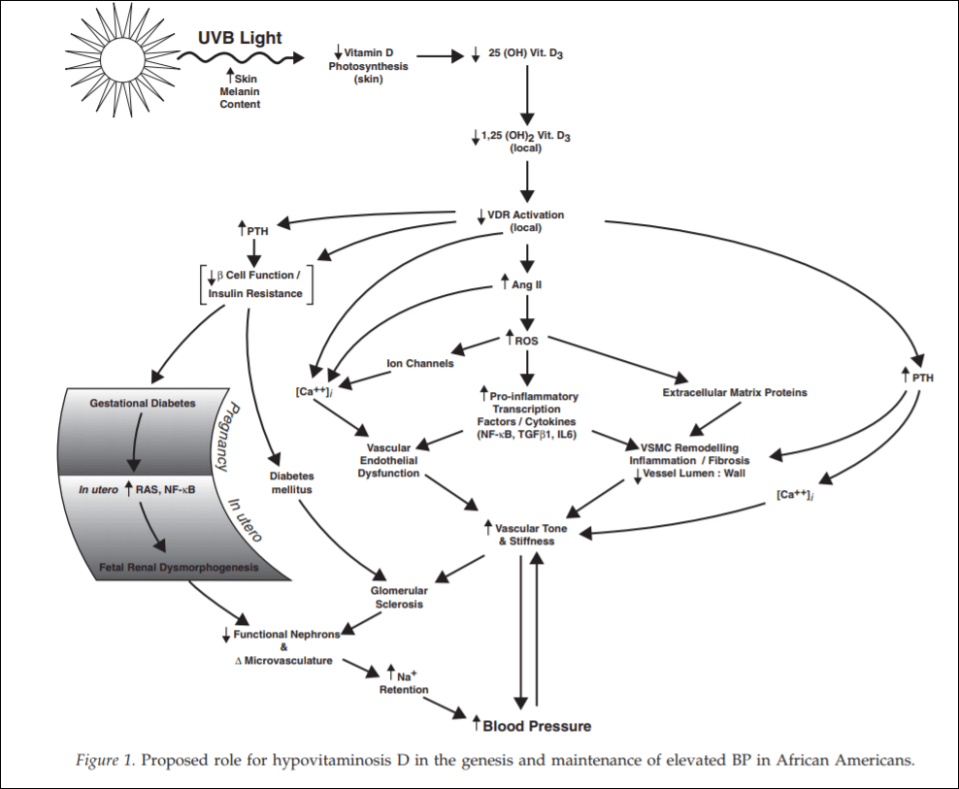
(From Rostand, 2010)
Since black Americans are no longer near the equator, their ability to synthesize vitamin D from UVB rays is diminished. This then probably leads the RAS (renin-angiotensin system) and inflammatory cytokine activation which then leads to vascular endothelial dysfunction along with structural changes to the microvasculature, which have been linked to vascular (arterial) stiffness along with increased vascular resistance, and these changes are shown to precede hypertension, which also occurs early in life. So since blacks are deficient in vitamin D, which even starts in the womb (Bodnar et al, 2007; Dawodu and Wagner, 2007; Lee et al, 2007; Khalessi et al, 2015; Seto et al, 2016), and this vitamin D deficiency most likely produces changes in large and small arteries and arterials, this could be the explanation for higher hypertension in black Americans (Rostand, 2010: 1701).
This would be a large environmental mismatch: since the population is displaced from its ancestral homeland, then this causes problems since it is not the environment where their ancestors evolved. So in this case, since black Americans are concentrated in the southeast corner of the United States, this may explain the high rates of vitamin D deficiency and hypertension in the black American community.
People whose ancestors evolved in locations with fewer UVB rays have lighter skin, whereas people whose ancestors evolved in locations with more UVB rays have darker skin. Thus, by placing populations in their opposite evolutionary environment, we can see how and why deleterious effects would occur in the population that is in the mismatched environment. For whites, skin cancer would occur, whereas for blacks, higher rates of hypertension and low birth weights occur.
Looking at levels of vitamin D deficiency in races is a great way to understand the evolution of certain populations. Because if the vitamin D hypothesis is correct, if skin color is an adaptation to UVB rays, with light skin being an adaptation to low UVB while dark skin is an adaptation to high UVB, then we can safely hypothesize about certain problems that would arise in races that are outside of their natural habitats. We have confirmed these hypotheses—black Americans who are outside of the location that their ancestors evolved in are more likely to have deleterious symptoms, and the symptoms are due to differences in vitamin D production, which come down to differences in skin color and how the skin synthesizes vitamin D in low-light environments.
Even though blacks have stronger bones than whites, this does not mean that they do not experience fractures at a high rate—especially children—and since the association was noticed, then by supplementing with vitamin D, this may lower the disparity of these types of injuries.
Since black Americans, compared to their evolutionary history, live in low-light environments, this then explains the how and why of vitamin D deficiency and why blacks need to supplement with vitamin D; no matter if certain studies show that blacks are ‘healthy’ even though they have low levels of vitamin D. If true (which I strongly doubt), that does not mean that black Americans should not supplement with vitamin D, because numerous other maladies are associated with vitamin D intake. This is one aspect where understanding the evolution of our species and the different races in it would lead to better medical care for individuals and ancestral groups that may need special treatment.
It is clear that race and geography should inform vitamin D intake, for if we do this, many diseases that arise can be ameliorated and quality of life can increase for everyone.
Race, Testosterone, Aggression, and Prostate Cancer
4050 words
Race, aggression, and prostate cancer are all linked, with some believing that race is the cause of higher testosterone which then causes aggression and higher rates of crime along with maladies such as prostate cancer. These claims have long been put to bed, with a wide range of large analyses.
The testosterone debate regarding prostate cancer has been raging for decades and we have made good strides in understanding the etiology of prostate cancer and how it manifests. The same holds true for aggression. But does testosterone hold the key to understanding aggression, prostate cancer and does race dictate group levels of the hormone which then would explain some of the disparities between groups and individuals of certain groups?
Prostate cancer
For decades it was believed that heightened levels of testosterone caused prostate cancer. Most of the theories to this day still hold that large amounts of androgens, like testosterone and it’s metabolic byproduct dihydrotestosterone, are the two many factors that drive the proliferation of cells and therefore, if a male is exposed to higher levels of testosterone throughout their lives then they are at a high risk of prostate cancer compared to a man with low testosterone levels, so the story goes.
In 1986 Ronald Ross set out to test a hypothesis: that black males were exposed to more testosterone in the womb and this then drove their higher rates of prostate cancer later in life. He reportedly discovered that blacks, after controlling for confounds, had 15 percent higher testosterone than whites which may be the cause of differential prostate cancer mortality between the two races (Ross et al, 1986) This is told in a 1997 editorial by Hugh McIntosh. First, the fact that black males were supposedly exposed to more testosterone in the womb is brought up. I am aware of one paper discussing higher levels of testosterone in black women compared to white women (Perry et al, 1996). Though, I’ve shown that black women don’t have high levels of testosterone, not higher than white women, anyway (see Mazur, 2016 for discussion). (Yes I changed my view on black women and testosterone, stop saying that they have high levels of testosterone it’s just not true. I see people still link to that article despite the long disclaimer at the top.)
Alvarado (2013) discusses Ross et al (1986), Ellis and Nyborg (1992) (which I also discussed here along with Ross et al) and other papers discussing the supposed higher testosterone of blacks when compared to whites and attempts to use a life history framework to explain higher incidences of prostate cancer in black males. He first notes that nutritional status influences testosterone production which should be no surprise to anyone. He brings up some points I agree with and some I do not. For instance, he states that differences in nutrition could explain differences in testosterone between Western and non-Western people (I agree), but that this has no effect within Western countries (which is incorrect as I’ll get to later).
He also states that ancestry isn’t related to prostate cancer, writing “In summation, ancestry does not adequately explain variation among ethnic groups with higher or lower testosterone levels, nor does it appear to explain variation among ethnic groups with high or low prostate cancer rates. This calls into question the efficacy of a disease model that is unable to predict either deleterious or protective effects.”
He then states that SES is negatively correlated with prostate cancer rates, and that numerous papers show that people with low SES have higher rates of prostate cancer mortality which makes sense, since people in a lower economic class would have less access to and a chance to get good medical care to identify problems such as prostate cancer, including prostate biopsies and checkups to identify the condition.
He finally discusses the challenge hypothesis and prostate cancer risk. He cites studies by Mazur and Booth (who I’ve cited in the past in numerous articles) as evidence that, as most know, black-majority areas have more crime which would then cause higher levels of testosterone production. He cites Mazur’s old papers showing that low-class men, no matter if they’re white or black, had heightened levels of testosterone and that college-educated men did not, which implies that the social environment can and does elevate testosterone levels and can keep them heightened. Alvarado concludes this section writing: “Among Westernized men who have energetic resources to support the metabolic costs associated with elevated testosterone, there is evidence that being exposed to a higher frequency of aggressive challenges can result in chronically elevated testosterone levels. If living in an aggressive social environment contributes to prostate cancer disparities, this has important implications for prevention and risk stratification.” He’s not really wrong but on what he is wrong I will discuss later on this section. It’s false that testosterone causes prostate cancer so some of this thesis is incorrect.
I rebutted Ross et al (1986) December of last year. The study was hugely flawed and, yet, still gets cited to this day including by Alvarado (2013) as the main point of his thesis. However, perhaps most importantly, the assay times were done ‘when it was convenient’ for the students which were between 10 am and 3 pm. To not get any wacky readings one most assay the individuals as close to 8:30 am as possible. Furthermore, they did not control for waist circumference which is another huge confound. Lastly, the sample was extremely small (50 blacks and 50 whites) and done on a nonrepresentative sample (college students). I don’t think anyone can honestly cite this paper as any evidence for blacks having higher levels of testosterone or testosterone causing prostate cancer because it just doesn’t do that. (Read Race, Testosterone and Prostate Cancer for more information.)
What may explain prostate cancer rates if not for differences in testosterone like has been hypothesized for decades? Well, as I have argued, diet explains a lot of the variation between races. The etiology of prostate cancer is not known (ACA, 2016) but we know that it’s not testosterone and that diet plays a large role in its acquisition. Due to their dark skin, they need more sunlight than do whites to synthesize the same amount of vitamin D, and low levels of vitamin D in blacks are strongly related to prostate cancer (Harris, 2006). Murphy et al (2014) even showed, through biopsies, that black American men had higher rates of prostate cancer if they had lower levels of vitamin D. Lower concentrations of vitamin D in blacks compared to whites due to dark pigmentation which causes reduced vitamin D photoproduction and may also account for “much of the unexplained survival disparity after consideration of such factors as SES, state at diagnosis and treatment” (Grant and Peiris, 2012).
Testosterone
As mentioned above, testosterone is assumed to be higher in certain races compared to others (based on flawed studies) which then supposedly exacerbates prostate cancer. However, as can be seen above, a lot of assumptions go into the testosterone-prostate cancer hypothesis which is just false. So if the assumptions are false about testosterone, mainly regarding racial differences in the hormone and then what the hormone actually does, then most of their claims can be disregarded.
Perhaps the biggest problem is that Ross et al is a 32-year-old paper (which still gets cited favorably despite its huge flaws) while our understanding of the hormone and its physiology has made considerable progress in that time frame. So it’s in fact not so weird to see papers like this that say “Prostate cancer appears to be unrelated related to endogenous testosterone levels” (Boyle et al, 2016). Other papers also show the same thing, that testosterone is not related to prostate cancer (Stattin et al, 2004; Michaud, Billups, and Partin, 2015). This kills a lot of theories and hypotheses, especially regarding racial differences in prostate cancer acquisition and mortality. So, what this shows is that even if blacks did have 15 percent higher serum testosterone than whites as Ross et al, Rushton, Lynn, Templer, et al believed then it wouldn’t cause higher levels of prostate cancer (nor aggression, which I’ll get into later).
How high is testosterone in black males compared to white males? People may attempt to cite papers like the 32-year-old paper by Ross et al, though as I’ve discussed numerous times the paper is highly flawed and should therefore not be cited. Either way, levels are not as high as people believe and meta-analyses and actual nationally representative samples (not convenience college samples) show low to no difference, and even the low difference wouldn’t explain any health disparities.
One of the best papers on this matter of racial differences in testosterone is Richard et al (2014). They meta-analyzed 15 studies and concluded that the “racial differences [range] from 2.5 to 4.9 percent” but “this modest difference is unlikely to explain racial differences in disease risk.” This shows that testosterone isn’t as high in blacks as is popularly misconceived, and that, as I will show below, it wouldn’t even cause higher rates of aggression and therefore criminal behavior. (Rohrmann et al 2007 show no difference in testosterone between black and white males in a nationally representative sample after controlling for lifestyle and anthropometric variables. Whereas Mazur, 2009 shows that blacks have higher levels of testosterone due to low marriage rates and lower levels of adiposity, while be found a .39 ng/ml difference between blacks and whites aged 20 to 60. Is this supposed to explain crime, aggression, and prostate cancer?)
However, as I’ve noted last year (and as Alvarado, 2013 did as well), young black males with low education have higher levels of testosterone which is not noticed in black males of the same age group but with more education (Mazur, 2016). Since blacks of a similar age group have lower levels of testosterone but are more highly educated then this is a clue that education drives aggression/testosterone/violent behavior and not that testosterone drives it.
Mazur (2016) also replicated Assari, Caldwell, and Zimmerman’s (2014) finding that “Our model in the male sample suggests that males with higher levels of education has lower aggressive behaviors. Among males, testosterone was not associated with aggressive behaviors.” I know this is hard for many to swallow that testosterone doesn’t lead to aggressive behavior in men, but I’ll cover that in the last and final section.
So it’s clear that the myth that Rushton, Lynn, Templer, Kanazawa, et al pushed regarding hormonal differences between the races are false. It’s also with noting, as I did in my response to Rushton on r/K selection theory, that the r/K model is literally predicated on 1) testosterone differences between races being real and in the direction that Rushton and Lynn want because they cite the highly flawed Ross et al (1986) and 2) testosterone does not cause higher levels of aggression (which I’ll show below) which then lead to higher rates of crime along with higher rates of incarceration.
A blogger who goes by the name of ethnicmuse did an analysis of numerous testosterone papers and he found:
 Which, of course, goes against a ton of HBD theory, that is, if testosterone did what HBDers believed it does (it doesn’t). This is what it comes down to: blacks don’t have higher levels of testosterone than whites and testosterone doesn’t cause aggression nor prostate cancer so even if this relationship was in the direction that Rushton et al assert then it still wouldn’t cause any of the explanatory variables they discuss.
Which, of course, goes against a ton of HBD theory, that is, if testosterone did what HBDers believed it does (it doesn’t). This is what it comes down to: blacks don’t have higher levels of testosterone than whites and testosterone doesn’t cause aggression nor prostate cancer so even if this relationship was in the direction that Rushton et al assert then it still wouldn’t cause any of the explanatory variables they discuss.
Last year Lee Ellis published a paper outlining his ENA theory (Ellis, 2017). I responded to the paper and pointed out what he got right and wrong. He discussed strength (blacks aren’t stronger than whites due to body type and physiology, but excel in other areas); circulating testosterone, umbilical cord testosterone exposure; bone density and crime; penis size, race, and crime (Rushton’s 1997 claims on penis size don’t ‘size up’ to the literature as I’ve shown two times); prostate-specific antigens, race, and prostate cancer; CAG repeats; intelligence and education and ‘intelligence’; and prenatal androgen exposure. His theory has large holes and doesn’t line up in some places, as he himself admits in his paper. He, as expected, cites Ross et al (1986) favorably in his analysis.
Testosterone can’t explain all of these differences, no matter if it’s prenatal androgen exposure or not, and a difference of 2.5 to 4.9 percent between blacks and whites regarding testosterone (Richard et al, 2014) won’t explain differences in crime, aggression, nor prostate cancer.
Other authors have attempted to also implicate testosterone as a major player in a wide range of evolutionary theories (Lynn, 1990; Rushton, 1997; Rushton, 1999; Hart, 2007; Rushton and Templer, 2012; Ellis, 2017). However, as can be seen by digging into this literature, these claims are not true and therefore we can discard the conclusions come to by the aforementioned authors since they’re based on false premises (testosterone being a cause for aggression, crime, and prostate cancer and r/K meaning anything to human races, it doesn’t)
Finally, to conclude this section, does testosterone explain racial differences in crime? No, racial differences in testosterone, however small, cannot be responsible for the crime gap between blacks and whites.
Testosterone and aggression
Testosterone and aggression, are they linked? Can testosterone tell us anything about individual differences in aggressive behavior? Surprisingly for most, the answer seems to be a resounding no. One example is the castration of males. Does it completely take away the urge to act aggressively? No, it does not. What is shown when sex offenders are castrated is that their levels of aggression decrease, but importantly, they do not decrease to 0. Robert Sapolsky writes on page 96 of his book Behave: The Biology of Humans at Our Best and Worst (2017) (pg 96):
… the more experience a male has being aggressive prior to castration, the more aggression continues afterward. In other words, the less his being aggressive in the future requires testosterone and the more it’s a function of social learning.
He also writes (pg 96-97):
On to the next issue that lessens the primacy of testosterone: What do individual levels of testosterone have to do with aggression? If one person higher testosterone levels than another, or higher levels this week than last, are they more likely to be aggressive?
Initially the answer seemed to be yes, as studies showed correlation between individual differences in testosterone levels and levels of aggression. In a typical study, higher testosterone levels would be observed in those male prisoners with higher rates of aggression. But being aggressive stimulates testosterone secretion; no wonder more aggressive individuals had higher levels. Such studies couldn’t disentangle chickens and eggs.
Thus, a better question is whether differences in testosterone levels among individuals predict who will be aggressive. And among birds, fish, mammals, and especially other primates, the answer is generally no. This has been studied extensively in humans, examining a variety of measures of aggression. And the answer is clear. To quote British endocrinologist John Archer in a definitive 2006 review, “There is a weak and inconsistent association between testosterone levels and aggression in [human] adults, and . . . administration of testosterone to volunteers typically does not increase aggression.” The brain doesn’t pay attention to testosterone levels within the normal range.
[…]
Thus, aggression is typically more about social learning than about testosterone, differing levels of testosterone generally can’t explain why some individuals are more aggressive than others.
Sapolsky also has a 1997 book of essays on human biology titled The Trouble With Testosterone: And Other Essays On The Biology Of The Human Predicament and he has a really good essay on testosterone titled Will Boys Just Be Boys? where he writes (pg 113 to 114):
Okay, suppose you note a correlation between levels of aggression and levels of testosterone among these normal males. This could be because (a) testosterone elevates aggression; (b) aggression elevates testosterone secretion; (c) neither causes the other. There’s a huge bias to assume option a while b is the answer. Study after study has shown that when you examine testosterone when males are first placed together in the social group, testosterone levels predict nothing about who is going to be aggressive. The subsequent behavioral differences drive the hormonal changes, not the other way around.
Because of a strong bias among certain scientists, it has taken do forever to convince them of this point.
[…]
As I said, it takes a lot of work to cure people of that physics envy, and to see interindividual differences in testosterone levels don’t predict subsequent differences in aggressive behavior among individuals. Similarly, fluctuations in testosterone within one individual over time do not predict subsequent changes in the levels of aggression in the one individual—get a hiccup in testosterone secretion one afternoon and that’s not when the guy goes postal.
And on page 115 writes:
You need some testosterone around for normal levels of aggressive behavior—zero levels after castration and down it usually goes; quadruple it (the sort of range generated in weight lifters abusing anabolic steroids), and aggression typically increases. But anywhere from roughly 20 percent of normal to twice normal and it’s all the same; the brain can’t distinguish among this wide range of basically normal values.
Weird…almost as if there is a wide range of ‘normal’ that is ‘built in’ to our homeodynamic physiology…
So here’s the point: differences in testosterone between individuals tell us nothing about individual differences in aggressive behavior; castration and replacement seems to show that, however broadly, testosterone is related to aggression “But that turns out to not be true either, and the implications of this are lost on most people the first thirty times you tell them about it. Which is why you’d better tell them about it thirty-one times, because it’s the most important part of this piece” (Sapolsky, 1997: 115).
Later in the essay, Sapolsky discusses a discusses 5 monkeys that were given time to form a hierarchy of 1 through 5. Number 3 can ‘throw his weight’ around with 4 and 5 but treads carefully around 1 and 2. He then states to take the third-ranking monkey and inject him with a ton of testosterone, and that when you check the behavioral data that he’d then be participating in more aggressive actions than before which would imply that the exogenous testosterone causes participation in more aggressive behavior. But it’s way more nuanced than that.
So even though small fluctuations in the levels of the hormone don’t seem to matter much, testosterone still causes aggression. But that would be wrong. Check out number 3 more closely. Is he now raining aggression and terror on any and all in the group, frothing in an androgenic glaze of indiscriminate violence. Not at all. He’s still judiciously kowtowing to numbers 1 and 2 but has simply become a total bastard to number 4 and 5. This is critical: testosterone isn’t causing aggression, it’s exaggerating the aggression that’s already there.
The correlation between testosterone and aggression is between .08 and .14 (Book, Starzyk, and Quinsey, 2001; Archer, Graham-Kevan, and Davies, 2005; Book and Quinsey, 2005). Therefore, along with all of the other evidence provided in this article, it seems that testosterone and aggression have a weak positive correlation, which buttresses the point that aggression concurrent increases in testosterone.
Sapolsky then goes on to discuss the amygdala’s role in fear processing. The amygdala has its influence on aggressive behavior through the stria terminalis, which is a bunch of neuronal connections. How the amygdala influences aggression is simple: bursts of electrical excitation called action potentials go up and down the stria terminalis which changes the hypothalamus. You can then inject testosterone right into the brain and will it cause the same action potentials that surge down the stria terminalis? No, it does not turn on the pathway at all. This only occurs only if the amygdala is already sending aggression-provoking action potentials down the stria terminalis with testosterone increasing the rate of action potentials you’re shortening the rest time between them. So it doesn’t turn on this pathway, it exaggerates the preexisting pattern, which is to say, it’s exaggerating the response to environmental triggers of what caused the amygdala to get excited in the first place.
He ends this essay writing (pg 119):
Testosterone is never going to tell us much about the suburban teenager who, in his after-school chess club, has developed a particularly aggressive style with his bishops. And it certainly isn’t going to tell us much about the teenager in some inner-city hellhole who has taken to mugging people. “Testosterone equals aggression” is inadequate for those who would offer a simple solution to the violent male—just decrease levels of those pesky steroids. And “testosterone equals aggression” is certainly inadequate for those who would offer a simple excuse: Boys will be boys and certain things in nature are inevitable. Violence is more complex than a single hormone. This is endocrinology for the bleeding heart liberal—our behavioral biology is usually meaningless outside of the context of social factors and the environment in which it occurs.
Injecting individuals with supraphysiological doses of testosterone as high as 200 and 600 mg per week does not cause heightened anger or aggression (Tricker et al, 1996; O’Connor et, 2002). This, too, is a large blow for the testosterone-induces-aggression hypothesis. Because aggressive behavior heightens testosterone, testosterone doesn’t heighten aggressive behavior. (This is the causality that has been looked for, and here it is. The causality is not in the other direction.) This tells us that we need to be put into situations for our aggression to rise and along with it, testosterone. I don’t even see how people could think that testosterone could cause aggression. It’s obvious that the environmental trigger needs to be there first in order for the body’s physiology to begin testosterone production in order to prepare for the stimulus that caused the heightened testosterone production. Once the trigger occurs, then it can and does stay heightened, especially in areas where dominance contests would be more likely to occur, which would be low-income areas (Mazur, 2006, 2016).
(Also read my response to Batrinos, 2012, my musings on testosterone and race, and my responses to Robert Lindsay and Sean Last.)
Lastly, one thing that gets on my nerves that people point to to attempt to show that testosterone and its derivatives cause violence, aggression etc is the myth of “roid rage” which is when an individual objects himself with testosterone, anabolic steroids or another banned substance, and then the individual becomes more aggressive as a result of more free-flowing testosterone in their bloodstream.
The problem here is that people believe what they hear on the media about steroids and testosterone, and they’re largely not true. One large analysis was done to see the effects of steroids and other illicit drug use on behavior, and what was found was that after controlling for other substance use “Our results suggest that it was not lifetime steroid use per se, but rather co-occurrring polysubstance abuse that most parsimoniously explains the relatively strong association of steroid use and interpersonal violence” (Lundholm et al, 2015). So after controlling for other drugs used, men who use steroids do not go to prison and be convicted of violence after other polysubstance use was controlled for, implying that is what’s driving interpersonal violence, not the substance abuse of steroids.
Conclusion
Numerous myths about testosterone have been propagated over the decades, which are still believed in the new millennium despite numerous other studies and arguments to the contrary. As can be seen, the myths that people believe about testosterone are easily debunked. Numerous papers (with better methodology than Ross et al) attest to the fact that testosterone levels aren’t as high as was believed decades ago between the races. Diet can explain a lot of the variation, especially vitamin D intake. Injecting men with supraphysiological doses of testosterone does not heighten anger nor aggression. It does not even heighten prostate cancer severity.
Racial differences in testosterone are also not as high as people would like to believe, there is even an opposite relationship with Asians having higher levels and whites having lower (which wouldn’t, on average, imply femininity) testosterone levels. So as can be seen, the attempted r/K explanations from Rushton et al don’t work out here. They’re just outright wrong on testosterone, as I’ve been arguing for a long while on this blog.
Testosterone doesn’t cause aggression, aggression causes heightened testosterone. It can be seen from studies of men who have been castrated that the more crime they committed before castration, the more crime they will commit after which implies a large effect of social learning on violent behavior. Either way, the alarmist attitudes of people regarding testosterone, as I have argued, are not needed because they’re largely myths.
Responses to The Alternative Hypothesis and Robert Lindsay on Testosterone
2300 words
I enjoy reading what other bloggers write about testosterone and its supposed link to crime, aggression, and prostate cancer; I used to believe some of the things they did, since I didn’t have a good understanding of the hormone nor its production in the body. However, once you understand how its produced in the body, then what others say about it will seem like bullshit—because it is. I’ve recently read a few articles on testosterone from the HBD-blog-o-sphere and, of course, they have a lot of misconceptions in them—some even using studies I have used myself on this blog to prove my point that testosterone does not cause crime!! Now, I know that most people don’t read studies that are linked, so they would take what it says on face value because, why not, there’s a cite so what he’s saying must be true, right? Wrong. I will begin with reviewing an article by someone at The Alternative Hypothesis and then review one article from Robert Lindsay on testosterone.
The Alternative Hypothesis
Faulk has great stuff here, but the one who wrote this article, Testosterone, Race, and Crime, 1) doesn’t know what he’s talking about and 2) clearly didn’t read the papers he cited. Read this article, you’ll see him make bold claims using studies I have used for my own arguments that testosterone doesn’t cause crime! Let’s take a look.
One factor which explains part of why Blacks have higher than average crime rates is testosterone. Testosterone is known to cause aggression, and Blacks are known to at once have more of it and, for genetic reasons, to be more sensitive to its effects.
- No it doesn’t.
- “Testosterone is known to cause aggression“, but that’s the thing: it’s only known that it ’causes’ aggression, it really doesn’t.
- Evidence is mixed on blacks being “… for genetic reasons … more sensitive to its effects” (Update on Androgen Receptor gene—Race/History/Evolution Notes).
Testosterone activity has been linked many times to aggression and crime. Meta-analyses show that testosterone is correlated with aggression among humans and non human animals (Book, Starzyk, and Quinsey, 2001).
Why doesn’t he say what the correlation is? It’s .14 and this study, while Archer, Graham-Kevan and Davies, (2005) reanalyzed the studies used in the previous analysis and found the correlation to be .08. This is a dishonest statement.
Women who suffer from a disease known as congenital adrenal hyperplasia are exposed to abnormally high amounts of testosterone and are abnormally aggressive.
Abnormal levels of androgens in the womb for girls with CAH are associated with aggression, while boys with and without CAH are similar in aggression/activity level (Pasterski et al, 2008), yet black women, for instance, don’t have higher levels of testosterone than white women (Mazur, 2016). CAH is just girls showing masculinized behavior; testosterone doesn’t cause the aggression (See Archer, Graham-Kevan and Davies, 2005)
Artificially increasing the amount of testosterone in a person’s blood has been shown to lead to increases in their level of aggression (Burnham 2007; Kouri et al. 1995).
Actually, no. Supraphysiological levels of testosterone administered to men (200 and 600 mg weekly) did not increase aggression or anger (Batrinos, 2012).
Finally, people in prison have higher than average rates of testosterone (Dabbs et al., 2005).
Dabbs et al don’t untangle correlation from causation. Environmental factors can explain higher testosterone levels (Mazur, 2016) in inmates, and even then, some studies show socially dominant and aggressive men have the same levels of testosterone (Ehrenkraz, Bliss, and Sheard, 1974).
Thus, testosterone seems to cause both aggression and crime.
No, it doesn’t.
Why Testosterone Does Not Cause Crime
Testosterone and Aggressive Behavior
Furthermore, of the studies I could find on testosterone in Africans, they have lower levels than Western men (Campbell, O’Rourke, and Lipson, 2003; Lucas and Campbell, and Ellison, 2004; Campbell, Gray, and Ellison, 2006) so, along with the studies and articles cited on testosterone, aggression, and crime, that’s another huge blow to the testosterone/crime/aggression hypothesis.
Richard et al. (2014) meta-analyzed data from 14 separate studies and found that Blacks have higher levels of free floating testosterone in their blood than Whites do.
They showed that blacks had 2.5 to 4.9 percent higher testosterone than whites, which could not explain the higher prostate cancer incidence (which meta-analyses call in to question; Sridhar et al 2010; Zagars et al 1998). That moderate amount would not be enough to cause differences in aggression either.
Exacerbating this problem even further is the fact that Blacks are more likely than Whites to have low repeat versions of the androgen receptor gene. The androgen reception (AR) gene codes for a receptor by the same name which reacts to androgenic hormones such as testosterone. This receptor is a key part of the mechanism by which testosterone has its effects throughout the body and brain.
The rest of the article talks about CAG repeats and aggressive/criminal behavior, but it seems that whites have fewer CAG repeats than blacks.
Robert Lindsay
This one is much more basic, and tiring to rebut but I’ll do it anyway. Lindsay has a whole slew of articles on testosterone on his blog that show he doesn’t understand the hormone, but I’ll just talk about this one for now: Black Males and Testosterone: Evolution and Perspectives.
It was also confirmed by a recent British study (prostate cancer rates are somewhat lower in Black British men because a higher proportion of them have one White parent)
Jones and Chinegwundoh (2014) write: “Caution should be taken prior to the interpretation of these results due to a paucity of research in this area, limited accurate ethnicity data, and lack of age-specific standardisation for comparison. Cultural attitudes towards prostate cancer and health care in general may have a significant impact on these figures, combined with other clinico-pathological associations.”
This finding suggests that the factor(s) responsible for the difference in rates occurs, or first occurs, early in life. Black males are exposed to higher testosterone levels from the very start.
In a study of women in early pregnancy, Ross found that testosterone levels were 50% higher in Black women than in White women (MacIntosh 1997).
I used to believe this, but it’s much more nuanced than that. Black women don’t have higher levels of testosterone than white women (Mazur, 2016; and even then Lindsay fails to point out that this was pregnant women).
According to Ross, his findings are “very consistent with the role of androgens in prostate carcinogenesis and in explaining the racial/ethnic variations in risk” (MacIntosh 1997).
Testosterone has been hypothesized to play a role in the etiology of prostate cancer, because testosterone and its metabolite, dihydrotestosterone, are the principal trophic hormones that regulate growth and function of epithelial prostate tissue.
Testosterone doesn’t cause prostate cancer (Stattin et al, 2003; Michaud, Billups, and Partin, 2015). Diet explains any risk that may be there (Hayes et al, 1999; Gupta et al, 2009; Kheirandish and Chinegwundoh, 2011; Williams et al, 2012; Gathirua-Mingwai and Zhang, 2014). However in a small population-based study on blacks and whites from South Carolina, Sanderson et al (2017) “did not find marked differences in lifestyle factors associated with prostate cancer by race.”
Regular exercise, however, can decrease PCa incidence in black men (Moore et al, 2010). A lot of differences can be—albeit, not too largely— ameliorated by environmental interventions such as dieting and exercising.
Many studies have shown that young Black men have higher testosterone than young White men (Ellis & Nyborg 1992; Ross et al. 1992; Tsai et al. 2006).
Ellis and Nyborg (1992) found 3 percent difference. Ross et al (1992) have the same problem as Ross et al (1986), which used University students (~50) for their sample. They’re not representative of the population. Ross et al (1992) also write:
Samples were also collected between 1000 h and 1500 h to avoid confounding
by any diurnal variation in testosterone concentrations.
Testosterone levels should be measured near to 8 am. This has the same time variation too, so I don’t take this study seriously due to that confound. Assays were collected “between” the hours of 10 am and 3 pm, which means it was whenever convenient for the student. No controls on activities, nor attempting to assay at 8 am. People of any racial group could have gone at whatever time in that 5 hour time period and skew the results. Assaying “between” those times completely defeats the purpose of the study.
This advantage [the so-called testosterone advantage] then shrinks and eventually disappears at some point during the 30s (Gapstur et al., 2002).
Gapstur et al (2002) help my argument, not yours.
This makes it very difficult if not impossible to explain differing behavioral variables, including higher rates of crime and aggression, in Black males over the age of 33 on the basis of elevated testosterone levels.
See above where I talk about crime/testosterone/aggression.
Critics say that more recent studies done since the early 2000’s have shown no differences between Black and White testosterone levels. Perhaps they are referring to recent studies that show lower testosterone levels in adult Blacks than in adult Whites. This was the conclusion of one recent study (Alvergne et al. 2009) which found lower T levels in Senegalese men than in Western men. But these Senegalese men were 38.3 years old on average.
Alvergne, Fauri, and Raymond (2009) show that the differences are due to environmental factors:
This study investigated the relationship between mens’ salivary T and the trade-off between mating and parenting efforts in a polygynous population of agriculturists from rural Senegal. The men’s reproductive trade-offs were evaluated by recording (1) their pair-bonding/fatherhood status and (2) their behavioral profile in the allocation of parental care and their marital status (i.e. monogamously married; polygynously married).
They also controlled for age, so his statement “But these Senegalese men were 38.3 years old on average” is useless.
These critics may also be referring to various studies by Sabine Rohrmann which show no significance difference in T levels between Black and White Americans. Age is poorly controlled for in her studies.
That is one study out of many that I reference. Rohrmann et al (2007) controlled for age. I like how he literally only says “age is poorly controlled for in her studies“, because she did control for age.
That study found that more than 25% of the samples for adults between 30 and 39 years were positive for HSV-2. It is likely that those positive samples had been set aside, thus depleting the serum bank of male donors who were not only more polygamous but also more likely to have high T levels. This sample bias was probably worse for African American participants than for Euro-American participants.
Why would they use diseased samples? Do you even think?
Young Black males have higher levels of active testosterone than European and Asian males. Asian levels are about the same as Whites, but a study in Japan with young Japanese men suggested that the Japanese had lower activity of 5-alpha reductase than did U.S. Whites and Blacks (Ross et al 1992). This enzyme metabolizes testosterone into dihydrotestosterone, or DHT, which is at least eight to 10 times more potent than testosterone. So effectively, Asians have the lower testosterone levels than Blacks and Whites. In addition, androgen receptor sensitivity is highest in Black men, intermediate in Whites and lowest in Asians.
Wu et al (1995) show that Asians have the highest testosterone levels. Evidence is also mixed here as well. See above on AR sensitivity.
Ethnicmuse also showed that, contrary to popular belief, Asians have higher levels of testosterone than Africans who have higher levels of testosterone than Caucasians in his meta-analysis. (Here is his data.)
The Androgen Receptor and “masculinization”
Let us look at one study (Ross et al 1986) to see what the findings of a typical study looking for testosterone differences between races shows us. This study gives the results of assays of circulating steroid hormone levels in white and black college students in Los Angeles, CA. Mean testosterone levels in Blacks were 19% higher than in Whites, and free testosterone levels were 21% higher. Both these differences were statistically significant.
Assay times between 10 am and 3 pm, unrepresentative sample of college men, didn’t have control for waist circumference. Horribly study.
A 15% difference in circulating testosterone levels could readily explain a twofold difference in prostate cancer risk.
No, it wouldn’t (if it were true).
Higher testosterone levels are linked to violent behavior.
Causation not untangled.
Studies suggest that high testosterone lowers IQ (Ostatnikova et al 2007). Other findings suggest that increased androgen receptor sensitivity and higher sperm counts (markers for increased testosterone) are negatively correlated with intelligence when measured by speed of neuronal transmission and hence general intelligence (g) in a trade-off fashion (Manning 2007).
Who cares about correlations? Causes matter more. High testosterone doesn’t lower IQ. Racial differences in testosterone are tiring to talk about now, but there are still a few more articles I need to rebut.
Conclusion
Racial differences in testosterone don’t exist/are extremely small in magnitude (as I’ve covered countless times). The one article from TAH literally misrepresents studies/leaves out important figures in the testosterone differences between the two races to push a certain agenda. Though if you read the studies you see something completely different. It’s the same with Lindsay. He misunderstood a few studies to push his agenda about testosterone and crime and prostate cancer. They’re both wrong, though.
Why Testosterone Does Not Cause Crime
Testosterone and Aggressive Behavior
Race, Testosterone, and Prostate Cancer
Population variation in endocrine function—Race/History/Evolution Notes
Racial differences in testosterone are tiring to talk about now, but there are still a few more articles I need to rebut. People read and write about things they don’t understand, which is the cause of these misconceptions with the hormone, as well as, of course, misinterpreting studies. Learn about the hormone and you won’t fear it. It doesn’t cause crime, prostate cancer nor aggression; these people who write these articles have one idea in their head and they just go for it. They don’t understand the intricacies of the endocrine system and how sensitive it is to environmental influence. I will cover more articles that others have written on testosterone and aggression to point out what they got wrong.
Race, Testosterone, and Honor Culture
2300 words
Misinformation about testosterone and strength in regards to race is rampant in the HBD-o-sphere. One of the most oft-repeated phrases is that “Blacks have higher levels of testosterone than whites”, even after controlling for numerous confounds. However, the people who believe this literally only cite one singular study with 50 blacks and 50 whites. Looking at more robust data with higher ns shows a completely different story. Tonight I will, again, go through the race/testosterone conundrum (again).
Type I fibers fire first when heavy lifting. Whites have more type I fibers. Powerlifters and Olympic lifters have a greater amount type IIa fibers, with fewer type IIx fibers (like whites). This explains why blacks are hardly represented in powerlifting and strongman competitions.
Somatype, too, also plays a role. Whites are more endo than blacks who are more meso. Endomorphic individuals are stronger, on average, than mesomorphic and ectomorphic individuals.
Blacks have narrower hips and pelves. This morphological trait further explains why blacks dominate sports. Some people may attempt to pick out one variable that I speak about (fiber type, morphology, somatype, fat mass, etc) and attempt to disprove it, thinking that disproving that variable will discredit my whole argument. However, fiber typing is set by the second trimester, with no change in fiber type from age 6 to adulthood (Bell et al, 1980).
It is commonly believed that blacks have higher levels of testosterone than whites. However, this claim is literally based off of one study (Ross et al, 1986) when other studies have shown low to no difference in T levels (Richards et al, 1992; Gapstur et al, 2002; Rohrmann et al, 2007; Mazur, 2009; Lopez et al, 2013; Richard et al 2014). People who still push the “blacks-have-higher-T-card” in the face of this evidence are, clearly, ideologues who want to cushion their beliefs when presented with contradictory evidence (Nyhan and Reifler, 2010).
‘Honor Culture’ and testosterone
In all of my articles on this subject, I have stated—extensively—that testosterone is mediated by the environment. That is, certain social situations can increase testosterone. This is a viewpoint that I’ve emphatically stated. I came across a paper while back that talks about a sociological perspective (I have huge problems with social ‘science’, [more on that soon] but this study was very well done) in regards to the testosterone difference between blacks and whites.
Some people when they read this, however, may go immediately to the part of the paper that says what they want it to say without fully assessing the paper. In this section, I will explain the paper and how it confirms my assertions/arguments.
Mazur (2016) begins the paper talking about ‘honor culture‘, which is a culture where people avoid intentionally offending others while also maintaining a status for not backing down from a confrontation. This theory was proposed by Richard Nisbett in 1993 to explain why the South had higher rates of violence—particularly the Scotch-Irish.
However parsimonious the theory may sound, despite its outstanding explanatory power, it doesn’t hold while analyzing white male homicides in the South. It also doesn’t hold analyzing within-county homicide rates either, since apparently poverty better explains higher homicide rates.
But let’s assume it’s true for blacks. Let’s assume the contention to be true that there is an ‘honor culture’ that people take part in.
Young black men with no education had higher levels of testosterone than educated whites and blacks. Looking at this at face value—literally going right to the section of the paper that says that poor blacks had higher testosterone, nearly 100 ng/ml higher than the mean testosterone of whites. As Mazur (2016) notes, this contradicts his earlier 2009 study in which he found no difference in testosterone between the races.
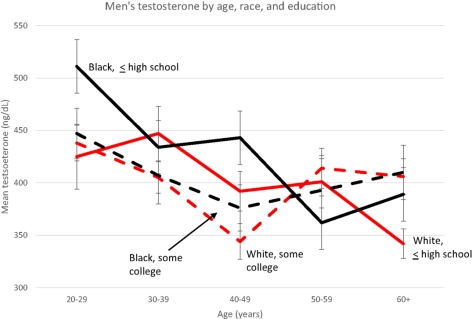
Note the low testosterone for both races at age 20-29—ranging from about 515 to 425—why such low testosterone levels for young men? Anyway, the cause for the higher levels is due to the type of honor culture that blacks participate in, according to Mazur (which is consistent with the data showing that testosterone rises during conflict/aggressive situations).
Mazur cites Elijah Anderson, saying that most youths have a “code of the streets” they take part in, which have to do with interpersonal communication such as “gait and verbal expressions” to deter aggressive behavior.
Testosterone is not a causal variable in regards to violent behavior. But it does rise during conflicts with others, watching a favorite sports team, asserting dominance, and even how you carry yourself (especially your posture). Since low-class blacks participate in these types of behaviors, then they would have higher levels of testosterone due to needing to “keep their status.”
When testosterone rises in these situations, it increases the response threat in mens’ brains, most notably showing increased activity in the amygdala. Further, dominant behavior and posture also increase testosterone levels. Putting this all together, since blacks with only a high school education have higher testosterone levels and are more likely to participate in honor culture compared to whites and blacks with higher educational achievement, then they would have higher testosterone levels than whites and blacks with a high school education who do not participate in honor culture.
Further, as contrary to what I have written in the past (and have since rescinded), there is no indication of higher testosterone levels in black women with low education. It seems this ‘honor culture’ effect on testosterone only holds for black men with only a high school education.
Mazur’s (2016) most significant finding was that black men aged 20-29 with only a high school education had 91 ng/ml higher testosterone than whites. Among older and/or educated men, testosterone did not vary. This indicates that since they have attained higher levels of educational success, there is no need to participate in ‘honor culture’.
This is yet further evidence for my assertion that environmental variables such as posture, dominance, and aggressive behavior raise testosterone levels.
The honor culture hypothesis is found to hold in Brazil in a comparative study of 160 inmates and non-inmates (De Souza et al, 2016). As Mazur (2016) notes, the honor culture hypothesis could explain the high murder rate for black Americans—the need to ‘keep their status’. It’s important to note that this increase in testosterone was not noticed in teenage or female blacks (because they don’t participate in honor culture).
There is a perfectly good environmental—not genetic—reason for this increase in testosterone in young blacks with only a high school education. Now that we know this, back to race and strength.
Mazur (2009) found that black men in the age range of 20-69, they averaged .39 ng/ml higher testosterone than whites, which is partly explained by lower marriage rates and low adiposity. White men are more likely to be obese than black men, since black men with more African ancestry are less likely to be obese. When controlling for BMI, blacks are found to have 2.5-4.9 percent more testosterone than whites (Gapstur et al, 2002, Rohrmann et al, 2007, Richard et al, 2014). There is little evidence for the assertion that blacks have higher levels of testosterone without environmental triggers.
Blacks between the age of 12 and 15 average lower levels of testosterone than whites. However, after the age of 15, “testosterone levels increase rapidly” with blacks having higher peak levels than whites (seen in table 2 below). After adjusting for the usual confounds (BMI, smoking, age, physical activity, and waist circumference), blacks still had higher levels of testosterone—which is attributed to higher levels of lean mass.
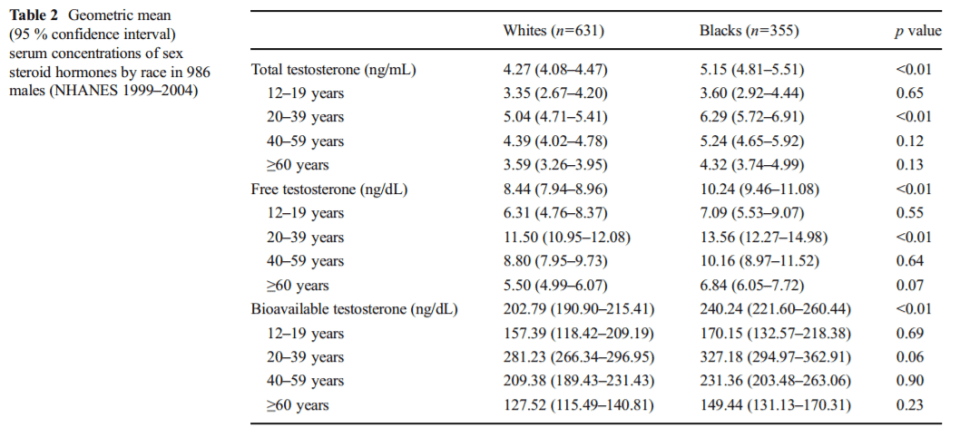
As seen above in table 2 from Hu et al (2014), the difference in total testosterone between blacks and whites aged 20-39 was 6.29 ng/ml and 5.04 ng/ml respectively, with free testosterone for whites being 11.50 and 13.56 for blacks and finally bioavailable testosterone for whites and blacks aged 20-39 was 281.23 and 327.18 ng/ml respectively. These small differences in testosterone cannot account for racial disparities in violence nor prostate cancer—since there is no relationship between prostate cancer and testosterone (Stattin et al, 2003; Michaud, Billups, and Partin, 2015).
In regards to Africans, the best studies I can find comparing some African countries with the West study salivary testosterone. However, there is a direct correlation between salivary testosterone and free serum testosterone (Wang et al, 1981; Johnson, Joplin, and Burrin, 1987). Of the studies I could find, Kenyan pastoralists called the Ariaal have lower levels of testosterone than Western men (Campbell, O’Rourke, and Lipson, 2003; Campbell, Gray, and Ellison, 2006) while men in Zimbabwe had levels “much lower” compared to Western populations (Lukas, Campbell, and Ellison, 2004). Lastly, among men aged 15 to 30, salivary testosterone levels in an American sample was 335 pmol//l compared to 286 pmol/l in men from the Congo (Elisson et al, 2002). Even certain African populations don’t have higher testosterone levels than Western peoples.
Conclusion
The meme that blacks have higher rates of testosterone in comparison to whites needs to be put to rest. This is only seen in blacks who participate in ‘honor culture’, which is an environmental variable. This is in contrast to people who believe that it is genetic in nature—environmental variables can and do drive hormones. Mazur (2016) is proof of that. Mazur (2016) also shows that the honor culture hypothesis doesn’t hold for teens or black males—so they don’t have elevated levels of testosterone. Certain studies of African populations, however, do not show higher levels of testosterone than Western populations.
Looking at the complete literature—rather than a select few studies— we can see that testosterone levels between white and black Americans are not as high as is commonly stated (Richards et al, 1992; Gapstur et al, 2002; Rohrmann et al, 2007; Mazur, 2009; Lopez et al, 2013; Hu et al, 2014; Richard et al, 2014). Further, even if blacks did have higher levels of testosterone than whites—across the board (sans honor culture), it still wouldn’t explain higher rates of black violence when compared to whites, nor would it explain higher prostate cancer rates (Stattin et al, 2003; Michaud, Billups, and Partin, 2015).
Only blacks with low educational achievement have higher levels of testosterone—which, even then is not enough to explain higher rates of violence or prostate cancer acquisition. Other factors explain the higher murder rate (i.e., honor culture, which increases testosterone, the environmental trigger matters first and foremost) and violent crime that blacks commit. But attempting to explain it with 30-year-old studies (Ross et al, 1986) and studies that show that environmental factors increase testosterone (Mazur, 2016) don’t lend credence to that hypothesis.
References
Bell, R. D., Macdougall, J. D., Billeter, R., & Howald, H. (1980). Muscle fiber types and morphometric analysis of skeletal muscle in six-year-old children. Medicine & Science in Sports & Exercise,12(1). doi:10.1249/00005768-198021000-00007
Campbell, B., O’rourke, M. T., & Lipson, S. F. (2003). Salivary testosterone and body composition among Ariaal males. American Journal of Human Biology,15(5), 697-708. doi:10.1002/ajhb.10203
Campbell, B. C., Gray, P. B., & Ellison, P. T. (2006). Age-related patterns of body composition and salivary testosterone among Ariaal men of Northern Kenya. Aging Clinical and Experimental Research,18(6), 470-476. doi:10.1007/bf03324846
De Souza, Souza, B. C., Bilsky, W., & Roazzi, A. (2016). The culture of honor as the best explanation for the high rates of criminal homicide in Pernambuco: A comparative study with 160 convicts and non-convicts. Anuario de Psicología Jurídica,26(1), 114-121. doi:10.1016/j.apj.2015.03.001
Ellison, P. T., Bribiescas, R. G., Bentley, G. R., Campbell, B. C., Lipson, S. F., Panter-Brick, C., & Hill, K. (2002). Population variation in age-related decline in male salivary testosterone. Human Reproduction,17(12), 3251-3253. doi:10.1093/humrep/17.12.3251
, , , , , . Serum androgen concentrations in young men: a longitudinal analysis of associations with age, obesity, and race—the CARDIA male hormone study. Cancer Epidemiol Biomarkers Prev 2002; 11: 1041–7
Hu, H., Odedina, F. T., Reams, R. R., Lissaker, C. T., & Xu, X. (2014). Racial Differences in Age-Related Variations of Testosterone Levels Among US Males: Potential Implications for Prostate Cancer and Personalized Medication. Journal of Racial and Ethnic Health Disparities,2(1), 69-76. doi:10.1007/s40615-014-0049-8
Johnson, S. G., Joplin, G. F., & Burrin, J. M. (1987). Direct assay for testosterone in saliva: Relationship with a direct serum free testosterone assay. Clinica Chimica Acta,163(3), 309-318. doi:10.1016/0009-8981(87)90249-x
Lopez, D. S., Peskoe, S. B., Joshu, C. E., Dobs, A., Feinleib, M., Kanarek, N., . . . Platz, E. A. (2013). Racial/ethnic differences in serum sex steroid hormone concentrations in US adolescent males. Cancer Causes & Control,24(4), 817-826. doi:10.1007/s10552-013-0154-8
Lukas, W. D., Campbell, B. C., & Ellison, P. T. (2004). Testosterone, aging, and body composition in men from Harare, Zimbabwe. American Journal of Human Biology,16(6), 704-712. doi:10.1002/ajhb.20083
Mazur, A. (2009). The age-testosterone relationship in black, white, and Mexican-American men, and reasons for ethnic differences. The Aging Male,12(2-3), 66-76. doi:10.1080/13685530903071802
Mazur, A. (2016). Testosterone Is High among Young Black Men with Little Education. Frontiers in Sociology,1. doi:10.3389/fsoc.2016.00001
Michaud, J. E., Billups, K. L., & Partin, A. W. (2015). Testosterone and prostate cancer: an evidence-based review of pathogenesis and oncologic risk. Therapeutic Advances in Urology,7(6), 378-387. doi:10.1177/1756287215597633
Nyhan, B., & Reifler, J. (2010). When Corrections Fail: The Persistence of Political Misperceptions. Political Behavior,32(2), 303-330. doi:10.1007/s11109-010-9112-2
Richard, A., Rohrmann, S., Zhang, L., Eichholzer, M., Basaria, S., Selvin, E., . . . Platz, E. A. (2014). Racial variation in sex steroid hormone concentration in black and white men: a meta-analysis. Andrology,2(3), 428-435. doi:10.1111/j.2047-2927.2014.00206.x
Richards, R. J., Svec, F., Bao, W., Srinivasan, S. R., & Berenson, G. S. (1992). Steroid hormones during puberty: racial (black-white) differences in androstenedione and estradiol–the Bogalusa Heart Study. The Journal of Clinical Endocrinology & Metabolism,75(2), 624-631. doi:10.1210/jcem.75.2.1639961
Rohrmann, S., Nelson, W. G., Rifai, N., Brown, T. R., Dobs, A., Kanarek, N., . . . Platz, E. A. (2007). Serum Estrogen, But Not Testosterone, Levels Differ between Black and White Men in a Nationally Representative Sample of Americans. The Journal of Clinical Endocrinology & Metabolism,92(7), 2519-2525. doi:10.1210/jc.2007-0028
Ross R, Bernstein L, Judd H, Hanisch R, Pike M, Henderson B. Serum testosterone levels in healthy young black and white men. J Natl Cancer Inst. 1986 Jan;76(1):45–48
Stattin, P., Lumme, S., Tenkanen, L., Alfthan, H., Jellum, E., Hallmans, G., . . . Hakama, M. (2003). High levels of circulating testosterone are not associated with increased prostate cancer risk: A pooled prospective study. International Journal of Cancer,108(3), 418-424. doi:10.1002/ijc.11572
Wang, C., Plymate, S., Nieschlag, E., & Paulsen, C. A. (1981). Salivary Testosterone in Men: Further Evidence of a Direct Correlation with Free Serum Testosterone. The Journal of Clinical Endocrinology & Metabolism,53(5), 1021-1024. doi:10.1210/jcem-53-5-1021
Racial Differences in Prostate Cancer: Part II
1050 words
I showed in part I, that the oft-cited reason for racial differences in prostate cancer acquisition and mortality are not due to higher levels of circulating testosterone when comparing blacks to whites (Richard et al, 2014). I posited (and provided sufficient evidence) that the disparity could come down to differences in vitamin D between the races. Black Americans are far removed from their ancestral environment, living in a cooler area. Their pigmentation reduces vitamin D production in the skin, since blacks need a lot more sunlight to synthesize the hormone than whites do, and the main culprit is the environment: not getting enough sunlight (Harris, 2006). I will provide further evidence for the theory.
The etiology of prostate cancer is not known (ACA, 2016; Bashir, 2015). The cause for the disparity in racial differences in prostate cancer may possibly come down to circulating vitamin D levels, with sunlight playing a large role in the variance. Racial differences in prostate cancer were larger in areas with less sunshine (Taksler et al, 2013). However, it is not known whether getting more sunlight (though the problem would still be getting enough in places with low levels of sunlight) or supplementing with vitamin D will help close the gap. Vitamin D is relevant for lethal prostate cancer (Shui et al 2012), whereas Li et al (2007) showed that supplementing with higher rates of vitamin D, especially during the winter months, may be particularly beneficial to men with low levels of circulating vitamin D. A study on veterans showed that men who had prostate cancer AND the lowest levels of vitamin D were more likely to die than veterans who had higher levels of the hormone (Der et al, 2014). Murphy et al (2014) showed in a biopsy, that in black Americans, low levels of vitamin D were associated with increased the odds of prostate cancer acquisition during the biopsy.
Black Americans are significantly more likely than European Americans to suffer from and die from prostate cancer (Hardiman et al, 2016). A difference of over 8,000 genes were found to be expressed differently. Blacks also have higher rates of prostate tumors and higher grade tumors than do European men. The racial disparity in prostate cancer mirrors circulating levels of vitamin D in the blood between the races (Nelson et 2016). Prostate cells become less sensitive to vitamin D through loss of receptors or signaling molecules “that mediate vitamin D’s actions, or through changes in metabolic enzymes that synthesize or degrade vitamin D compounds” (Peehl and Feldman, 2013). Hardiman et al (2016) showed that there were over 3,000 genes that differed between blacks and whites. Due to the fact that blacks are living outside of their ancestral climes, this is a large mediator of the prostate cancer gap. Vitamin D deficiency can also explain a large variation of the black-white prostate cancer gap (Grant and Peiris 2011).
Along with direct measurement of circulating vitamin D in the bloodstream, we also have correlates. Hypertension is correlated with prostate cancer: blacks have higher rates of hypertension; obesity further exacerbates the problem. Blacks males are more likely to be obese (though barely, which is where the other environmental factors come in). Men suffering from two or more health problems linked to metabolic syndrome are more likely to get prostate cancer. Blacks are more likely to get metabolic syndrome.
Clearly, a large portion of the variation in prostate cancer acquisition and mortality can be attributed to environmental factors (vitamin D intake specifically). We can also look to East Asia and their increasing rates of prostate cancer as well (Chen et al, 2014; Zhu et al, 2014). There are no genetic changes in the past ten years to account for this, so the only culprit is diet. Our Americanized diets have been making it to East Asia recently and it’s having a negative effect on them. China’s obesity rate is dramatically increasing, along with their rates of prostate cancer acquisition. It seems that the Western diet could also play a part in racial differences in prostate cancer acquisition.
To be fair the non-significance of this result might be attributable to the small number (only four) of African nations in the analysis. A number of previous studies have actually found that people of African descent on average do have shorter CAG repeats than other peoples (Ackerman et al., 2012; Esteban et al., 2005; Kittles et al., 2001; Lange et al., 2008). However, whether this actually indicates anything about the life history strategy of different populations remains questionable. The two other androgen indicators for which African data was available follow a completely different pattern. For androgenic hair, Caucasians have the highest rate, followed by Asians, then Africans. For prostate cancer, Caucasians have the highest rate, followed by Asians and Africans, who do not significantly differ.
The difference comes down, mostly in my opinion, due to diet. You can see this by looking at rates of prostate cancer in populations that have adopted, or are current adopting our Western diet.
There is a good chance that environmental factors explain a large part of the variance in prostate cancer acquisition and mortality. I, of course, do not deny intrinsic genetic explanations or other hormonal imbalances, however this is the best explanation I’ve come across. The fact that sunlight dictates prostate cancer acquisition is a huge tell and should be further researched.
I used to be a proponent of the testosterone theory, however, Richard et al (2014) shows a 2.5 to 4.9 percent difference in free testosterone between blacks and whites, which they conclude, does not explain the disparity between the races. Hormones do matter, and hormones can and do vary individually and by group, which are mediated by diet. Once we find out which foods either hurt or help prostate cancer growth, then we can have better treatments for this disease for men of all races.
There are numerous ways in which prostate cancer can be mitigated, with diet obviously playing a large factor (Son, Aronson, and Litwin, 2005; Lin, 2015; Nelson, Demarzo, and Yegnasubramanian, 2014). Future studies researching the racial disparities in prostate cancer should take into account UV radiation from the sun, circulating vitamin D in the blood, and diet amongst a myriad of other variables (these three just stand out to me). Moreover, large-scalre cohorts should be undertaken to see what effects diet can have on the mortality of those suffering from prostate cancer, as possibly supplementing vitamin D to attempt to fight the disease
Are There Race Differences in Penis Size? Part II
1000 words
I haven’t completely discredited the notion that Rushton and Lynn may be correct on this variable, but I’m highly skeptical. Hormonal data doesn’t show it. Hormones like IGF-1 and androgen don’t show the differences between races that would lead you to believe that Rushton’s Rule applies here.
PP is at it again, citing the same studies, not providing primary sources, and not addressing what I say to him about hormones in regards to penis size. Hormones affect the body in different ways, and different races have different levels of hormones. This is what I will discuss today.
Insulin-like growth factor 1 (IGF-1) is a hormone that, as it’s name implies, is structurally similar to the hormone insulin. IGF-1 is “partly responsible for systemic GH activities although it possesses a wide number of own properties (anabolic, antioxidant, anti-inflammatory and cytoprotective actions).” Laron and Klinger (1998) showed that children with Laron syndrome who stopped receiving IGF-1 injections showed reductions in penile and testicular size and they returned to pretreatment serum levels. This shows the effects of IGF-1 on sexual organ size.
Knowing this about IGF-1, for Rushton’s theory to be plausible, Blacks would have higher levels, Asians the lowest, and whites in the middle, skewing towards Asians. Platz et al (1999) investigated whether there were racial differences in circulating IGF-1 and insulin-like growth factor-binding protein 3 (IGFBP-3). IGFBP-3 binds IGF-1 and 2, with a dysregulation of IGFBP-3 correlating with cancer. IGFBP-3 is the main transporter of IGF-1 and 2 in the blood stream. The researchers tested men whose self-described ancestry (we know that self-describer ancestry is a great proxy for race, having a 99.86 percent success rate) African American (63) a random sample of Asians and Caucasians (75 respectively) aged 45 to 78 years old. Caucasians had the highest levels of IGF-1 (224 ng/ml), Asians (208 ng/ml), and African Americans (205 ng/ml). The IGF-1:IGFBP-3 ratio was greatest in Caucasians and lowest in Asians. This study was carried out to see if IGF-1 had an effect on prostate cancer. The 13 percent difference in IGFBP-3 between blacks and whites may account for the higher levels of prostate cancer, as IGFBP-3 can control IGF-1 bioavailabilty.
PP also cites Ross et al (1986) showing that blacks have “19 percent higher testosterone”, attempting to use this as evidence for the theory in favor of an inverse relationship between brain size and penis size. He seems to think that total testosterone matters, when what matters is free testosterone.It’s also 15 percent circulating testosterone, 13 percent free testosterone in that one study. Free testosterone is biologically active, and is able to exert its effect by passing through a cell and activating its receptor. Speaking of free testosterone, in this meta-analysis of 23 studies on black-white differences in testosterone, Richard et al (2014) showed a 2.5 to 4.9 percent difference in free testosterone and concluded that that difference was not enough to account for the racial disparity in prostate cancer. So it’s either black Americans have lower levels of IGFBP-3 or diet/environmental factors that cause this racial disparity in prostate cancer, not testosterone.
Rohrmann et al (2007) showed that testosterone differences between blacks (n=363) and whites (n=674) did not noticeably differ (5.29 ng/ml and 5.11 ng/ml respectively). Mexican Americans (n=376) , on the other hand, showed a higher average rate (5.48 ng/ml) over both cohorts. Blacks had higher levels of estradiol than whites (40.80 pg/nl and 35.46 pg/nl respectively). Blacks also had a higher level of sex hormone-binding globulin (SHGB) (36.49 nmol/liter) than whites (34.91 nmol/liter) and Mexican Americans (34.91 nmol/liter). That may account for some of the racial disparity in prostate cancer, but it’s not testosterone (which shows that ‘higher levels of testosterone’ as PP says, isn’t proof of any racial differences in penis size).
The Kinsey data is nonrepresentative and nonrandom. We have comparative sizes for certain ethnies, and the only statistical difference is between Nigerians and Koreans and Czechs. Rushton and Boegart didn’t mention that blacks danced less than white college students, blacks are more prudish regarding nudity, more likely to have a prostitute as a sexual partner and less likely to want large families (Weizmann et al, 1990). A study on certain CAG repeats shows that Africans cluster with East Asians on two measures, contradicting Lynn’s hypothesis. French Army Surgeon, lol (see Weizman et al 1990 from above):
This work is filled with internal contradictions. For example, an average African Negro penis is said to be 7 3/4 to 8 inches long on p. 56, while on p. 242 it is stated that it “generally exceeds” 9 inches. Similarly, while the French Army surgeon announces on p. 56 that he once discovered a 12-inch penis, an organ of that size becomes “far from rare” on p. 243. As one might presume from such a work, there is no indication of the statistical procedures used to compute averages, what terms such as “often” mean, how subjects were selected, how measurements were made, what the sample sizes were, etc.
I think I’ve shown that there are no “””racial””” differences in size with the Veale et al 2014 study and the Orakwe and Ebuh (2007) study. As far as I see, two statistical differences exist between Nigerians and Koreans and Czechs. But there’s not enough “””quality data””” to say “this race bigger than that race”. To believe there are racial differences in penis size or that there is even an inverse relationship between penis size and brain size takes a huge leap of faith to believe.
There are, without a doubt, average differences in a lot of things between races; hormones being one of them. Any differences between races in IGF-1 have no effect on penis size (IGF-1 is, however, one reason why black girls reach menarche at a younger age than white girls. Will write more on that in the future.). Africans were more similar to Asians that Caucasians on two of the five androgen indicators that Dutton (2015) tested. The Kinsey data is nonrepresentative and nonrandom and that is what PP continuously references. I’m highly skeptical leading towards no based on my knowledge of hormones and how they work in the human body. Testosterone does not explain any racial differences in penis size, and does not explain any differences in prostate cancer acquisition (though, other hormones do).
