
Home » Posts tagged 'testosterone' (Page 2)
Tag Archives: testosterone
Find the Genes: Testosterone Version
1600 words
Testosterone has a similar heritability to IQ (between .4 and .6; Harris, Vernon, and Boomsma, 1998; Travison et al, 2014). To most, this would imply a significant effect of genes on the production of testosterone and therefore we should find a lot of SNPs that affect the production of testosterone. However, testosterone production is much more complicated than that. In this article, I will talk about testosterone production and discuss two studies which purport to show a few SNPs associated with testosterone. Now, this doesn’t mean that the SNPs cause high/low testosterone, just that they were associated. I will then speak briefly on the ‘IQ SNPs’ and compare it to ‘testosterone SNPs’.
Testosterone SNPs?
Complex traits are ‘controlled’ by many genes and environmental factors (Garland Jr., Zhao, and Saltzman, 2016). Testosterone is a complex trait, so along with the heritability of testosterone being .4 to .6, there must be many genes of small effect that influence testosterone, just like they supposedly do for IQ. This is obviously wrong for testosterone, which I will explain below.
Back in 2011 it was reported that genetic markers were discovered ‘for’ testosterone, estrogen, and SHGB production, while showing that genetic variants in the SHGB locus, located on the X chromosome, were associated with substantial testosterone variation and increased the risk of low testosterone (important to keep in mind) (Ohlsson et al, 2011). The study was done since low testosterone is linked to numerous maladies. Low testosterone is related to cardiovascular risk (Maggio and Basaria, 2009), insulin sensitivity (Pitteloud et al, 2005; Grossman et al, 2008), metabolic syndrome (Salam, Kshetrimayum, and Keisam, 2012; Tsuijimora et al, 2013), heart attack (Daka et al, 2015), elevated risk of dementia in older men (Carcaillon et al, 2014), muscle loss (Yuki et al, 2013), and stroke and ischemic attack (Yeap et al, 2009). So this is a very important study to understand the genetic determinants of low serum testosterone.
Ohlsson et al (2011) conducted a meta-analysis of GWASs, using a sample of 14,429 ‘Caucasian’ men. To be brief, they discovered two SNPs associated with testosterone by performing a GWAS of serum testosterone concentrations on 2 million SNPs on over 8,000 ‘Caucasians’. The strongest associated SNP discovered was rs12150660 was associated with low testosterone in this analysis, as well as in a study of Han Chinese, but it is rare along with rs5934505 being associated with an increased risk of low testosterone(Chen et al, 2016). Chen et al (2016) also caution that their results need replication (but I will show that it is meaningless due to how testosterone is produced in the body).
Ohlsson et al (2011) also found the same associations with the same two SNPs, along with rs6258 which affect how testosterone binds to SHGB. Ohlsson et al (2011) also validated their results: “To validate the independence of these two SNPs, conditional meta-analysis of the discovery cohorts including both rs12150660 and rs6258 in an additive genetic linear model adjusted for covariates was calculated.” Both SNPs were independently associated with low serum testosterone in men (less than 300ng/dl which is in the lower range of the new testosterone guidelines that just went into effect back in July). Men who had 3 or more of these SNPs were 6.5 times more likely to have lower testosterone.
Ohlsson et al (2011) conclude that they discovered genetic variants in the SHGB locus and X chromosome that significantly affect serum testosterone production in males (noting that it’s only on ‘Caucasians’ so this cannot be extrapolated to other races). It’s worth noting that, as can be seen, these SNPs are not really associated with variation in the normal range, but near the lower end of the normal range in which people would then need to seek medical help for a possible condition they may have.
In infant males, no SNPs were significantly associated with salivary testosterone levels, and the same was seen for infant females. Individual variation in salivary testosterone levels during mini-puberty (Kurtoglu and Bastug, 2014) were explained by environmental factors, not SNPs (Xia et al, 2014). They also replicated Carmaschi et al (2010) who also showed that environmental factors influence testosterone more than genetic factors in infancy. There is a direct correlation between salivary testosterone levels and free serum testosterone (Wang et al, 1981; Johnson, Joplin, and Burin, 1987), so free serum testosterone was indirectly tested.
This is interesting because, as I’ve noted here numerous times, testosterone is indirectly controlled by DNA, and it can be raised or lowered due to numerous environmental variables (Mazur and Booth, 1998; Mazur, 2016), such as marriage (Gray et al, 2002; Burnham et al, 2003; Gray, 2011; Pollet, Cobey, and van der Meij, 2013; Farrelly et al, 2015; Holmboe et al, 2017), having children (Gray et al, 2002; Gray et al, 2006; Gettler et al, 2011); to obesity (Palmer et al, 2012; Mazur et al, 2013; Fui, Dupuis, and Grossman, 2014; Jayaraman, Lent-Schochet, and Pike, 2014; Saxbe et al, 2017) smoking is not clearly related to testosterone (Zhao et al, 2016), and high-carb diets decrease testosterone (Silva, 2014). Though, most testosterone decline can be ameliorated with environmental interventions (Shi et al, 2013), it’s not a foregone conclusion that testosterone will sharply decrease around age 25-30.
Studies on ‘testosterone genes’ only show associations, not causes, genes don’t directly cause testosterone production, it is indirectly controlled by DNA, as I will explain below. These studies on the numerous environmental variables that decrease testosterone is proof enough of the huge effects of environment on testosterone production and synthesis.
How testosterone is produced in the body
There are five simple steps to testosterone production: 1) DNA codes for mRNA; 2) mRNA codes for the synthesis of an enzyme in the cytoplasm; 3) luteinizing hormone stimulates the production of another messenger in the cell when testosterone is needed; 4) this second messenger activates the enzyme; 5) the enzyme then converts cholesterol to testosterone (Leydig cells produce testosterone in the presence of luteinizing hormone) (Saladin, 2010: 137). Testosterone is a steroid and so there are no ‘genes for’ testosterone.
Cells in the testes enzymatically convert cholesterol into the steroid hormone testosterone. Quoting Saladin (2010: 137):
But to make it [testosterone], a cell of the testis takes in cholesterol and enzymatically converts it to testosterone. This can occur only if the genes for the enzymes are active. Yet a further implication of this is that genes may greatly affect such complex outcomes as behavior, since testosterone strongly influences such behaviors as aggression and sex drive. [RR: Most may know that I strongly disagree with the fact that testosterone *causes* aggression, see Archer, Graham-Kevan and Davies, 2005.] In short, DNA codes only for RNA and protein synthesis, yet it indirectly controls the synthesis of a much wider range of substances concerned with all aspects of anatomy, physiology, and behavior.
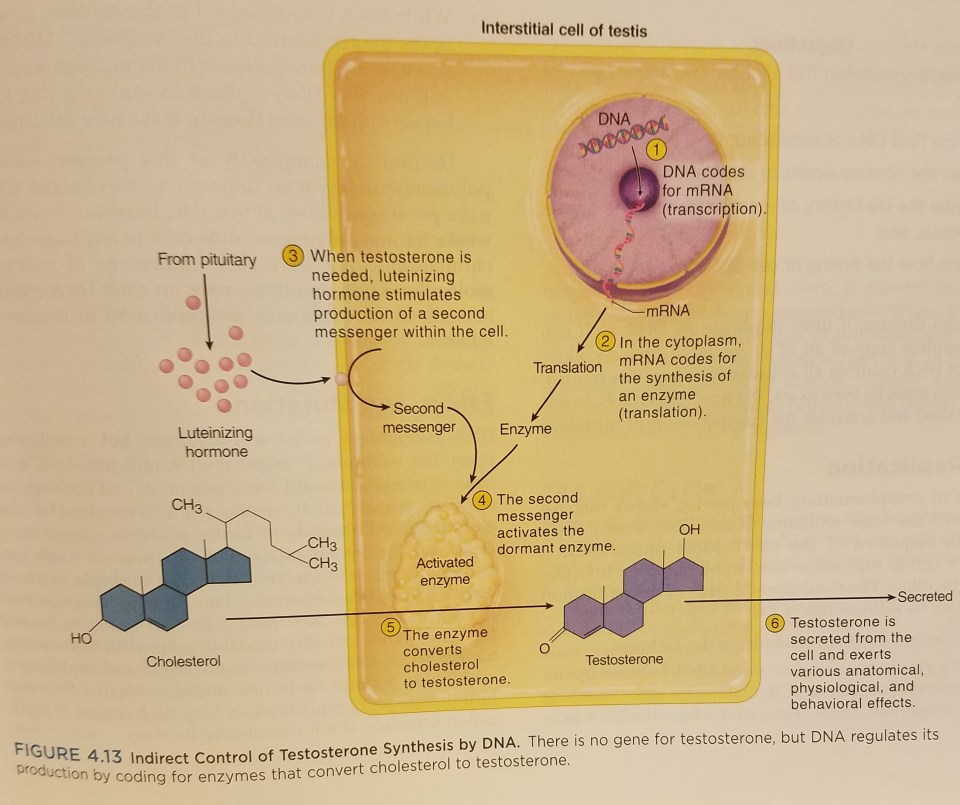
(Figure from Saladin (2010: 137; Anatomy and Physiology: The Unity of Form and Function)
Genes only code for RNA and protein synthesis, and thusly, genes do not *cause* testosterone production. This is a misconception most people have; if it’s a human trait, then it must be controlled by genes, ultimately, not proximately as can be seen, and is already known in biology. Genes, on their own, are not causes but passive templates (Noble, 2008; Noble, 2011; Krimsky, 2013; Noble, 2013; Also read Exploring Genetic Causation in Biology). This is something that people need to understand; genes on their own do nothing until they are activated by the system.
What does this have to do with ‘IQ genes’?
My logic here is very simple: 1) Testosterone has the same heritability range as IQ. 2) One would assume—like is done with IQ—that since testosterone is a complex trait that it must be controlled by ‘many genes of small effect’. 3) Therefore, since I showed that there are no ‘genes for’ testosterone and only ‘associations’ (which could most probably be mediated by environmental interventions) with low testosterone, may the same hold true for ‘IQ genes/SNPS’? These testosterone SNPs I talked about from Ohlsson et al (2011) were associated with low testosterone. These ‘IQ SNP’ studies (Davies et al, 2017; Hill et al, 2017; Savage et al, 2017) are the same—except we have an actual idea of how testosterone is produced in the body, we know that DNA is indirectly controlling its production, and, most importantly, there is/are no ‘gene[s] for’ testosterone.
Conclusion
Testosterone has the same heritability range as IQ, is a complex trait like IQ, but, unlike how IQ is purported to be, it [testosterone] is not controlled by genes; only indirectly. My reasoning for using this example is simple: something has a moderate to high heritability, and so most would assume that ‘numerous genes of small effect’ would have an influence on testosterone production. This, as I have shown, is false. It’s also important to note that Ohlsson et al (2011) showed associated SNPs in regards to low testosterone—not testosterone levels in the normal range. Of course, only when physiological values are outside of the normal range will we notice any difference between men, and only then will we find—however small—genetic differences between men with normal and low levels of testosterone (I wouldn’t be surprised if lifestyle factors explained the lower testosterone, but we’ll never know that in regards to this study).
Testosterone production is a real, measurable physiologic process, as is the hormone itself; which is not unlike the so-called physiologic process that ‘g’ is supposed to be, which does not mimic any known physiologic process in the body, which is covered with unscientific metaphors like ‘power’ and ‘energy’ and so on. This example, in my opinion, is important for this debate. Sure, Ohlsson et al (2011) found a few SNPs associated with low testosterone. That’s besides the point. They are only associated with low testosterone; they do not cause low testosterone. So, I assert, these so-called associated SNPs do not cause differences in IQ test scores; just because they’re ‘associated’ doesn’t mean they ’cause’ the differences in the trait in question. (See Noble, 2008; Noble, 2011; Krimsky, 2013; Noble, 2013.) The testosterone analogy that I made here buttresses my point due to the similarities (it is a complex trait with high heritability) with IQ.
Evidence for Testosterone Influencing Sports Performance
1200 words
Back in July I wrote about how there is controversy on whether or not MtF transgenders should compete with ‘bio women’ and whether or not their anthropometry or hormones gave them an advantage over biological women (I am aware that T levels decrease once they go on HRT, just a lot of them still have T ranges in near the low end of the new numbers for men). Well I am reading The Sports Gene by Jerry Epstein and he brings up two (anecdotal) examples of MtF transgenders who take HRT and see a decrease in performance due to decreased T:
No scientist can claim to know the precise impact of testosterone on any individual athlete. But a 2012 study that spent three months following female athletes from a range of sports—including track and field and swimming—showed that elite-level competitors had testosterone levels that consistently remained more than twice as high as those of the nonelites. And there are powerful anecdotes as well.
Joanna Harper, fifty-five, is a medical physicist who was born a male and later transitioned to living as a woman. Harper also happens to be a nationally accomplished age-group runner, and when she started hormone therapy in August 2004 to suppress her body testosterone and physically transition to female [Note from RR: I, of course, do not agree with the use of ‘her’ and that ‘she’ ‘physically transition[ed] to female’] like any good scientist, she took data. Harper figured she would slow down gradually, but was surprised to find herself getting slower and weaker by the end of the first month. “I felt the same when I ran,” she says. “I just couldn’t go as fast.” In 2012, Harper won the U.S. national cross-country title for the fifty-five-to-fifty-nine age group, but age and gender-graded performance standards indicate that Harper is precisely as competitive now as a female as she was as a male. That is, as a female, Harper is just as good relative to women as she was relative to men before her transition, but she’s far slower than her former, higher-testosterone self.
In 2003, as a man, Harper ran Portland’s Helvetia Half-Marathon in 1:23:11. In 2005, as a woman, she ran the same race in 1:34:01. Harper’s male time was about fifty seconds faster than her female time. She has compiled data from five other runners who have transitioned from male to female, and all show the same pattern of precipitous speed decline. One runner competed in the same 5K for fifteen years straight, eight times as a man and then seven times as a woman following testosterone suppression therapy; always faster than nineteen minutes as a man, and always slower than twenty minutes as a woman. (Epstein, 2013: 78) [Keep in mind that I have the nook version so the physical copy may have this on a different page.
Yes this is anecdotal evidence that testosterone gave an advantage while ‘male’ and then when they ‘transitioned’ to ‘female’ it showed that they became weaker, but still at the top level of women’s performance. Knowing this—how this man had an advantage ‘as a man’ and kept the same relative advantage when he ‘transitioned to a woman’ is a large clue that testosterone does infer an inherent advantage to athletes who have more of the hormone surging through their body.
Testosterone is known to affect skeletal muscle growth, but the mechanisms by which testosterone affects muscle growth are not known (Bhasin, Woodhouse, and Storer, 2001). Also, women with very high androgen levels—whether it’s due to endogenous or exogenous testosterone—have a 2.5 to 5 percent advantage over women who have androgen levels in the normal range (Berman, 2017). So the difference in performance—between women at least—with high and low levels of testosterone is not too great, though that 2.5 to 5 percent advantage most likely would come into play at the very end of the race.
Also recall that I previously wrote that, per the IOC guidelines, a ‘MtF’ needs to ‘declare herself’ a woman for at least four years while taking HRT for 1-2 years to be able to compete with ‘the gender they think they are’. Well, the testosterone levels that the IOC states is ‘OK’ for ‘MtFs’ is still in the low range of the new testosterone guidelines for men! Testosterone most definitely does give an advantage in sports. Think of sports as a modern day test of survival. Basically, those good at sports—such as football and basketball for instance—would have been better able to form hunting parties in our evolutionary past. So while forming these parties, testosterone rose since testosterone raises while men are in groups as well as preparing for competition (Booth et al, 1989). So since our modern body plans sprang up around 2 mya with the appearance of Homo erectus in the fossil record, we can logically infer that cooperation and testosterone—among other things—were needed to be successful hunters.
So if you look at most sports as just a way for men to have a competitive spirit and simulate fighting/hunting with other men, then it makes it clear that testosterone does infer an advantage in sports. For instance, there is a clear relationship between testosterone and explosive jumping (Cardinale and Stone, 2006). These relationships are very clear, have large effects yet bodies like the IOC disregard these findings, allowing MtFs to compete with real women, even when the data and verbal argumentation against letting them compete are logically sound.
Studies do state, of course, that the relationship between high testosterone and athletic performance hasn’t been proven, they also haven’t been refuted either (Sudai, 2017). In fact, all you need to look at is traits that are influenced by testosterone—height, size of limbs, fat mass, shoulder width/size (the most androgen receptors lie in the shoulders and traps muscles, so to tell if someone is juicing, they will have low levels of body fat but ‘3-D delts’ and large traps) etc. So just by looking at a few simple traits and then comparing anatomy with females who have high testosterone compared to women who do not have high levels of testosterone, we can draw the logical conclusion that testosterone does increase sports performance for both men and women, and we have both anecdotal and experimental evidence for the assertion.
In sum, the anecdotal evidence from Epstein’s book is a good start. However, we will need more than anecdotal evidence to prove that testosterone truly does give individuals an advantage if they do have higher testosterone levels than their competition. As larger studies get done, these effects will begin to get teased out. I am certain that testosterone will be found to give a huge advantage in terms of sports, and since sports are a way for us to compete with each other, impress women, gauge other males’ fighting skills, and began as a way to hone skills used to hunt and fight (Lombardo, 2012). Sports began as a way for us to develop the skills needed to survive and hunt, among other things, and so, to hunt, you need to have high levels of testosterone to give that ‘boost’. So if sports began as a way to gauge potential rivals and allies, and as a way to hone/improve fighting skills, then we can logically state that testosterone does give an advantage in sports competition.
Testosterone: “The Crime Gene?”
1150 words
I came across this video on YouTube last night by a geneticist/science writer Steve Jones. He is also the Emeritus Professor of genetics at University College London. This makes what he says in the video I will speak about below very troubling—especially to a man of his caliber with the knowledge he has—views he has on the hormone.
In the very beginning of the video titled Testosterone and Crime: What Can Genes Tell Us About Behavior?, Jones says “But in fact, there are genes—there is a gene—for crime, which causes nearly all the crime, and is widely used and we understand a great deal about it. It’s a chemical gene it produces a particular chemical, which we understand in detail is the chemical testosterone. Testosterone—we all have it but some of us have rather more than others—testosterone is of course a gene that is made—switched on by the Y chromosome and makes males male. Women have a small amount but only a small amount and as they get older … Now testosterone is a dangerous, dangerous thing to have. I don’t recommend it, those of you who have it, don’t get it. And if you’ve got some, don’t get any more.” What bullshit! This guy is a literal genetics Ph.D. saying this; this is proof that knowledge/educational attainment does not stop you from saying dumb, untrue things.
“I don’t know that this character does it, but certainly plenty of bodybuilders inject steroids—testosterone—into themselves. They damage themselves severely. Their life expectancy goes down strikingly. They die for all those male reasons. They die from violence, they die from suicide, they die from car accidents, they die from heart disease, all those things are true of males. … But even if you look at males and females in general, there is kind of a depressing picture for half of the room, I’m not sure which half.” Jones then talks about how men die at a much higher rate than women for a slew of reasons. This is his logic: Men have higher testosterone than women. Testosterone is shown to cause violence, aggression, heart disease, risk-taking, etc. Men have way more testosterone than women. Therefore testosterone is the reason why men die more than women and commit more violence than women. This is horrible logic—coming from a geneticist no less!
“Men actually—less expectedly perhaps—are much less good at dealing with parasites and infectious disease than women are. And that’s because testosterone—the male hormone—suppresses the immune system. Now the immune system fights off the parasites and we don’t do nearly as well.” There is actually some empirical data for his argument here. Back in 2013, it was shown that testosterone, gene expression, and the immune system were linked. They discovered that higher levels of testosterone prevented Module 52 genes from turning on. So higher levels of testosterone result in more Module 52 expression. Testosterone also does exert immune-suppressing effects, “increasing the severity of malaria, leishmaniasis, amebiasis, and tuberculosis, while at the same time supporting the clearance of toxoplasmosis (Bernin & Lotter, 2014; Nhamoyebonde & Leslie, 2014)” (Giefing-Kroll et al, 2015). The suppressive effects of testosterone on the immune system and how down-regulates “the systemic immune response by cell type specific effects in the context of immunological disorders.” (Trigunaite, Dimo, and Jorgensen, 2015).
The effects of testosterone replacement therapy (TRT) on the immune system have not been looked into, but it has a positive effect on elderly men (Osterberg, Bernie, and Ramasamy, 2014). However, Braude, Tang-Martinez, and Taylor (1999) challenge the wisdom that testosterone is an immuno-depressor. This is Jones’ only claim that is not outright wrong; there is data out there for both positions (of course I think that Braude, Tang-Martinez and Taylor, 1999 drive a solid argument against the testosterone-causes-immuno-suppression hypothesis).
The Jones says one of the dumbest things I’ve ever heard “And men, of course, are murdered much more than women. And who murders them—of course—other men. … Men murder at a much higher rate than women. … And that effect is striking—that effect is true worldwide—all over the world men, testosterone, murder at 10 times the rate of women. … So it’s a universal, it’s a biological universal, it’s clearly due to testosterone. There’s no question. The evidence is absolutely clear. So it’s a genetic phenomenon, it’s a gene for crime.” Should I be nice here and assume that whatever ‘gene’ he’s proposing that ’causes’ testosterone production actually causes the crime? Or should I take what he said at face value—that testosterone is a literal gene that causes crime? I think I’ll go with the second one.
“It’s certainly genetic, it’s also environmental. And you can’t disentangle it. You can change part of it—the environment—you can’t change the other part—the genes. And I always find it kind of odd that the public is so interested in the bit you can’t change—the genes—and is so uninterested in the bit you can—the environment.” This is wrong. Not all of it, but most of it. I don’t think that people are more interested in genes and toss aside environment—especially for testosterone. Because, as I documented yesterday, hereditarians assume that since testosterone has a heritability of around .6 then it must be mostly genetic in nature. This is wrong. As Jones said, the environment effects testosterone production too (though he didn’t go into the mechanisms).
The Left goes to the environment side—change the environment, change hormone production (this is true)—whereas the Right goes to the genes side—can’t change genes and environment is a product of genes so nothing can be done. (Oversimplified, don’t crucify me.) Both are wrong. Strong genetic determinism (gene G almost always leads to the development of trait T. (G increases the probability of T and the probability of T, given G, is 95% or greater) doesn’t make sense because a large majority of traits are moderately or weakly determined by genetics (Resnick and Vorhaus, 2006).
In sum, Jones is clueless about testosterone. He only really said one thing that is not outright wrong (but it is questionable). It doesn’t cause crime, it doesn’t cause men to murder more. The press has gotten all of these views into people’s heads because they want to demonize men—and the hormone that is largely responsible for male-ness. It’s incredible that this guy is both a geneticist, science writer and professor of genetics and still calls testosterone a ‘gene’ saying that it is responsible for ‘most of the crime’ committed. Anyone who has been reading this blog for the past year or so since I have began revising many of my main views knows how wrong this is. People really need to get a clue on testosterone and stop spreading bullshit. I know that I’ll have to keep correcting misconceptions on testosterone for a good long time (like with r/K theory) but I enjoy writing about both things so it’s not too big a deal. I just wish people would actually educated themselves on basic physiology so that the trainwreck of a video that Jones made does not get made.
No, Black Women Do Not Have Higher Testosterone than White Women (And More On Hereditarian Claims on Racial Testosterone Differences)
1850 words
It has been over a year since I wrote the article Black Women and Testosterone, and I really regret it. Yes, I did believe that black women had higher levels of testosterone than white women due to one flimsy study and another article on pregnant black women. I then wised up to the truth about testosterone and aggression/crime/race/sex and revised the articles (like I have done with r/K selection theory). However, after I revised my views on the supposed differences in testosterone between black men/white men and black women/white women, people still cite the article, disregarding the disclaimer at the top of the article. I quoted Mazur (2016), who writes (emphasis mine):
The pattern [high testosterone] is not seen among teenage boys or among females.
…
There is no indication of inordinately high T among young black women with low education.
…
Honor cultures are cast as male affairs, but with T data in hand for both sexes, it is worth exploring whether or not a similar pattern exists among women. Mean T was calculated as a function of age for the four combinations of race and education used in Table 1 but now for women. All plots show T declining with age, from about 35 ng/dL in the 20–29 age group to about 20 ng/dL among women 60 years and older. The four plots essentially overlap without discernible differences among them. Given the high skew of T among adult females, both raw and ln-transformed values were analyzed with similar results. There is no indication of inordinately high T among young black women with low education.
…
In the present study, at least, the sexes differ because the very high T seen among young black men with low education does not occur among young black women with low education.
This is very clear… Mazur (2016) analyzed the NHANES 2011-2012 data and this is what he found. I understand that most HBD bloggers do believe this, well, like a lot of their strong assertions (which I have rebutted myself), they’re wrong. They don’t get it. They do not understand the hormone.
The reason why I’m finally writing this (which is long overdue) is that I saw a referral from this website today: https://www.minds.com/RedPillTV who writes about the aforementioned black women and testosterone article:
It is known that blacks have the highest levels of testosterone out of the major races of humanity. However, what’s not known is that black women have higher rates than white women. The same evolutionary factors that make it possible for black men to have high testosterone make it possible for women as well.
https://notpoliticallycorrect.me/2016/09/06/black-women-and-testosterone/
…..No. It seems that people just scroll on by the disclaimer at the top that is bolded and italicized and just go to the (now defunct) article and attempt to prove their assertion that black women have higher testosterone than white women with an article that I have stated myself I no longer believe and have provided the rationale/data for the position. This shows that people have their own biases and no matter what the author writes about their views that have changed due to good arguments/data, they will still attempt to use the article to prove their assertion.
I’ve written at length that testosterone does not cause 1) aggression, 2) crime and 3) prostate cancer. People are scared of testosterone mostly due to the media fervor of any story that may have a hint of ‘toxic masculinity’. They (most alt-righters) are scared of it because of Lynn/Rushton/Templer/Kanazawa bullshit on the hormone. Richard Lynn doesn’t know what he’s talking about on testosterone. No, Europeans did not need lower levels of aggression in the cold; Africans didn’t need higher levels of aggression (relative to Europeans) to survive in the tropics. The theory that supposed differential testosterone differences between the races are “the physiological basis in males of the racial differences in sexual drive which form the core of the different r/K reproduction strategies documented by J.P. Rushton” (Lynn, 1990: 1203). The races, on average, do not differ in testosterone as I have extensively documented. So hereditarians like Lynn and others need to look for other reasons to explain blacks’ higher rate of sexual activity.
Rushton’s views on the testosterone and supposed r/K continuum have been summarily rebutted by me. These psychologists’ views on the hormone (that they don’t understand the production of nor do they understand the true reality of the differences between the races) are why people are afraid of testosterone. No, testosterone is not some ‘master switch’ as Rushton (1999) asserts. Rushton asserts that racial differences in temperament are mediated by the hormone testosterone. He further dives into this assertion stating “Testosterone level correlates with temperament, self-concept, aggression, altruism, crime, and sexuality, in women as well as in men (Harris, Rushton, Hampson, & Jackson, 1996). It may ‘correlate’ with aggression and crime, but as I have documented, they do not cause either.
The aggression/testosterone correlation is only .08 (Archer, Graham-Kevan, and Davies, 2005). Furthermore, the diurnal variation in testosterone does not directly correlate to when testosterone levels are highest in the day (at 8 am and drop thereafter), with adults peaking in crime at 10 pm and kids at 3 pm, with rises at 8 pm and 12 pm (not surprisingly, kids go in to school around 8 am, go to recess at 12 and leave at 3).

(Source: The Office of Juvenile Justice and Delinquency Prevention (OJJDP))
If you’ve read as much Rushton as I have, you’ll notice that he begins to sound like a broken record when talking about certain things. One of the most telling is Rushton’s repeated assertions that blacks average 3-19 percent higher testosterone than whites. The 3 percent number comes from Ellis and Nyborg (1992) and the 19 percent number comes from Ross et al (1986) (which Rushton should know that after adjustments for confounding, it decreased to 13 percent). These are the only studies that hereditarians ever cite for these claims that blacks average higher testosterone than whites. That seems a bit fishy to me. Cite a 30-year-old study along with a 25-year-old study (with such huge variation from Rushton and those who cite him for this matter—3-19 percent!!) as ‘proof’ that blacks average such higher levels of testosterone in comparison to whites.
Ross et al (1986) is one of the most important studies to rebut for this hereditarian claim that testosterone causes all of these maladies in black American populations. Ross et al (1986) propose that higher levels of the hormone lead to the higher rates of prostate cancer in black American populations. However, meta-analyses do not show this (Zagars et al, 1998; Sridhar et al, 2010).
Rushton et al’s assertions—largely—lie on this supposed testosterone difference between the races and how it supposedly leads to higher rates of crime, prostate cancer, aggression, and violence. However, the truth of the matter is, this is all just hereditarian bullshit. Larger analyses—as I have extensively documented—do not show this trend. And even accepting the claim that blacks have, say, 19 percent higher levels of testosterone than whites, it still would not explain the supposed prostate cancer rates between the races (Stattin et al, 2003; Michaud, Billups, and Partin, 2015). Even if blacks had 19 percent higher testosterone than whites, it would not explain higher levels of crime nor aggression due to such a hilariously low correlation of .08 (Archer, Graham-Kevan, and Davies, 2005).
Finally, I have a few words for Michael Hart and his (albeit sparse) claims on testosterone in his 2007 book Understanding Human History.
Hart (2007) writes:
(Many of these differences in sexual behavior may be a consequence of the fact that
blacks, on average, have higher levels of testosterone than whites.7) (pg. 127)
And….. footnote number 7 is…. surprisingly (not): 7) Ross, R., et al. (1986). Not going to waste my time on this one, again. I’ve pointed out numerous flaws in the study. (I will eventually review the whole thing.)
It seems unlikely, though, that the higher testosterone level in blacks — which is largely genetic in origin — has no effect on their sexual behavior (pg. 128; emphasis mine)
This is bullshit. People see the moderately high heritability of testosterone (.60; Harris, Vernon, and Boomsma, 1998) and jump right to the “It’s genetics!!!” canard without even understanding its production in the body (it is a cholesterol-based hormone which is indirectly controlled by DNA, there are no ‘genes for’ testosterone). Here are the steps: 1) DNA codes for mRNA; 2) mRNA codes for the synthesis of an enzyme in the cytoplasm; 3) luteinizing hormone stimulates the production of another messenger in the cell when testosterone is needed; 4) this second messenger activates the enzyme; 5) the enzyme then converts cholesterol to testosterone
I have documented numerous lines of evidence showing that testosterone is extremely sensitive to environmental factors (Mazur and Booth, 1998; Mazur, 2016), and due to the homeodynamic physiology we have acquired due to ever-changing environments (Richardson, 2017), this allows our hormones to up- or down-regulate depending on what occurs in the environment. The quote from Hart is bullshit; he doesn’t know what he’s talking about.
For females in Siberia, the disadvantages of failing to find a man who would
provide for her and her children during their childhood were much greater than they were in tropical climates, and females who were not careful to do so were much less likely to pass on their genes. Furthermore, because females in harsh climates were so demanding on this point, males who seemed unlikely to provide the needed assistance found it hard to find mates. In other words, there was a marked sexual selection against such males. Such selection could result, for example, in the peoples living in northerly climates gradually evolving lower levels of testosterone than the peoples living in subSaharan Africa. (pg. 131)
This is a bullshit just-so story. Africans in Africa have lower levels of testosterone than Western men (Campbell, O’Rourke, and Lipson, 2003; Lucas and Campbell, and Ellison, 2004; Campbell, Gray, and Ellison, 2006).
Note also that a difference in testosterone level frequently affects not
only the sexual behavior of a young male, but also his aggressiveness.
No it does not (Archer, Graham-Kevan, and Davies, 2005).
Thankfully, that’s all he wrote about testosterone. There is so much bullshit out there. Though, people who like and seek out the truth will learn that there are no racial differences and that testosterone does not cause crime/aggression/prostate cancer and that it’s just hereditarian bullshit.
The evidence I have amassed and the arguments I have given point to a few things: 1) the races do not differ in testosterone/there is a small negligible difference; 2) testosterone does not cause crime; 3) testosterone does not cause aggression; 4) black women do not have higher levels of testosterone than white women; 5) high levels of testosterone do not cause prostate cancer; and 6) even allowing a 19 percent black/white difference will not have hereditarian claims hold true.
So for anyone who comes across my old articles on testosterone and sex/race, do a bit more reading of my newer material here to see my new viewpoints/arguments. DO NOT cite these articles as proof for your claims of higher levels of black men/women. DO cite the old articles ALONG WITH the new ones to show how and why my views changed along with the studies I have cited that changed my view. (Actually understanding the production of testosterone in the body was a huge factor too, which I talk about in Why Testosterone Does Not Cause Crime.)
Does Testosterone Affect Human Cognition and Decision-Making?
1450 words
According to a new article published at The Guardian, testosterone does affect human cognition and decision-making. The article, titled, Now we men can blame our hormones: testosterone is trouble, by Phil Daoust, is yet more media sensationalism against testosterone. Daoust’s article is full of assumptions and conclusions that do not follow from an article he cites on testosterone and cognitive reflection and decision making.
The cited article, Single dose testosterone administration impairs cognitive reflection in men, states that endogenous testosterone (testosterone produced in the body) is correlated with physical aggression. However, I’ve shown that this is not true. They conclude overall the exogenous testosterone is related to an increase in irrational thinking and decision-making. Nothing wrong with concluding that from the data. However, Daoust’s interpretation and conclusions he draws from this study are wrong, mostly due to the same old tales and misconceptions about testosterone.
This is the largest study of the effect of exogenous testosterone and decision-making and cognition. The authors show that men administered a gel that was rubbed into the upper body that is used for TRT (testosterone replacement therapy) showed “incorrect intuitive answers were more common, and correct answers were less common in the T group, for each of the three CRT questions analyzed separately” (Nave et al, 2017: 8). However, what The Guardian article does not state is that this relationship could be mediated by more than testosterone, such as motivation and arithmetic skills.
Nevertheless, those who rubbed themselves with the testosterone gel answered 20 percent fewer questions correctly. This was attributed to the fact that they were more likely to be anxious and not think about the answer. One of the authors also states that either testosterone inhibits the action of mentally checking your work or it increases the intuitive feeling that you’re definitely right (since those who rubbed themselves with T gel gave more intuitive answers, implying that the testosterone made them go to their first thought in their head). I have no problems with the paper—other than the fact that gel has an inconsistent absorption rate and has high rates of aromatization. The study has a good design and I hope it gets explored more. I do have a problem with Dauost’s interpretation of it, however.
A host of studies have already shown a correlation between elevated testosterone levels and aggression – and now they’re being linked to dumb overconfidence.
The ‘host of studies‘ that ‘have already shown a correlation between elevated testosterone levels and aggression‘ don’t say what you think they do. This is another case of the testosterone sensationalism of the media—talking about a hormone they don’t really know anything about.
That won’t help with the marketing – though it may explain Donald Trump and his half-cocked willy-waggling. Perhaps it’s not the president’s brain that’s running things, but the Leydig cells in his testicles.
Nice shot. This isn’t how it works, though. You can’t generalize a study done on college-aged males to a 71-year-old man.
Women aren’t entirely off the hook – their bodies also produce testosterone, though in smaller quantities, and the Caltech study notes that “it remains to be tested whether the effect is generalisable to females” – but for now at least they now have another way to fight the scourge of mansplaining: “You’re talking out of your nuts.”
Another paragraph showing no understanding, even bringing up the term ‘mansplaining’—whatever that means. This article is, clearly, demonizing high T men, and is a great example of the media bias on testosterone studies that I have brought up in the past.
Better still, with the evils of testosterone firmly established, the world may learn to appreciate older men. Around the age of 30, no longer “young, dumb and full of cum”, we typically find our testosterone levels declining, so that with every day that passes we become less aggressive, more rational and generally nicer.
“The evils of testosterone firmly established“, nice job at hiding your bias. Yes the cited article (Nave et al 2017) does bring up how testosterone is linked to aggression. But, for the millionth time, the correlation between testosterone and aggressive behavior is only .08 (Archer, Graham-Kevan, and Davies, 2005).
Even then, most of the reduction of this ‘evil hormone’ is due to lifestyle changes. It just so happens that around the ages 25-30—when most men notice a decrease in testosterone levels—that men begin to change their lifestyle habits, which involve marriage which decreases testosterone levels (Gray et al, 2002; Burnham et al, 2003; Gray, 2011; Pollet, Cobey, and van der Meij, 2013; Farrelly et al, 2015; Holmboe et al, 2017), having children (Gray et al, 2002; Gray et al, 2006; Gettler et al, 2011) to obesity (Palmer et al, 2012; Mazur et al, 2013; Fui, Dupuis, and Grossman, 2014; Jayaraman, Lent-Schochet, and Pike, 2014; Saxbe et al, 2017) smoking is not clearly related to testosterone (Zhao et al, 2016), and high-carb diets decrease testosterone (Silva, 2014).
So the so-called age-related decline in testosterone is not really age-related at all—it has to do with environmental and social factors which then decreases testosterone (Shi et al, 2013). Why should a man be ‘happy’ that his testosterone levels are decreasing due—largely—to his lifestyle? Low testosterone is related to cardiovascular risk (Maggio and Basaria, 2009), insulin sensitivity (Pitteloud et al, 2005; Grossman et al, 2008), metabolic syndrome (Salam, Kshetrimayum, and Keisam, 2012; Tsuijimora et al, 2013), heart attack (Daka et al, 2015), elevated risk of dementia in older men (Carcaillon et al, 2014), muscle loss (Yuki et al, 2013), and stroke and ischemic attack (Yeap et al, 2009).
So it seems that, contrary to Phil Daoust’s (the author of The Guardian article on testosterone) claims that low testosterone is associated with less aggressive behavior, more rationality and being nicer, in general, are wrong. Low testosterone is associated with numerous maladies, and the Daoust is trying to make low testosterone out to be ‘a good thing’, while demonizing men with higher levels of testosterone with cherry-picked studies and not large meta-analyses like I have cited that show that testosterone has an extremely low correlation with aggressive behavior.
As I have covered in the past, testosterone levels in the West are declining, along with semen count and quality. These things are due, largely in part, to social and environmental factors such as obesity, low activity, and an overall change in lifestyle. One (albeit anecdotal) reason I could conjure up has to do with dominance. Testosterone is the dominance hormone and so if testosterone levels are declining, then that means men must not be showing dominance as much. I would place part of the blame here on feminism and articles like the one reviewed here as part of the problem. So contra the author’s assertion, lower levels of testosterone into old age are not good, since that signifies a change in lifestyle—many of which are in the control of the male in question (I, of course, would not advise anyone to not have children or get married).
Nave et al (2017) lead the way for further research into this phenomenon. If higher doses of exogenous testosterone do indeed inhibit cognitive reflection, then, as the authors note, “The possibility that this widely prescribed treatment has unknown deleterious influences on specific aspects of decision-making should be investigated further and taken into account by users, physicians, and policy makers” (Nave et al, 2017: 11). This is perhaps one of the most important sentences in the whole article. This is about the application of testosterone-infused gel and decision-making. They’re talking about the implications of administering the gel to men and how it affects decision-making and cognitive reflection. This study is NOT generalizable for 1) endogenous testosterone and 2) non-college students. If the author understood the paper and science, he wouldn’t make those assumptions about Trump’s Leydig cells in his testicles “running the show”.
Because of the testosterone fear, good studies like Nave at al (2017) get used for an agenda by people who don’t understand the hormone. People the the Right and Left both have horrible misconceptions about the hormone, and some cannot interpret studies correctly and draw the correct conclusions from them. Testosterone—endogenous or exogenous—does not cause aggression (Batrinos, 2012). This is an established fact. The testosterone decrease between the ages of 25-30 is avoidable if you don’t change to bad habits that decrease testosterone. All in all, the testosterone scare is ridiculous. People are scared of it because they don’t understand it.
Daoust didn’t understand the article he cited and drew false conclusions from his misinterpretations. I would be interested to see how men would fare on a cognitive reflection test after, say, their favorite team scored during a game, and not after being given supraphysiological doses of testosterone gel. Drawing conclusions like Daoust did, however, is wrong and will mislead numerous more people under the guise of science.
Responses to The Alternative Hypothesis and Robert Lindsay on Testosterone
2300 words
I enjoy reading what other bloggers write about testosterone and its supposed link to crime, aggression, and prostate cancer; I used to believe some of the things they did, since I didn’t have a good understanding of the hormone nor its production in the body. However, once you understand how its produced in the body, then what others say about it will seem like bullshit—because it is. I’ve recently read a few articles on testosterone from the HBD-blog-o-sphere and, of course, they have a lot of misconceptions in them—some even using studies I have used myself on this blog to prove my point that testosterone does not cause crime!! Now, I know that most people don’t read studies that are linked, so they would take what it says on face value because, why not, there’s a cite so what he’s saying must be true, right? Wrong. I will begin with reviewing an article by someone at The Alternative Hypothesis and then review one article from Robert Lindsay on testosterone.
The Alternative Hypothesis
Faulk has great stuff here, but the one who wrote this article, Testosterone, Race, and Crime, 1) doesn’t know what he’s talking about and 2) clearly didn’t read the papers he cited. Read this article, you’ll see him make bold claims using studies I have used for my own arguments that testosterone doesn’t cause crime! Let’s take a look.
One factor which explains part of why Blacks have higher than average crime rates is testosterone. Testosterone is known to cause aggression, and Blacks are known to at once have more of it and, for genetic reasons, to be more sensitive to its effects.
- No it doesn’t.
- “Testosterone is known to cause aggression“, but that’s the thing: it’s only known that it ’causes’ aggression, it really doesn’t.
- Evidence is mixed on blacks being “… for genetic reasons … more sensitive to its effects” (Update on Androgen Receptor gene—Race/History/Evolution Notes).
Testosterone activity has been linked many times to aggression and crime. Meta-analyses show that testosterone is correlated with aggression among humans and non human animals (Book, Starzyk, and Quinsey, 2001).
Why doesn’t he say what the correlation is? It’s .14 and this study, while Archer, Graham-Kevan and Davies, (2005) reanalyzed the studies used in the previous analysis and found the correlation to be .08. This is a dishonest statement.
Women who suffer from a disease known as congenital adrenal hyperplasia are exposed to abnormally high amounts of testosterone and are abnormally aggressive.
Abnormal levels of androgens in the womb for girls with CAH are associated with aggression, while boys with and without CAH are similar in aggression/activity level (Pasterski et al, 2008), yet black women, for instance, don’t have higher levels of testosterone than white women (Mazur, 2016). CAH is just girls showing masculinized behavior; testosterone doesn’t cause the aggression (See Archer, Graham-Kevan and Davies, 2005)
Artificially increasing the amount of testosterone in a person’s blood has been shown to lead to increases in their level of aggression (Burnham 2007; Kouri et al. 1995).
Actually, no. Supraphysiological levels of testosterone administered to men (200 and 600 mg weekly) did not increase aggression or anger (Batrinos, 2012).
Finally, people in prison have higher than average rates of testosterone (Dabbs et al., 2005).
Dabbs et al don’t untangle correlation from causation. Environmental factors can explain higher testosterone levels (Mazur, 2016) in inmates, and even then, some studies show socially dominant and aggressive men have the same levels of testosterone (Ehrenkraz, Bliss, and Sheard, 1974).
Thus, testosterone seems to cause both aggression and crime.
No, it doesn’t.
Why Testosterone Does Not Cause Crime
Testosterone and Aggressive Behavior
Furthermore, of the studies I could find on testosterone in Africans, they have lower levels than Western men (Campbell, O’Rourke, and Lipson, 2003; Lucas and Campbell, and Ellison, 2004; Campbell, Gray, and Ellison, 2006) so, along with the studies and articles cited on testosterone, aggression, and crime, that’s another huge blow to the testosterone/crime/aggression hypothesis.
Richard et al. (2014) meta-analyzed data from 14 separate studies and found that Blacks have higher levels of free floating testosterone in their blood than Whites do.
They showed that blacks had 2.5 to 4.9 percent higher testosterone than whites, which could not explain the higher prostate cancer incidence (which meta-analyses call in to question; Sridhar et al 2010; Zagars et al 1998). That moderate amount would not be enough to cause differences in aggression either.
Exacerbating this problem even further is the fact that Blacks are more likely than Whites to have low repeat versions of the androgen receptor gene. The androgen reception (AR) gene codes for a receptor by the same name which reacts to androgenic hormones such as testosterone. This receptor is a key part of the mechanism by which testosterone has its effects throughout the body and brain.
The rest of the article talks about CAG repeats and aggressive/criminal behavior, but it seems that whites have fewer CAG repeats than blacks.
Robert Lindsay
This one is much more basic, and tiring to rebut but I’ll do it anyway. Lindsay has a whole slew of articles on testosterone on his blog that show he doesn’t understand the hormone, but I’ll just talk about this one for now: Black Males and Testosterone: Evolution and Perspectives.
It was also confirmed by a recent British study (prostate cancer rates are somewhat lower in Black British men because a higher proportion of them have one White parent)
Jones and Chinegwundoh (2014) write: “Caution should be taken prior to the interpretation of these results due to a paucity of research in this area, limited accurate ethnicity data, and lack of age-specific standardisation for comparison. Cultural attitudes towards prostate cancer and health care in general may have a significant impact on these figures, combined with other clinico-pathological associations.”
This finding suggests that the factor(s) responsible for the difference in rates occurs, or first occurs, early in life. Black males are exposed to higher testosterone levels from the very start.
In a study of women in early pregnancy, Ross found that testosterone levels were 50% higher in Black women than in White women (MacIntosh 1997).
I used to believe this, but it’s much more nuanced than that. Black women don’t have higher levels of testosterone than white women (Mazur, 2016; and even then Lindsay fails to point out that this was pregnant women).
According to Ross, his findings are “very consistent with the role of androgens in prostate carcinogenesis and in explaining the racial/ethnic variations in risk” (MacIntosh 1997).
Testosterone has been hypothesized to play a role in the etiology of prostate cancer, because testosterone and its metabolite, dihydrotestosterone, are the principal trophic hormones that regulate growth and function of epithelial prostate tissue.
Testosterone doesn’t cause prostate cancer (Stattin et al, 2003; Michaud, Billups, and Partin, 2015). Diet explains any risk that may be there (Hayes et al, 1999; Gupta et al, 2009; Kheirandish and Chinegwundoh, 2011; Williams et al, 2012; Gathirua-Mingwai and Zhang, 2014). However in a small population-based study on blacks and whites from South Carolina, Sanderson et al (2017) “did not find marked differences in lifestyle factors associated with prostate cancer by race.”
Regular exercise, however, can decrease PCa incidence in black men (Moore et al, 2010). A lot of differences can be—albeit, not too largely— ameliorated by environmental interventions such as dieting and exercising.
Many studies have shown that young Black men have higher testosterone than young White men (Ellis & Nyborg 1992; Ross et al. 1992; Tsai et al. 2006).
Ellis and Nyborg (1992) found 3 percent difference. Ross et al (1992) have the same problem as Ross et al (1986), which used University students (~50) for their sample. They’re not representative of the population. Ross et al (1992) also write:
Samples were also collected between 1000 h and 1500 h to avoid confounding
by any diurnal variation in testosterone concentrations.
Testosterone levels should be measured near to 8 am. This has the same time variation too, so I don’t take this study seriously due to that confound. Assays were collected “between” the hours of 10 am and 3 pm, which means it was whenever convenient for the student. No controls on activities, nor attempting to assay at 8 am. People of any racial group could have gone at whatever time in that 5 hour time period and skew the results. Assaying “between” those times completely defeats the purpose of the study.
This advantage [the so-called testosterone advantage] then shrinks and eventually disappears at some point during the 30s (Gapstur et al., 2002).
Gapstur et al (2002) help my argument, not yours.
This makes it very difficult if not impossible to explain differing behavioral variables, including higher rates of crime and aggression, in Black males over the age of 33 on the basis of elevated testosterone levels.
See above where I talk about crime/testosterone/aggression.
Critics say that more recent studies done since the early 2000’s have shown no differences between Black and White testosterone levels. Perhaps they are referring to recent studies that show lower testosterone levels in adult Blacks than in adult Whites. This was the conclusion of one recent study (Alvergne et al. 2009) which found lower T levels in Senegalese men than in Western men. But these Senegalese men were 38.3 years old on average.
Alvergne, Fauri, and Raymond (2009) show that the differences are due to environmental factors:
This study investigated the relationship between mens’ salivary T and the trade-off between mating and parenting efforts in a polygynous population of agriculturists from rural Senegal. The men’s reproductive trade-offs were evaluated by recording (1) their pair-bonding/fatherhood status and (2) their behavioral profile in the allocation of parental care and their marital status (i.e. monogamously married; polygynously married).
They also controlled for age, so his statement “But these Senegalese men were 38.3 years old on average” is useless.
These critics may also be referring to various studies by Sabine Rohrmann which show no significance difference in T levels between Black and White Americans. Age is poorly controlled for in her studies.
That is one study out of many that I reference. Rohrmann et al (2007) controlled for age. I like how he literally only says “age is poorly controlled for in her studies“, because she did control for age.
That study found that more than 25% of the samples for adults between 30 and 39 years were positive for HSV-2. It is likely that those positive samples had been set aside, thus depleting the serum bank of male donors who were not only more polygamous but also more likely to have high T levels. This sample bias was probably worse for African American participants than for Euro-American participants.
Why would they use diseased samples? Do you even think?
Young Black males have higher levels of active testosterone than European and Asian males. Asian levels are about the same as Whites, but a study in Japan with young Japanese men suggested that the Japanese had lower activity of 5-alpha reductase than did U.S. Whites and Blacks (Ross et al 1992). This enzyme metabolizes testosterone into dihydrotestosterone, or DHT, which is at least eight to 10 times more potent than testosterone. So effectively, Asians have the lower testosterone levels than Blacks and Whites. In addition, androgen receptor sensitivity is highest in Black men, intermediate in Whites and lowest in Asians.
Wu et al (1995) show that Asians have the highest testosterone levels. Evidence is also mixed here as well. See above on AR sensitivity.
Ethnicmuse also showed that, contrary to popular belief, Asians have higher levels of testosterone than Africans who have higher levels of testosterone than Caucasians in his meta-analysis. (Here is his data.)
The Androgen Receptor and “masculinization”
Let us look at one study (Ross et al 1986) to see what the findings of a typical study looking for testosterone differences between races shows us. This study gives the results of assays of circulating steroid hormone levels in white and black college students in Los Angeles, CA. Mean testosterone levels in Blacks were 19% higher than in Whites, and free testosterone levels were 21% higher. Both these differences were statistically significant.
Assay times between 10 am and 3 pm, unrepresentative sample of college men, didn’t have control for waist circumference. Horribly study.
A 15% difference in circulating testosterone levels could readily explain a twofold difference in prostate cancer risk.
No, it wouldn’t (if it were true).
Higher testosterone levels are linked to violent behavior.
Causation not untangled.
Studies suggest that high testosterone lowers IQ (Ostatnikova et al 2007). Other findings suggest that increased androgen receptor sensitivity and higher sperm counts (markers for increased testosterone) are negatively correlated with intelligence when measured by speed of neuronal transmission and hence general intelligence (g) in a trade-off fashion (Manning 2007).
Who cares about correlations? Causes matter more. High testosterone doesn’t lower IQ. Racial differences in testosterone are tiring to talk about now, but there are still a few more articles I need to rebut.
Conclusion
Racial differences in testosterone don’t exist/are extremely small in magnitude (as I’ve covered countless times). The one article from TAH literally misrepresents studies/leaves out important figures in the testosterone differences between the two races to push a certain agenda. Though if you read the studies you see something completely different. It’s the same with Lindsay. He misunderstood a few studies to push his agenda about testosterone and crime and prostate cancer. They’re both wrong, though.
Why Testosterone Does Not Cause Crime
Testosterone and Aggressive Behavior
Race, Testosterone, and Prostate Cancer
Population variation in endocrine function—Race/History/Evolution Notes
Racial differences in testosterone are tiring to talk about now, but there are still a few more articles I need to rebut. People read and write about things they don’t understand, which is the cause of these misconceptions with the hormone, as well as, of course, misinterpreting studies. Learn about the hormone and you won’t fear it. It doesn’t cause crime, prostate cancer nor aggression; these people who write these articles have one idea in their head and they just go for it. They don’t understand the intricacies of the endocrine system and how sensitive it is to environmental influence. I will cover more articles that others have written on testosterone and aggression to point out what they got wrong.
Racial Differences in Testosterone…again
1200 words
Testosterone is a fascinating hormone—the most well-known hormone to the lay public. What isn’t well-known to the lay public is how the hormone is produced and the reasons why it gets elevated. I’ve covered racial differences in testosterone in regards to crime, penis size and Rushton’s overall misuse of r/K selection theory. In this article, I will talk about what raises and decreases testosterone, as well as speak about racial differences in testosterone again since it’s such a fun topic to cover.
JP Rushton writes, in his 1995 article titled Race and Crime: An International Dilemma:
One study, published in the 1993 issue of Criminology by Alan Booth and D. Wayne Osgood, showed clear evidence of a testosterone-crime link based on an analysis of 4,462 U.S. military personnel. Other studies have linked testosterone to an aggressive and impulsive personality, to a lack of empathy, and to sexual behavior.
Booth and Osgood (1993: 93) do state that “This pattern of results supports the conclusions that (I) testosterone is one of a larger constellation of factors contributing to a general latent propensity toward deviance and (2) the influence of testosterone on adult deviance is closely tied to social factors.” However, as I have extensively documented, the correlation between testosterone and aggression is extremely low (Archer, 1991; Book et al (2001); Archer, Graham-Kevan and Davies, 2005), and therefore cannot be the cause of crime.
Another reason why testosterone is not the cause of aggression/deviant behavior is due to what times most crimes are committed at. Therefore, testosterone cannot possibly be the cause of crime. I’ve also shown that, contrary to popular belief, blacks don’t have higher levels testosterone than whites, along with the fact that testosterone does not cause prostate cancer, that even if blacks did have these supposed higher levels of the hormone, that it would NOT explain higher rates of crime.
Wu et al (1995) show that Asian Americans had the highest testosterone levels, African Americans were intermediate and European Americans were last, after adjustments for BMI and age were made. Though, I’ve shown in larger samples that, if there is any difference at all (and a lot of studies show no difference), it is a small advantage favoring blacks. We then are faced with the conclusion that this would not explain disease prevalence nor higher rates of crime or aggression.
Testosterone, contrary to Rushton’s (1999) assertion, is not a ‘master switch’. Rushton, of course, cites Ross et al (1986) which I’ve tirelessly rebutted. Assay times were all over the place (between 10 am and 3 pm) with testosterone levels being highest at 8 am. The most important physiological variable in Rushton’s model is testosterone, and without his highly selected studies, his narrative falls apart. Testosterone doesn’t cause crime, aggression, nor prostate cancer.
The most important take away is this: Rushton’s r/K theory hinges on 1) blacks having higher levels of testosterone than whites and 2) that these higher levels of testosterone then influence higher levels of aggression which lead to crime and then prostate cancer. Even then, Sridhar et al (2010) meta-analyzed 17 articles which talk about racial differences in prostate cancer survival rates. They state in their conclusion that “there are no differences between African American and Whites in survival from prostate cancer.” Zagars et al (1998) show that there were no significant racial differences in serum testosterone. Furthermore, when matched for major prognostic factors “the outcome for clinically local–regional prostate cancer does not depend on race (6,7,14–19). Moreover there appear to be no racial differences in the response of advanced prostate cancer to androgen ablation (29,47). Our study provides further evidence that racial differences in disease outcome are absent for clinically localized prostate cancer” (Zagars et al, 1998: 521). So it seems that these two studies also provide further support that Rushton et al were wrong in regards to prostate cancer mortality as well.
Rushton (1997 185) writes:
In any case, socialization cannot account for the early onset of the traits, the speed of dental and other maturational variables, the size of the brain, the number of gametes produced, the physiological differences in testosterone, nor the evidence on cross-cultural consistency.
There are no racial differences in testosterone and if there were, social factors would explain the difference between the races. However, as I’ve noted in the past, testosterone levels are high in young black males with low educational attainment (Mazur, 2016). The higher levels of testosterone in blacks compared to whites (which, if you look at figure 1 the levels are not high at all) is accounted for by honor culture, a social variable. Furthermore, the effects of the environment are also more notable on testosterone than are genetics at 5 months of age (Carmaschi et al, 2010). Environmental factors greatly influence testosterone (Booth et al, 2006), so Rushton stating that “socialization cannot account for the early onset” of “physiological differences in testosterone” is clearly wrong since environmental influences can be seen in infants as well as adults. Testosterone is strongly mediated by the environment; this is not up for debate.
Testosterone is one of many important hormones in the body; the races do not differ in the variable. So, therefore, all of Rushton’s ‘r/K predictions’, which literally hinge on testosterone (Lynn, 1990) fall apart without this ‘master switch’ (Rushton, 1999) driving all of these behaviors. Any theories of crime that include testosterone as a main driver in crime need to be rethunk; numerous studies attest to the fact that testosterone does not cause crime. Racial differences in testosterone only appear in small studies and the studies that do show these differences get touted around all the while, all of the better, larger analyses don’t get talked about because it goes against a certain narrative.
Finally, there is no inevitability of a testosterone decrease in older men. So-called “age-related declines” in the hormone are largely explained by smoking, obesity, chronic disease, marital status, and depression (Shi et al, 2013), and even becoming a father explains lower levels of testosterone (Gray, Yang, and Pope, 2006). On top of that, marriage also reduces testosterone, with men who went from unmarried to married showing a sharp decline in testosterone over a ten-year period (Holmboe et al, 2017). This corroborates numerous other studies showing that marriage lowers testosterone levels in men (Mazur and Michalek, 1998; Nansunga et al, 2014) But some of this decrease may be lessened by frequent sexual intercourse (Gettler et al, 2013). So if you live a healthy lifestyle, the testosterone decrease that plagues most men won’t occur to you. The decreases are due to lifestyle changes; not explicitly tied to age.
People are afraid of higher levels of testosterone at a young age and equally as terrified of lowering testosterone levels at an old age. However, I’ve exhasutively shown that testosterone is not the boogeyman, nor the ‘master switch’ (Rushton, 1999) it’s made out to be. There are no ‘genes for’ testosterone; its production is indirect through DNA. Thusly, if you keep an active lifestyle, don’t become obese, and don’t become depressed, you can bypass the so-called testosterone decrease. Fear mongering on both sides of the ‘testosterone curve’ are seriously blown out of proportion. Testosterone doesn’t cause crime, aggression, nor prostate cancer (even then, large meta-analyses show no difference in PCa mortality between blacks and whites).
The fear of the hormone testosterone is due to ignornace of what it does in the body and how it is produced in the body. If people were to understand the hormone, they would not fear it.
Why Are People Afraid of Testosterone?
1100 words
The answer to the question of why people are afraid of testosterone is very simple: they do not understand the hormone. People complain about birth rates and spermatogenesis, yet they believe that having high testosterone makes one a ‘savage’ who ‘cannot control their impulses’. However, if you knew anything about the hormone and how it’s vital to normal functioning then you would not say that.
I’ve covered why testosterone does not cause crime by looking at the diurnal variation in the hormone, showing that testosterone levels are highest at 8 am and lowest at 8 pm, while children commit the most crimes at 3 pm and adults at 10 pm. The diurnal variation is key: if testosterone truly did cause crime then rates of crime would be higher in both children and adults in the morning; yet, as can be seen with children, there are increases in amounts of violence committed when they enter school, go to recess, and exit school. This shows why those times are related to the spike in crime in children.
I have wrote a previous article citing a paper by Book et al (2001) in which they meta-analyzed testosterone studies and found that the correlation between testosterone and aggression was .14. However, that estimate is too high since they included 15 studies that should have not been included in the analysis. The true correlation is .08 (Archer, Graham-Kevan, and Davies, 2004). So, clearly, along with the fact that the diurnal variation in testosterone does not correlate with crime spikes, it shows that testosterone has no relationship to the cause of crime; it’s just always at the scene because it prepares the body to deal with a threat. That does not mean that testosterone itself causes crime.
One main reason people fear testosterone and believe that it causes crime and by extension aggressive behavior is because of racial crime disparities. According to the FBI, black Americans by and large commit the most crime, despite being 13 percent of the US population. And since it has been reported that blacks have higher levels of testosterone (Ross et al, 1986; Lynn, 1992; Rushton, 1997; Ellis, 2017), people believe that the supposed higher levels of testosterone that blacks, on average, have circulating in their blood is the ultimate cause of the crime disparities in America between races. Though see above to see why this is not the ultimate cause.
Blacks, contrary to popular belief, don’t have higher levels of testosterone (Gasper et al, 2006; Rohrrman et al, 2007; Lopez et al, 2013; Richard et al, 2014). Even if they did have higher levels, say the 13 percent that is often cited, it would not be the cause of higher rates of crime, nor the cause of higher rates of prostate cancer in blacks compared to whites. What does cause part of the crime differential, in my opinion, is honor culture (Mazur, 2016). The blacks-have-higher-testosterone canard was pushed by Rushton and Lynn to explain both higher rates of prostate cancer and crime in black Americans, however I have shown that high levels of testosterone do not cause prostate cancer (Stattin et al, 2003; Michaud, Billups, and Partin, 2015). Looking to testosterone as a ‘master switch’ as Rushton called it is the wrong thing to research because, clearly, the theories of Lynn, Rushton, and Ellis have been rebutted.
People are scared of testosterone because they do not understand the hormone. Indeed, people complain about lower birth rates and lower sperm counts, yet believe that having high testosterone will cause one to be a high T savage. This is seen in the misconception that injecting anabolic steroids causes higher levels of aggression. One study looked at the criminal histories of men who self-reported drug use and steroid use Lundholm et al (2014) who conclude: “We found a strong association between self-reported lifetime AAS use and violent offending in a population-based sample of more than 10,000 men aged 20-47 years. However, the association decreased substantially and lost statistical significance after adjusting for other substance abuse. This supports the notion that AAS use in the general population occurs as a component of polysubstance abuse, but argues against its purported role as a primary risk factor for interpersonal violence. Further, adjusting for potential individual-level confounders initially attenuated the association, but did not contribute to any substantial change after controlling for polysubstance abuse.“
The National Institute of Health (NIH) writes: “In summary, the extent to which steroid abuse contributes to violence and behavioral disorders is unknown. As with the health complications of steroid abuse, the prevalence of extreme cases of violence and behavioral disorders seems to be low, but it may be underreported or underrecognized.” We don’t know whether steroids cause aggression or more aggressive athletes are more likely to use the substance (Freberg, 2009: 424). Clearly, the claims of steroids causing aggressive behavior and crime are overblown and there has yet to be a scientific consensus on the matter. A great documentary on the matter is Bigger, Stronger, Faster, which goes through the myths of testosterone while chronicling the use of illicit drugs in bodybuilding and powerlifting.
People are scared of the hormone testosterone—and by extent anabolic steroids—because they believe the myths of the hulking, high T aggressive man that will fight at the drop of the hat. However, reality is much more nuanced than this simple view and psychosocial factors must also be taken into account. Testosterone is not the ‘master switch’ for crime, nor prostate cancer. This is very simply seen with the diurnal variation of the hormone as well as the peak hours for crime in adolescent and adult populations. The extremely low correlation with aggression and testosterone (.08) shows that aggression is mediated by numerous other variables other than testosterone, and that testosterone alone does not cause aggression, and by extension crime.
People fear things they don’t understand and if people were to truly understand the hormone, I’m sure that these myths pushed by people who are scared of the hormone will no longer persist. Low levels of testosterone are part of the cause of our fertility problems in the West. So does it seem logical to imply that high testosterone is for ‘savages’, when, clearly, high levels of testosterone are needed for spermatogenesis which, in turn, would mean a higher birth rate? Anyone who believes that testosterone causes aggression and crime and that the injection of anabolic steroids causes ‘roid rage’ should do some reading on how the production of the hormone in the body as well as the literature on anabolic steroids. If one wants birth rates to increase in the West, then they must also want testosterone levels to increase as well, since they are intimately linked.
Testosterone does not cause crime and there is no reason to fear the hormone.
The West’s Sperm Decline: Is It True?
2200 words
Another day, another slew of articles full of fear mongering. This one is on sperm decline in the West. Is it true? I have recently covered on this blog that as of July 17th, 2017, the testosterone range for men decreased (more on that when I get access to the paper). I have also covered the obesity epidemic a bit, and that also factors in to lowered testosterone and, of course, low spermatoza count. Due to these environmental factors, we can logically deduce that sperm counts have fallen as well. However, as I will cover, it may not be so cut and dry due to analyzing numerous studies with different counting methodologies among numerous other confounds that will be addressed below. First I will cover the physiology of sperm production and what may cause decreases in production. Next, I will cover the new study that is being passed around. Finally, I will talk about why you should worry about this.
Physiology of sperm production
The accumulation of testosterone by ABP leads to the onset and rising rate of sperm production. So if testosterone production ceases or decreases, then subsequent decreases in sperm count and spermatogenesis should follow. If this change is drastic, infertility will soon follow. The process of sperm production is called spermatogenesis. It occurs in the seminiforous tubules and involves three main events: 1) remodeling relatively large germ cells into smaller mobile cells with flagella, 2) reducing the chromosome number by half, and 3) shuffling the genes so that each chromosome in the sperm carries novel gene combinations that differ from the parents. This is what ensures that a child will differ from their parents but still, at the same time, will be similar to them. The process by which this occurs is called meiosis, in which four daughter cells split which subsequently differentiate sperm (Saladin, 2010: 1063).
After the conclusion of meiosis I, each chromosome is still double stranded, except each daughter cell only has 23 chromosomes becoming a haploid while at the end of meiosis II, there are four haploid cells with 23 single-stranded chromosomes. Fertilization then combined the 23 chromosomes from the father and mother, which “reestablishes the diploid number of 46 chromosomes in the zygote“(Saladin, 2010: 1063-1064).
Spermatogonia divide by mitosis and then enlarge to become primary spermatocyte. The cell is then protected from the immune system since it is going to become genetically different from the rest of the cells in the body. Since the cells are guarded from the body’s immune system, the main spermatocyte undergoes meiosis I, giving rise to equal size haploid and genetically unique secondary spermatocytes. Then, each secondary spermatocyte undergoes meiosis II dividing into two spermatids with a total of four spermatogoniom. Lastly, the spermatozoa undergo no further division but undergoes spermiogenesis in which it differentiates into a single spermatozoon (Saladin, 2010: 1065-1066). Young men produce about 300,000 sperm per minute, about 400 million per day.
Sperm decrease?
The new study was published on July 25, 2017, in the journal Human Reproduction Update titled Temporal trends in sperm count: a systematic review and meta-regression analysis. Levine et al (2017) used 185 studies (n=42,935) and showed a sperm count (SC) decline of .75 percent per year, coming out to a 28.5 percent decrease between 1975 and 2011. Similar declines were seen in total sperm count (TSC) while 156 estimates of serum volume showed little change.
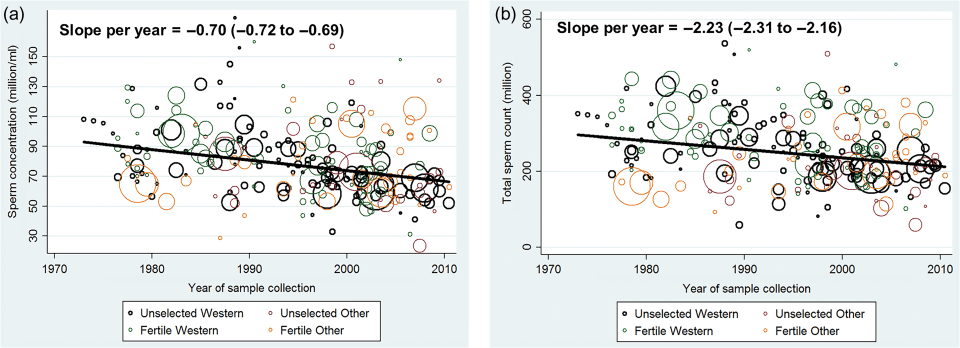
Figure 2a shows the mean sperm concentration between the years 1973 and 2011. Figure 2b shows the mean total sperm count between those same years.
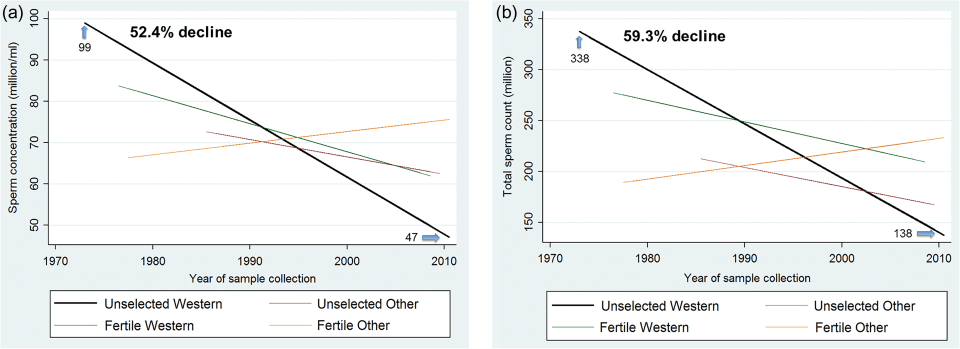
Figure 3a shows sperm concentration for the West (North America, Australia, Europe and New Zealand) vs Other (South America, Asia, and Africa), adjusted for potential confounders such as BMI, smoking etc. Figure 3b shows total sperm count by fertility and the West and Other. You can see that Fertile Other had a sharp increase, but the increase may be due to limited statistical power and a lack of studies of unselected men from those countries before 1985. There is a sharp increase for Other, however and so the data does not support as sharp of a decline as observed in Western countries.
If this is true, why is this happening? Factors that decrease spermatogenesis include (but are not limited to): obesity, smoking, exposure to traffic exhaust fumes, and combustion products. Though there is no data (except animal models) that lend credence to the idea that pesticides, food additives, etc decrease spermatogenesis (Sharpe, 2010). Other factors are known to cause lower SC which includes maternal smoking, alcohol, stress, endocrine disruptors, persistent and nonpersistent chemicals, and, perhaps most importantly today, the use of mobile phones and the wireless Internet (Virtanen, Jorgansen, and Toparri, 2017). Radiation exposure due to constant mobile phone use may cause DNA fragmentation and decreased sperm mobility (Gorpinchenko et al, 2014). Clearly, most of this decrease can largely be ameliorated. Exercise, eating right, and not smoking seem to be the most immediate changes that can and will contribute to an increase in SC in Western men. This will also increase testosterone levels. The cause is largely immobility due to the comfortable lifestyles that we in the West have. So by becoming more active and putting down smartphones, we can then begin to reverse this downward trend.
Saladin (2010: 1067) also states that pollution has deleterious effects on reproduction—and by proxy, sperm production. He states that the evidence is mounting that we are showing declining fertility due to “anatomical abnormalities” in water, meat, vegetables, breast milk and the uterus. He brings up that sperm production decreased in 15,000 men in 1990, decreasing from 113 million/ml in 1940 to 66 million/ml in 1990. Sperm production decreased more, he says, since “the average volume of semen per ejaculate has dropped 19% over this period” (Saladin, 2010: 1067).
Saladin (2010: 1067) further writes:
The pollutants implicated in this trend include a wide array of common herbicides, inseciticides, industrial chemicals, and breakdown products of materials ranging from plastics to dishwashing detergents. Some authorities think these chemicals act by mimicking estrogens by blocking the action of testosterone by binding to its receptors. Other scientists, however, question the data and feel the issue may be overstated. While the debate continues, the U.S. Environmental Protection Agency is screening thousands of industrial chemicals for endocrine effects.
Is it really true?
As seen above, the EPA is investigating whether thousands of industrial chemicals of effects on our endocrine system. If this is true, it occurs due to the binding of these chemicals to androgen receptors, blocking the production of testosterone and thusly sperm production. However, some commentators have contested the results of studies that purport to show a decrease in SC in men over the decades.
Sherins and Delbes are critical of such studies. They rightly state that most of these studies have numerous confounds such as:
1) lack of standardized counting measures, 2) bias introduced by using different counting methodologies, 3) inadequate within-individual semen sampling in the analysis, 4) failure to account for variable abstinence intervals and ejaculatory frequency, 5) failure to assess total sperm output rather than concentration, 6) failure to assess semen parameteres other than the number of sperm, 7) failure to account for age of subject, 8) subject selection bias among comparitive studies, 9) inappropriate statistical analysis, 10) ignoring major geographic differences in sperm counts, and 11) the causal equating of male ferility with sperm count per se.
Levine et al (2017) write:
We controlled for a pre-determined set of potential confounders: fertility group, geographic group, age, abstinence time, whether semen collection and counting methods were reported, number of samples per man and indicators for exclusion criteria (Supplementary Table S1).
So they covered points 1, 2, 4, 5, 6, 7, 8, 9, and 10. This study is very robust. Levine et al (2017) replicate numerous other studies showing that sperm count has decreased in Western men (Centola et al, 2015; Senputa et al, 2017; Virtanen, Jorgensen, and Toparri, 2017). Men Southern Spain show normal levels (Fernandez et al, 2010), while Southern Spanish University students showed a decrease (Mendiola et al, 2013). The same SC decrease has been noted in Brazil in the last ten years (Borges Jr. et al, 2015).
However, te Velde and Bonde (2013) in their paper Misconceptions about falling sperm counts and fertility in Europe contest the results of studies that argue that SC has decreased within the last 50 years stating that, for instance in Denmark, the median values remained between 40-45 million sperm per ml in the 15 years analyzed. They also state that declining birth rates can be explained by cultural and social factors, such as contraception, the female emancipation, and the second demographic transition. Clearly, ferility rates are correlated with the human development index (HDI) meaning that more developed countries have a lower birth rate in comparison to less developed countries. I believe that part of the reason why we in the West have lower birth rates is because there are too many things to for us to do to occupy our time, time that could be used to have children, like going to school to pursue Masters degrees and PhDs, to just wanting more ‘me time’.
Te Velde and Bonde (2013) conclude:
‘Whether the sperm concentration and human fecundity have declined during the past 50 years is a question we will probably never be able to answer’. This statement by Olsen and Rachootin in 200348 still holds for sperm concentration despite the report in 1992. In the meantime, we know that the results of oft-repeated studies from Copenhagen and Malmö do not indicate any notable change in sperm count during the last 10–15 years. Moreover, none of the available evidence points to a decline in couple fecundity during the last 30–40 years, including Denmark.28 Moreover, birth rates and TFRs instead of declining are on the increase in many EU countries, including the spectacular rise in Denmark.34
Echoing the same sentiments, Cocuzza and Esteves (2014) conclude “that there is no enough evidence to confirm a worldwide decline in sperm counts or other semen parameters. Also, there is no scientific truth of a causative role for endocrine disruptors in the temporal decline of sperm production as observed in some studies. We conjecture that a definite conclusion would only be achieved if good quality collaborative long-term research was carried out, including aspects such as semen quality, reproductive hormones, and xenobiotics, as well as a strict definition of fecundity.” Merzenich, Zeeb, and Blettner (2010) also caution that “The observed time trend in semen quality might be an artefact, since the methodological differences between studies might be time dependent as well. Intensive research will be necessary in both clinical and epidemiological domains. More studies are needed with strict methodological standards that investigate semen quality obtained from large samples of healthy men representative for the normal male population.”
Clearly, this debate is long and ongoing, and I doubt that even Levine et al (2017) will be good enough for some researchers.
Conclusion
There are various papers for and against a decrease in sperm production in the West, just like with testosterone. However, there are ways we can deduce that SC has fallen in the West, since we have definitive data that testosterone levels have decreased. This, then, would lead to a decrease in sperm production and then fecundity and number of children conceived by couples. Of course, sociocultural factors are involved, as well as immediate environmental ones that are immediately changeable. Even if there is no scientific consensus on industrial chemicals and effects on the endocrine system, you should stay away from those too. One major reason for the decrease in sperm production—if the decrease is true—is increased mobile phone usage. Mobile phone usage has increased and so this would lower SC over time.
Whether or not the decrease in SC is true or not, every man should take steps to lead a healthier lifestyle without their cell phone. Because if this decrease is true (and Other doesn’t show a decrease as well) then it would be due to the effects of our First World societies, which would mean that we need to change how we live our lives to get back on the right track. Clearly, we must change our diets and our lifestyles. I’ve written numerous articles about how testosterone is strongly mediated by the environment, and that testosterone production in men has decreased since Western men have been, in a way, feminized and not been as dominant. This can and does decrease testosterone production which would, in turn, decrease sperm production and decrease fertility rates.
Nevertheless, taking steps to leading a healthier lifestyle will ameliorate a ton of the problems that we have in the West, which are mainly due to low birth rates, and by ameliorating these problems, the quality of life will the increase in the West. I am skeptical of the decrease due to what was brought up above, but nevertheless I assume that it is true and I hope my readers do too—if only to get some fire under you to lead a healthier lifestyle if you do not do so already as to prevent these problems before they occur and lead to serious deleterious health consequences.
(I am undecided leaning towards yes. There are too many behaviors linked to lower SC which Western men partake in. There are numerous confounds which may have not been controlled for, however knowing the main reasons why men have lower sperm count and the increased prevalence in these behaviors, we can logically deduce that sperm count has fallen too. Look to the testosterone decrease, that causes both low sperm count and lower fertility.)
Preliminary Thoughts on ‘Male-to-Female’ Transgenders in Sports
1500 words
(See my article on transvestic disorder and gender dysphoria for an intro on my view of transgenderism.)
I have been researching male-to-female (MtF) transgenders (TGs) in sports for the past few months. I, like we all do, have my own biases with what should be done with this problem (not letting them compete with women), however jumping to my initial bias there would not be fair so I’ve undertaken the task of reading as many journal articles on the matter as I possibly can. From my research on the matter, there is no direct consensus in the literature that I could come across. In this article, I will show some of the research I’ve found and how it is inconclusive (as well as interject my own thoughts on the matter, mainly speaking about bone density, somatype, and testosterone). (I will cover female-to-male (FtM) transgenders in a future article.)
One recent article making its way around the news is of a MtF who won a weightlifting competition. He (I will be referring to the people I reference by their biological sex) had a total of 590 pounds, besting the second place winner by 42 pounds. Hubbard (the weightlifter who ‘transitioned’) is 39 and has been ‘transitioning’ since his mid-30s. He has also had previous experience competing. The IOC (International Olympic Committee) has no guidelines that a TG athlete must undergo ‘sex-reassignment surgery’, however, they must be on hormone replacement therapy (HRT) for at least 12 months and demonstrate that they have testosterone levels ‘within acceptable limits’. Well, what are ‘acceptable limits’?
The IOC has a short paper on this matter, writing:
The athlete must demonstrate that her total testosterone level in serum has been below 10 nmol/L for at least 12 months prior to her first competition (with the requirement for any longer period to be based on a confidential case-by-case evaluation, considering whether or not 12 months is a sufficient length of time to minimize any advantage in women’s competition).
The athlete’s total testosterone level in serum must remain below 10 nmol/L throughout the period of desired eligibility to compete in the female category.
Compliance with these conditions may be monitored by testing. In the event of non-compliance, the athlete’s eligibility for female competition will be suspended for 12 months.
So the MtF athlete must have a testosterone level of less than 10 nanomoles and declare that they are ‘female’ for at least four years. The IOC states that the individual must be taking HRT for a year or two—whenever they are able to show that their testosterone levels are below that 10 nanomolar mark, they are then allowed to compete. However, other members of the IOC have stated that 10 nanomoles is too high (which is the lower end for males) while arguing that it should be reduced to 3 nanomoles per liter of blood (3 nanomoles is the upper-end for women).
10 nanomoles per liter of blood converts to about 288 ng/dl (nanograms per deciliter). Going with the lower end suggested by other members of the IOC, 3 nanomoles per deciliter of blood converts to 87 ng/dl. The range for women is 15 to 70 ng/dl. Now, the 10 nmol/l is, as you can see, way too high. However, 10 nmol/l converts to slightly higher than the lower end of the new testosterone guidelines for the average male in America and Europe (which I covered yesterday, the new levels being 264-916 ng/dl). As we can see, even 10 nmol/l is way too high and, in my opinion, will give an unfair advantage to these athletes (I know that there is no consensus on whether or not testosterone does give an inherent advantage to MtFs of to hyperandrogenic women; I provide evidence for that below).
In regards to women and hypoandrogenism, Stanton and Wood (2011) state that “excess production of endogenous testosterone due to inborn disorders of sexual development (DSD) may convey a competitive advantage.” The fact of the matter is, endogenous and exogenous testosterone does convey an advantage. So if having higher levels of testosterone conveys a physical advantage in said sport, then 10 nmol/l is way too high. Therefore, the only way (in the eyes of the IOC, not in my opinion) for MtFs to compete with women is to get ‘sex-reassignment surgery’, as the gonads will be removed and testosterone levels will plummet. But how by how much?
In a new review of the literature, Jones et al (2017) state that “there is no direct or consistent research suggesting transgender female individuals (or male individuals) have an athletic advantage at any stage of their transition (e.g. cross-sex hormones, gender-confirming surgery) and, therefore, competitive sport policies that place restrictions on transgender people need to be considered and potentially revised.” They further state that, in most instances, testosterone levels in MtFs “[tended] to be lower than average compared with cisgender women.” So they conclude that there is no evidence that MtFs have no inherent advantage since 1) most of them have lower levels of testosterone than ‘cis-gendered women’, and 2) that there is ‘no evidence’ of testosterone conferring an advantage in athletes (I beg to differ there). The review by Jones et al is a great starting point, however, I disagree with them on numerous things (which I will cover in greater depth in an upcoming, exhaustive research article).
Mueller et al (2011) studied a sample of 84 MtFs who were treated with 10 mg of oestradiol every ten days. They were “treated with subcutaneous injections of 3.8 mg goserelin acetate every 4 weeks to suppress endogenous sex hormone secretion completely.” Follow-ups then commenced at 12 and 24 months. It was found that their BMI, fat mass, and lumbar bone mineral density (BMD) had increased. Conversely, they had a significant decrease in lean mass with a concurrent increase in BMI, which would lead to strength decreases and increased range of motion (ROM), and there was no effect on femoral bone density. This is a larger study than most, most studies having ns of ~20, so the results are robust for this research.
Even if MtFs have a decrease in lean mass and gain in fat mass, they still have inherent biological advantages over women. Testosterone, of course, is not the only reason why men are superior to women in most sports (contrary to the literature). Muscle fiber distribution, cross-sectional area, leverages, etc all play a part in why men are better at sports than women (this is covered at length in Man the Athlete). To the best of my knowledge, cross-sectional area, muscle fiber distribution and leverages don’t change. This is another physical advantage that MtFs would have over ‘cis-gendered women’.
Hyperandrogenic women have also been the center of a lot of controversy (if you follow the Olympics, you may have heard about it occurring during the last Games). Hyperandrogenism affects 5-10 percent of women that are of reproductive age. Signs of hyperandrogenism include hirsutism (hairiness in women), androgenic alopecia (Price, 2003), acne, and virilization (the development of male body hair, bulk, and a deep voice, male-typical characteristics) (Yildiz, 2006). After Caster Semenaya’s dominating win in the middle distance run during last year’s Olympics, the IOC revised their regulations on hyperandrogenic women.
However, Karkazis et al (2016) argued against the IOC and IAAF (International Association of Athletics Federation) stating that “The current scientific evidence, however, does not support the notion that endogenous testosterone levels confer athletic advantage in any straightforward or predictable way.” I strongly disagree with the contention, which I will cover at length in the future. (See Cardinale and Stone, 2006; Wood and Stanton, 2012; Vanny and Moon, 2015.) Of course testosterone is not the only biological factor that confers an advantage, but the difference between hyperandrogenic women and normal women is large (hyperandrogenic women have three times the testosterone compared to normal women, so between 45 to 210 ng/dl). So should they be allowed to compete with women with average levels of testosterone?
Men are built differently than women. Even with HRT, MtFs people would still have an advantage over women. The differences are biological, physiological and anatomic in nature and surgery nor HRT will affect certain factors that would confer an advantage due to the sex the person was born as. That part, in my opinion, is the key factor at play. The difference between MtFs and women do not go away due to surgery and HRT (though some do), so since MtFs have certain biological, anatomical and physiological differences, they should not be allowed to compete with women. That is the one main factor in this debate that is being overlooked. And due to these inherent advantages, they should be barred from competing with women.
This then brings up some interesting implications. Should we segregate competitions by race since the races have strengths and weaknesses due to biology and anatomy, such as somatype? It’s an interesting question to consider, but I think we can all agree on one thing: Women should compete with women, and men should compete with men. Thus, transgenders should compete with transgenders. Even the IOC’s regulations are too high, and in my opinion (contra the literature), testosterone does confer an advantage to those who have it in higher levels (i.e. MtFs). Even then, disregarding testosterone, there are a slew of reasons as to why MtFs should not compete with women which will be covered more in the future.
