
Home » Articles posted by RaceRealist (Page 19)
Author Archives: RaceRealist
Answering Hoffman et al’s 15-Question Questionnaire
1200 words
Hoffman et al (2016) questioned laypeople and medical students and residents on a 15-question questionnaire regarding different beliefs people have about racial differences. The point of the questionnaire was to ascertain how people are biased in regard to racial differences in pain and how the bias affects the treatment the individual of the certain racial group. Only two of the questions had anything to do with pain. In this article, I will answer the questions one by one.
The 15 questions are in the Supporting Information for Hoffman et al (2016). The questions (and my responses) are as follows.
1. On average, Blacks age more slowly than Whites.
This one is true (though they rate this question as false). I don’t know why, though, because there are differences between black and white skin and these differences affect the rate of aging between races.
Campiche et al (2019) found that there is a difference in aging regarding skin in different ethnies (the cohorts were French and Mauritanian). The average age was 46 for the French and 56 foe the Mauritanians, and the Mauritanians still looked younger! Campiche et al (2019) write:
The difference in age between our Caucasian and Black African cohorts (median age 46 years vs 56 years) could bring into question the comparisons of the two cohorts. Nevertheless, we mostly found that Caucasians displayed more severe signs of aging than Black Africans which is in line with the common understanding that the onset of aging in fair skin starts earlier than in darkly pigmented skin and that there were differences in the appearance of lip lines and facial pores.
This question is true, contrary to the claims of Hoffman et al (2016).
2. Black people’s nerve-endings are less sensitive than White people’s nerve-endings.
I can find no literature on this matter and the only articles point me to Hoffman et al (2016) and different articles on the matter. I accept the claim as false.
3. Black people’s blood coagulates more quickly–because of that, Blacks have a lower rate of hemophilia than Whites.
Blacks’ blood does clot faster than whites, and part of the cause is differences in the PAR4 gene family (Bray et al, 2013). The reason that blacks’ blood clots faster than whites’ is due to the effects of thrombin, an enzyme that activates the molecule responsible for blood clotting. Blacks do have a lower rate of hemophilia than whites, though, but not by much (13.2 cases/100,000 for whites compared to 11 for blacks) (Soucie, Evatt, and Jackson, 1998). The question is true, contra Hoffman et al (2016).
4. Whites, on average, have larger brains than Blacks.
They stated that this question is false, which is bizarre. I am aware of no literature that attests to the claim that whites do not have larger brains than blacks. Many analyses back the claim that whites have larger brains than blacks (though Nisbett disagrees and states that there are studies that show the contrary but does not leave a citation) (Rushton, 1997). (Though see Race and Brain Size: Blacks Have Bigger Brains for an alternate view.)
5. Whites are less susceptible to heart disease like hypertension than Blacks.
They say this claim is true. And it is. Hypertension (high blood pressure) is a physiological variable which means that social environment can greatly affect it (Williams, 1992). Higher rates of obesity drive this association as well. American blacks have a lower rate of CHD than whites (7.2 compared to 7.8) but this is reversed for women (7.0 compared to 4.6) (Leigh, Alvarez, and Rodriguez, 2016). The CDC, though, says that the rate of heart disease is the same between blacks and whites, at 23.8 percent though (slightly higher than the 23.5 percent average).
6. Blacks are less likely to contract spinal cord diseases like multiple sclerosis.
They say that this claim is false, and it seems that it is (Langer-Gould et al, 2013). Though Marrie et al (2006) state that blacks experience greater MS disability than whites.
7. Whites have a better sense of hearing compared with Blacks.
They state that this claim is false. Pratt et al (2009) state that hearing loss is more likely to occur in white over black elderly patients.
8. Black people’s skin has more collagen (i.e., it’s thicker) than White people’s skin.
They state that this claim is false, and it is. That there is no difference in skin thickness between blacks and whites is irrelevant, though. Black skin is more compact, with greater intercellular cohesion (LaRuche and Cesarini, 1992; Rawlings, 2006).
9. Blacks, on average, have denser, stronger bones than Whites.
They state that this claim is true, and it is (Wagner and Heyward, 2000; Hocheberg, 2007).
10. Blacks have a more sensitive sense of smell than Whites; they can differentiate odors and detect faint smells better than Whites.
This claim is false, according to Hofmann et al. And I can find nothing in the literature on the matter so I will accept their claim.
11. Whites have more efficient respiratory systems than Blacks.
They state that this claim is false. However, Schwartz et al (1988) state that “Controlling for sex, age, standing height, and body mass index, blacks had consistently lower levels of lung function for most measures.” This claim seems to be true.
12. Black couples are significantly more fertile than White couples.
They state this claim is false. Wellons et al (2008) state that “black women were more likely to have experienced infertility.” So the claim is in the opposite of what Hoffman et al question.
13. Whites are less likely to have a stroke than Blacks.
They state that this claim is true, and it is. Minorities are more likely to have a stroke than whites. Brevata et al (2005) write that blacks are more likely to have severe strokes than whites. The claim is true.
14. Blacks are better at detecting movement than Whites.
This seems like a bizarre claim. They state that it is false and I will accept it as false since I can find no literature on the matter.
15. Blacks have stronger immune systems than Whites and are less likely to contract colds.
Europeans and Africans have different immune systems. The immune system of black Americans is stronger than whites’. Twenty-four hours after being infected with salmonella and listeria bacteria, researchers found that the white blood cells from black Americans responded quicker than that of the white blood cells from white Americans. The white blood cells from black Americans ridded the infection about three times quicker than the white blood cells from black Americans. They stated that this claim is false, but it appears to be true.
So, by my count, out of the 15 questions asked, 8 of them have a factual basis (with some in the opposite direction), compared to Hoffman et al’s (2016) assertion that only 4 of them are true. In any case, there are a lot of myths about racial differences out there, and some of these questions by Hoffman et al are myths. Though some of them do have a factual basis. I wonder what kind of literature they referred to when asking these questions, because the literature that I am aware of when it comes to some of these matters is different compared to what Hoffman et al (2016) claim. Racial/ethnic differences do, obviously, exist but there are many myths involved with them.
Race/Ethnicity and Pain
1700 words
There are many superficial physical differences between the races. But differences in pain sensitivity would be one that is not really “superficial”, as you can’t really see it (you can see someone’s reaction to pain, but not see it). “Pain” is defined as physical discomfort caused by injury. There are some myths about pain differences between racial groups, that still persist today. And these myths have bad consequences.
For example, Hoffman et al (2016) state that “people assume a priori that blacks feel less pain than do whites.” Hoffman et al (2016) carried out two studies: (1) using a between-participants design, laymen were asked to assess the pain of white and black subjects and (2) again using a between-participants design, they asked students and medical doctors to assess pain between blacks and whites. In (2) they asked these 15 questions:
1. On average, Blacks age more slowly than Whites.
2. Black people’s nerve-endings are less sensitive than White
people’s nerve-endings.
3. Black people’s blood coagulates more quickly–because of
that, Blacks have a lower rate of hemophilia than Whites.
4. Whites, on average, have larger brains than Blacks.
5. Whites are less susceptible to heart disease like hypertension than Blacks.
6. Blacks are less likely to contract spinal cord diseases like
multiple sclerosis.
7. Whites have a better sense of hearing compared with Blacks.
8. Black people’s skin has more collagen (i.e., it’s thicker) than
White people’s skin.
9. Blacks, on average, have denser, stronger bones than Whites.
10. Blacks have a more sensitive sense of smell than Whites;
they can differentiate odors and detect faint smells better
than Whites.
11. Whites have more efficient respiratory systems than Blacks.
12. Black couples are significantly more fertile than White couples.
13. Whites are less likely to have a stroke than Blacks.
14. Blacks are better at detecting movement than Whites.
15. Blacks have stronger immune systems than Whites and are
less likely to contract colds.
(I’ll cover these questions in a future article.)
Here is the table showing the respondents’ answers to the questions:
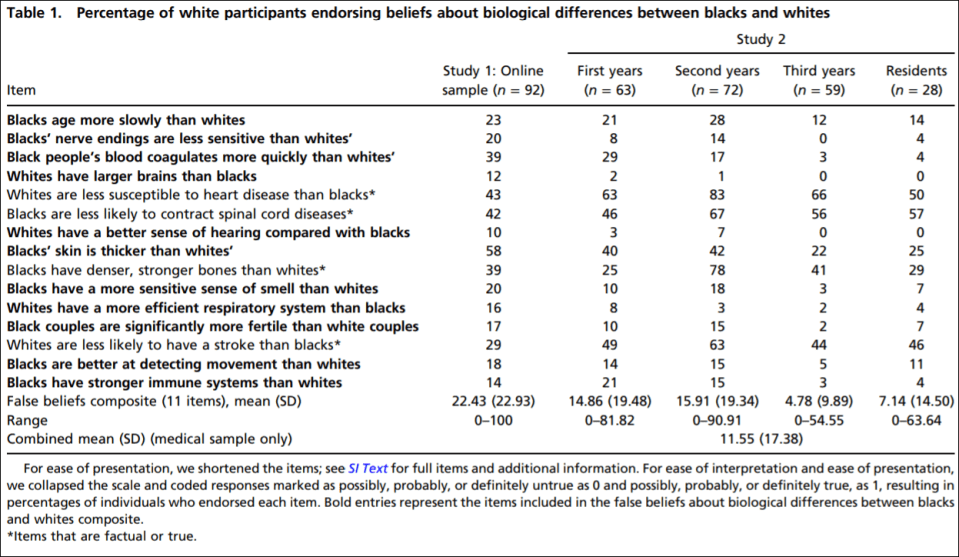
So they established that whites with no medical training hold false beliefs about black-white differences that then carry over to pain management. They showed in study 2 that medical students’ and residents’ apparently false beliefs about racial differences in the questions they answered showed bias in the accuracy of the recommended pain treatments. Hoffman et al (2016) conclude that:
The present work sheds light on a heretofore unexplored source of racial bias in pain assessment and treatment recommendations within a relevant population (i.e., medical students and residents), in a context where racial disparities are well documented (i.e., pain management). It demonstrates that beliefs about biological differences between blacks and whites—beliefs dating back to slavery—are associated with the perception that black people feel less pain than do white people and with inadequate treatment recommendations for black patients’ pain.
(See also the Psychology Today article on the matter.)
Similarly, Hollingshead et al (2016) reported that subjects, regardless of race, rated the white person more sensitive to pain and more likely to report pain than the black person. Whites reported that they were less pain sensitive and less likely to report pain than their peers. Blacks reported that they were more sensitive to pain while reporting more pain than their peers.
Interestingly, Trawalter, Hoffman, and Waytz (2012) state that black NFL players are more likely to play in a subsequent game than whites when injured, and that, as found in many other studies, blacks are more likely to feel less pain than whites. However, what the literature really shows is the opposite: blacks are more likely to feel pain than whites.
Kim et al (2017) showed that blacks, “Hispanics” and Asians had lower pain tolerance, higher pain ratings and greater temporal sensation of pain. They also showed that blacks had lower pain tolerance and higher pain ratings but no differences in pain threshold.
Blacks report greater pain regarding AIDs, glaucoma, migraine, headache, jaw pain, postoperative pain, joint pain and many other types of pain compared to whites (Green et al, 2003; Klonoff, 2009). Riley III et al’s (2002) results indicate that blacks show a stronger link between pain and emotions than whites. Obana and Davis (2016) showed that Native Hawaiian/Pacific Islander male and females reported higher pain scores than whites when it came to joint pain (but they were not significant). Bolen et al (2010) showed that work limitation, severe joint pain, and arthritis-attributable activity were higher for non-“Hispanic” blacks, “Hispanics” and multiracial people compared to non-“Hispanic” whites. Even American Indians, Alaskan natives, and Aboriginal Canadians had a higher prevalence of pain and pain symptoms than Americans (Jimenez et al, 2011).
Chan et al (2011) surveyed older Singaporeans. They found that Malay people had lower pain sensitivity compared to Chinese people, and that Indians reported greater pain sensitivity when compared with Malay and Chinese people. Australian women rated menstrual pain higher and lasting 36 percent longer than Chinese women (Zhu et al, 2010).
When it comes to potential mechanisms, physiological mechanisms are hypothesized by Campbell and Edwards (2012) who write:
For example, in comparison to non-Hispanic whites, African–Americans have reduced nociceptive flexion reflex thresholds [26]; the nociceptive flexion reflex is an electrophysiological, spinally mediated reflex, which is not amenable to voluntary control or subject to issues of response bias that plague self-report of pain experiences. This finding suggests that the observed ethnic differences in pain are unlikely to be fully explainable by sociocultural influences and hints that neurobiological processes may contribute to such differences.
Mossey (2011) shows that “Racial/ethnic minorities consistently receive less adequate treatment for acute and chronic pain than non-Hispanic whites, even after controlling for age, gender, and pain intensity.” Martinez et al (2014) showed that when it comes to colorectal and lung cancer, mixed-race individuals and blacks are more likely to report higher pain severity than whites. (Also see Shavers, Bakos, and Sheppard, 2010.)
All of the literature points in the opposite direction of the myths about pain sensitivity in regard to race: blacks feel more pain than whites and are more likely to have a lower pain tolerance. So the myths people hold about differences in pain between racial groups (mostly blacks and whites) are false. Pain is a subjective experience. And there will be differences in pain thresholds between individuals and racial groups and the causes may be both sociocultural and physiological in nature. However, this bias (in the wrong direction) speaks to what I wrote about last night: physician bias when it comes to blacks and other minorities.
Barr (2014: 183-184) writes:
Based to a certain extent on the attention given to his earlier publication, Todd moved to a faculty position with the Emory University School of Medicine, in Atlanta, Georgia. There he was able to essentially repeat his earlier study, this time examining persons coming tothe emergency room of a large, inner-city community hospital in Atlanta that was affiliated with Emory (Todd et al, 2000). He evaluated the medical records of 217 individuals coming to the emergency room over a 40-month period for treatment of an isolated long-bone fracture. Given the racial makeup of Atlanta, these included 127 blacks and 90 whites. They found that
- 54 of the blacks (43 percent) received no medication for pain during their treatment
- 23 of the whites (26 percent) received no medication for pain during their treatment
As with the earlier study in Los Angeles involving whites and Hispanics, in this study, the blacks were nearly twice as likely to receive no pain medication while in the emergency room. With this study, the authors were keenly aware of the importance of documenting the extent to which the patients expressed painful symptoms. By thoroughly reviewing the medical records of these patients, they found that 54 percent of blacks and 59 percent of whites had a notation in their medical record that they had expressed painful symptoms. The nearly twofold difference in withholding pain medication in blacks and whites was because the doctor didn’t order the medication, not because the patient didn’t want the medication.
This, again, speaks to physician bias when it comes to race in a medical context. Race is a useful tool in medicine, but to hold biases in the complete opposite direction that they exist in is wrong. This study—and many others—speak to the type of bias that physicians have against minorities in a medical context. Understanding that the differences in pain are actually the opposite from what is commonly believed by both laypeople and medical doctors is important: if blacks feel more pain than whites regarding the same injuries and they are not getting the care needed, then this speaks to physician bias. What Barr showed was that blacks were treated at the emergency room based on their ethnicity. This is wrong. Race/ethnicity is a useful tool in medicine, but to outright use it as an assumption for numerous factors makes no sense and could cause more harm than good.
Using race in a medical context is a good thing. But using race in a medical context using essentialist, outdated views about race is wrong and can lead to many horrible outcomes. Of course, using race in this context can and does lead to certain things being discovered over others. For instance, if one’s race is assumed to be “driving” one’s illness (i.e., that one has a disease that that race/ethny is more likely to have), then race can and is a good marker to use—specifically geographic ancestry. However, when it comes to things like pain management, this obviously leads to false ideas about how different groups manage and feel pain.
Views about racial differences in pain affect both laypeople and medical doctors. These views can be and are harmful. The literature points to the case being the opposite of what is believed by people: blacks have lower pain tolerance and higher pain ratings than whites. These types of differences are also found between many other races and ethnic groups. The causes could be both sociocultural and physiological. A person’s response to pain depends on their unique physiology, life experiences, ethnicity and other factors. Understanding how and why physicians are biased toward how blacks feel pain is important, along with addressing the other biases that they have about other minorities when it comes to a medical context. Race and ethnicity are important tools for medicine, but these are some of the ways that the concepts can be used with nothing good coming out of it.
Health by State and Racial Discrimination by Physicians
3000 words
I’m currently reading Health Disparities in the United States: Social Class, Race, Ethnicity and Health by medical doctor and sociologist Donald Barr. In the book, he chronicles differences in health between races and ethnies, talks about the concepts of race used and cites well-known studies to people who read this blog, and he also shows that doctors are—either conscious or not—biased against minorities in certain medical contexts.
In Chapter 1 discusses the fact that, although Americans spend the most money on health care, Americans have a lower life expectancy and higher infant mortality rate than all other developed countries, showing the association in social inequality and health across all income levels and education. In Chapter 2, he asks the question “What is health?”, discussing many concepts of what “health” is. In Chapter 3, he defines “socioeconomic status” and shows the link between poor health and poor SES. In Chapter 4, he discusses the link between inequality and poor health, introducing the concept of “allostatic load”, which is the physiologic response to being in a spot of social disadvantage.
In Chapter 5, he looks at different race concepts, since it is a main premise of the book. In Chapter 6, he shows that minorities are more likely to be in a position of low SES. He asks, if minorities of the same SES as whites are consistently found to be of lower health than whites of the same SES, is it because those with poor health tend to be minorities, that they tend to have lower SES or both? In Chapter 7, he asks the same questions while focusing on children. In Chapter 8, he examines disparities in access to healthcare, showing that even when minorities have the same insurance and doctors that minorities still face worse health outcomes (he shows that they either do not receive appropriate healthcare or receive lower-quality care). In Chapter 9, he shows that physicians treat blacks and other minorities differently, albeit unconsciously. In Chapter 10, he discusses when—if ever—a physician would be justified in using racial/ethnic categories. And in Chapter 11, he states that not all of these disparities need to be eliminated.
In Chapter 2, Barr (2014: 45) presents this table, showing rates of illness and selective rates of death between States in America. Obviously, the one to look at that is different than the others is Mississippi. Mississippi is 37.5% black. 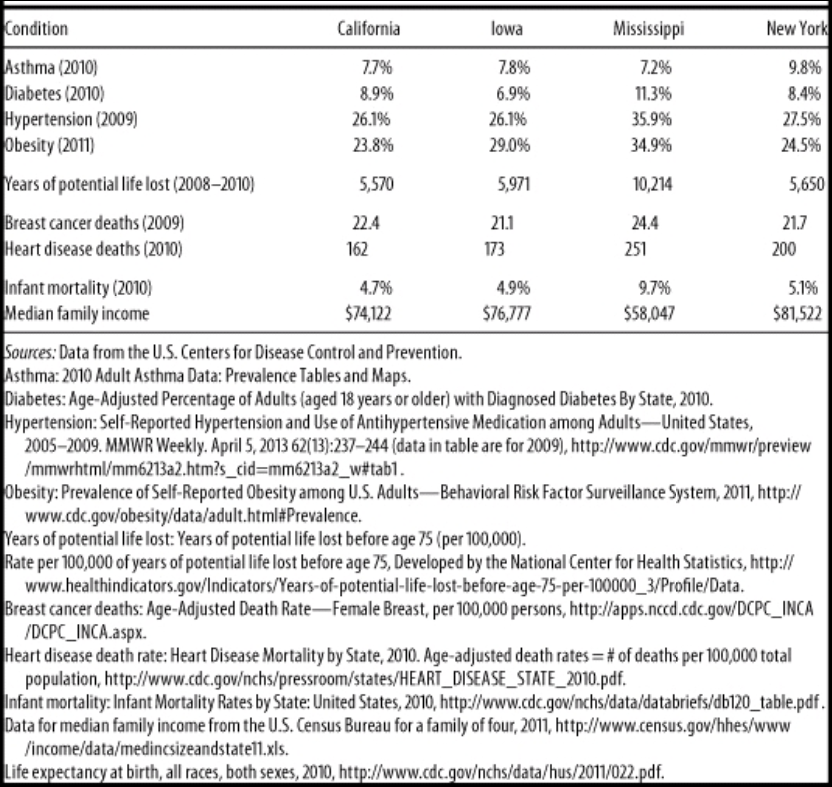
Wow, I wonder why Mississippi has such a high rate of obesity, diabetes, and hypertension (high blood pressure). Must be all of those obesity, diabetes and hypertension genes (HBDer).
Obesity and diabetes
The first thing to look at is median income. It is substantially lower in Mississippi compared to California, Iowa, and New York. About 23 million people in America live one mile from a supermarket, while black Americans are about half as likely to have access to supermarkets while “Hispanics” are about a third likely to have access to them (New York Law School Racial Justice Project, 2012). So when it comes to those who have to travel more than a mile for fresh fruit and vegetables, they have poorer health (Stack, 2015). So combine lower median income, along with food deserts and one can start to see how minorities have poorer health due in part to their SES. In short, living in a food desert can affect public health.
Blacks are the most obese ethnic group in America, and this relationship is largely driven by black women. Now, it’s not weird that women have higher levels of body fat than men, since women it is needed for physiological functioning. Though, there is something weird here: Black American men with more African ancestry are less likely to be obese (Klimentidis et al, 2016). Since black women and black men in America are in the same economic bracket, there must be something in the West African male physiology that “protects” them against central adiposity, though variation in social, environmental and cultural factors may play a role as well. In any case, the more West African ancestry American blacks have, the less likely they are to be obese. Klimentidis et al’s (2016) study “suggests that there are specific genetic variants and physiological mechanism(s) that differ among West African and European populations.”
Obesity affects more ethnies in America than others: non-Hispanic blacks and “Hispanics” are more likely to be obese than non-“Hispanic” whites and Asians (Hales et al, 2017). This could be due to, in part, to the variation in supermarket access and access to good foods—the concept of food deserts. Look at any low-income area near you. You’ll see a majority of corner stores with cheap, garbage food. The lack of ability to buy good food (along with the education to know what to buy and when to buy it) can explain differences in obesity rates—obviously not all. Obesity is related with diabetes, and sinec the relationship is so strong, the term “diabesity” was coined.
Eating cheap, processed carbohydrates spikes insulin. Repeated insulin spikes over time leads to type II diabetes and, eventually, obesity too. One can be skinny and have diabetes (a phenomenon known as thin on the outside, fat on the inside “TOFI”). However, since both diseases are co-morbid, we need to look at them in similar contexts. The higher rates of obesity can help to explain the higher rates of diabetes and hypertension—since those who are obese have higher blood pressure (Aronow, 2017).
Minorities are more likely to develop type II diabetes (Tuchman, 2011), and the cause of this is access to high-quality foods. But racial differences in obeisty and SES do not fully explain the higher rates of type II diabetes in black Americans; being a black American is a strong, independent factor for developing type II diabetes and this is compounded by low SES (Brancati et al, 1996). Zizi et al (2016) showed that both long and short black sleepers have an increased risk of developing type II diabetes. There are racial differences in sleep, with blacks having higher durations of long and short sleep compared to whites (Adenekan et al, 2013).
Hypertension
Now let’s look at hypertension (blood pressure). Blood pressure is a physiological variable. Since it is a physiological variable, it can and does respond to social/environmental contexts. So blood pressure can be affected by social contexts, too. For example, Williams (1992) cites stress, socioecologic stress, social support, coping patterns, health behavior, sodium and more for reasons why blacks have higher BP than whites. Dressler (1991) shows that the struggle to maintain a middle-class lifestyle is related to higher levels of BP. Similarly, Keith and Herring (1991) show that skin color is a strong predictor of occupational status and that darker-skinned blacks in America are twice as likely to experience racial discrimination than lighter-skinned blacks. This, too, can help to account for higher levels of BP between the races. In any case, Williams (1992) shows, definitively, that the causes of black-white differences in BP lie in the social environment.
Similarly, Non, Gravlee, and Mulligan (2012) show that racial disparities in BP are explained by education, and not genetic ancestry. They show that the association between BP and education was much stronger for blacks than for whites. Their results also support “the minority poverty hypothesis because the worst blood pressures were predicted for people who faced the double burden of being less educated and identifying as African American.” People who face discrimination could, and do, have higher levels of BP due to the stress they feel due to the discrimination. (Note that I take no sides on whether the discrimination is real or imagined, because even if it were imagined, it still leads to real physiologic consequences.)
Do note that there is a just-so story to explain how and why blacks have higher levels of blood pressure than whites: The Slavery Hypertension Hypothesis (Lujan and Dicarlo, 2018). This has all of the hallmarks of a just-so story posited by evolutionary psychologists. The story goes like this: Black slaves who were on the way to America in the Middle Passage had genes that favored better salt retention. So it is noted that black Americans have higher rates of BP than whites, and then they work backward and attempt to posit the best story possible to explain the current-day observation. This is the usual method evolutionary psychologists use—the method of reverse engineering, the inference from function to cause. So (1) note that blacks have higher levels of BP than whites; (2) infer the function to cause (blacks with genes that favored salt retention were more likely to survive; so (3) this is why blacks have higher rates of BP than whites. Though the explanation fails, since education, and not genetic ancestry, explains the difference in BP between blacks and whites (Non, Gravlee, and Mulligan, 2012). One only needs to understand the intricacies of physiology and how our physiological systems respond to what occurs in the greater environment.
So, obesity can explain both the higher rates of diabetes and higher rates of blood pressure, with differences in the immediate social environment explaining the rest of the differences in blood pressure between blacks and whites. (Note that heart disease deaths are directly related to hypertension. Heart disease affects blacks more than whites.)
Breast cancer
In Race, Medicine, and Epigenetics: How the Social Becomes Biological, I shortly discussed breast cancer in black women:
Black women are more likely to die from breast cancer, for example, and racism seems like it can explain a lot of it. They have less access to screening, treatment, care, they receive delays in diagnoses, along with lower-quality treatment than white women. But “implicit racial bias and institutional racism probably play an important role in the explanation of this difficult treatment” (Hardimon, 2017: 166). Furthermore, black women are more than twice as likely to acquire a type of breast cancer called “triple negative” breast cancer (Stark et al, 2010; Howlader et al, 2014; Kohler et al, 2015; DeSantis et al, 2019). Of course, this could be a relevant race-related genetic difference in disease.
Infant mortality
Now note the infant mortality rate between the states: the infant mortality rate in Mississippi is 9.7%. Smith et al (2018) show that black women are at a higher rate of having their infant die at birth. Pre-term births are related to low birth weights, and they both are related to infant mortality. Matoba and Collins (2017) write:
In the United States, African-American infants have significantly worse infant mortality than white infants. Individual risk factors alone do not explain this persistent gap, just as they did not explain the disparity in preterm birth and low birth weight. Recent studies in social determinants provide insight into the contribution of community and environmental factors to the racial disparity. Select community-level factors are potential, but partial, determinants of the racial disparity. Interpersonal and institutionalized racism is an important, and increasingly recognized, stressor for African-American women with damaging consequences to maternal and child health.
The Guardian ran a recent story on infant mortality and race, positing racism as a cause of the disparity. In any case, the social environment can and does play a part in everything discussed here today since the social can and does become biological. Part of the reason why Mississippi has a way higher rate of years of potential life lost (10,214 compared to 5500-5900 for Iowa, New York, and California) is that rates of infant mortality are higher in Mississippi. So the median age of death is 75. If an infant dies at one year of age, then that is 74 years of life lost. Therefore it is not surprising that the State with the highest level of infant mortalities has a higher number of years of potential life lost. Further, one 2017 review found that segregation was associated with increased risk of preterm birth and low birth weight for blacks (Mehra, Boyd, and Ickovis, 2017)
Note how Mississippi has lower rates of asthma. This is explained by the fact that Mississippi is more rural than, say New York. Rates of asthma are associated with living in a metropolitan area (Frazier et al, 2012; Malik, Kumar, and Frieri, 2012). (Note that blacks and other races have higher rates of asthma than other races.)
Physician bias
The lower one’s position is on the social hierarchy the lower their probability of staying healthy and having a high life expectancy; when people have the same type of health insurance and are treated for the same disease in the same hospital by the same doctor, that minority groups get worse health care, either not receiving it or receiving lower standards of quality in care. What could account for such disparities? I asked PumpkinPerson the question, and he said:
1) EGI: Doctors put more effort into saving coethnics: she looks like my italian grandma. I’ll make sure she gets the best medicine.
2) IQ: low IQ populations don’t understand the doctor’s advice and damage their health
3) r/K: some populations have faster life history so don’t live as long, even with good medical care
If (1), then the doctors need to be named, shamed, and have their medical licenses revoked. If (2), then they need better education (since IQ is just an index of middle-class knowledge). (3) is completely irrelevant, since it doesn’t make sense for humans and the concept is long-dead in ecology. In any case, PumpkinPerson danced around the true cause: differences in healthcare brought about by unconscious bias (of which (1) may be a cause). But positing (1) as a cause completely misses the point (and is the usual HBDer reductionism to genes causing most/if not all things). It’s the usual HBD/Rushtonian reductionism to genes. That’s all the HBD worldview reduces to: genes/IQ.
In any case, Reschovsky and O’Malley (2008: 229, 230)
Our results indicate that the minority makeup of physicians’ patient panels is associated with greater reports from physicians of difficulties providing high-quality care. At least some of this relationship appears to be explained by the lower resources flowing to high-minority practices.
The results of this study suggest that racial and ethnic disparities in primary health care are in part systemic in nature, and the lower resources flowing to physicians treating more minority patients are a contributing factor.
Thus, bias—whether conscious or unconscious—by physicians can explain how and why there are differences in health outcomes between people that have the same health insurance and doctor. Barr (2014: 168) states that “for black Americans, where a person lives sems to be associated with access to primary care, the quality of available hospital care, and the quality of available home care.” Barr shows that blacks receive a different level of care for a wide-range of diseases and illnesses compared to whites. For instance, Smedley et al (2003) write that “some evidence suggests that bias, prejudice, and stereotyping on the part of healthcare providers may contribute to differences in care.” Quite clearly, there is racial bias against minorities and it does seem to affect healthcare, whether or not it is intended or unintended (conscious or unconscious) (Williams and Rucker, 2000). Bird and Clinton (2001: 255) write:
Race and class-based structuring of the U.S. health delivery system has combined with other factors, including physicians’ attitudes—perhaps legacies conditioned by their participation in slavery and creation of the scientific myth of black biological and intellectual inferiority—to create a medical-social, health system cultural, and health delivery environment which contributes to the propagation of racial health disparities, and, ultimately, the health system’s race and class dilemma.
Blacks are more likely to take the advice of physicians, and to use the needed services, such as preventative care and are less likely to delay seeking care when the physician is of their own race (Saha et al, 2000; LaVeist, Nuru-Jeter, and Jones, 2008).
Blacks are more likely to perceive racism in healthcare and when they are able to choose their own doctors, they are more satisfied with their level of care (Chen et al, 2005). Chapman, Kaatz, and Carnes (2013) show that increasing awareness of implicit bias in healthcare can lower such disparities, stating that having more black doctors will alleviate such problems since they are less likely to be biased. Having a black doctor lead to more effective care for black men. Quite clearly, the race of the doctor matters for implicit biases and minority doctors lead to more effective healthcare for minorities, since they are less likely to be affected by racial biases. Minorities trust the healthcare system less than whites (Boulware et al, 2003). Black and white physicians even agree that race is a medically relevant data point, but do not agree on why (Bonham et al, 2009).
Conclusion
The table presented by Barr is telling. He purported to show that on certain indices of health, certain states fair worse than others. Rates of illness and rates of death between different states (with differing ethnic compositions) were compared. Using national data, he showed that Mississippi has the highest rates of death and illness (sans asthma). Social factors can and do account for the differences in hypertension between blacks and whites (and States); food deserts (lack of access to good food) can explain higher rates of obesity and diabetes and also higher rates of blood pressure between the races (and States with a higher percentage of certain racial/ethnic groups). Of course, physiological variables are affected by the social environment, so we have to look at differences in the social environment between groups to see how and why there are differences in any physiological variable we look at.
Doctors, whether consciously or not, treat minority patients differently and there is evidence that this leads to differences in health outcomes between ethnic groups in America. PP’s hypotheses don’t cut it (the only one that does it his “EGIs”, but that explanation fails; the cause is bias by the doctors but “EGIs” have nothing to do with the bias). In any case, there are social and cultural reasons why there are such health disparities between States and races/ethnies. Understanding the causes behind them can and will lead to closing the gap between them. The social can and does become biological, and this is the perfect way to show this. There are ways to lower the disparities in a medical context, and education seems to be one of them—for both patient and doctor.
Some states are healthier than others based on objective measures of health and mortality, and understanding the reasons why can and will decrease these differences.
Black and White Skin
1750 words
Skin color is the first thing you see when you see someone. Skin color has many uses, and the color of one’s skin can give you a general idea of the type of climate one’s ancestors evolved in. The lighter one’s skin is may tell you that their ancestors evolved in low UVB radiation, whereas the darker one’s skin is may tell you that their ancestors evolved in high UVB places. So this tells us that as migration occurred out of Africa, skin needed to lighten in order to synthesize vitamin D in low UVB climes. Note that I won’t make any claims about any skin color being an adaptation to any climate; I will just state that there is a strong association between UVB and skin color—the higher the UVB the darker the skin and the lower the UVB the lighter the skin.
The skin comprises about 16 percent of the human body, making it the body’s largest organ (D’Orazio et al, 2013). There are two layers to the skin, the dermis and epidermis. The outermost layer of skin—the epidermis—is the point of contact with the environment. So since this is the case, then the number of UVB rays in any given environment will dictate the color of one’s skin—in an ancestral manner.
So the most important factor in skin color is melanin, which is produced by melanocytes, but it accumulates in the keratinocytes of the stratum basale (the deepest layer of the five layers of the epidermis) and the stratum spinosum (the layer between the stratum granulosum and the stratum basale). Two forms of melanin exist: eumelanin (which is brownish black) and pheomelanin (which is reddish-yellow and contains sulfur).
In his textbook Anatomy and Physiology: The Unity of Form and Function, professor Ken Saladin writes:
People of different skin colors have essentially the same number of melanocytes, but in dark-skinned people, the melanocytes produce greater quantities of melanin, the melanin granules in the keratanocytes are more spread out than tightly clumped, and the melanin breaks down more slowly. Thus, melanized cells may be seen throughout the epidermis, from stratum basale to stratum corneum. In light-skinned people, the melanin is clumped near the keratinocyte nucleus, so it imparts less color to the cells. It also breaks down more rapidly, so little of it is seen beyond the stratum basale, if even there.
The amount of melanin in the skin also varies with exposure to ultraviolet (UV) rays of sunlight, which stimulates melanin synthesis and darken the skin. A sun-tan fades as melanin is degraded in older keratinocytes and as the keratinocytes migrate to the surface and exfoliate. (Saladin, 2010: 194)
Skin color is one of the most significant factors involved in colonizing a certain, new, area where the skin color the group has is not conducive to life in that clime. So, when the out of Africa migration occurred, skin color needed to lighten as to better confer survival in the new, colder climes. Though, there is an anomaly: Arctic peoples. Why is their skin dark—at least relative to other peoples who live or have lived in colder climates?
Think about life in the Arctic. It is pretty much all white. Food is scarce, and they eat a lot of animal fat and protein. Now, think about the ice. The ice reflects UV rays onto the skin of the Arctic people, making it not as light as, say, Europeans and East Asians.
A term I’ve heard a lot over the years is “Black don’t crack”, speaking to the fact that a lot of black people look young, even into old age. What, if any, is the physiologic reason behind this? For instance, Vashi, Maymone, and Kundu (2016) write:
Individuals with darker skin are overall thought to have firmer and smoother skin than individuals with lighter skin of the same age
Rawlings (2006) states that “Caucasians have an earlier onset and greater skin wrinkling and sagging signs than other skin types and in general increased pigmentary problems are seen in skin of colour although one large study reported that East Asians living in the U.S.A. had the least pigment spots.” Blacks have more corneosome layers than whites (21.8 cell layers compared to 16.7 cell layers). There is no difference in skin thickness between whites and blacks, so black skin is thought to be more compact with greater intercellular cohesion (see also La Ruche and Cesarini, 1992). Take transepidermal water loss (TEWL)—the total amount of water vapor lost through the skin and other appendages through non-sweating conditions. Since the Asian corneum is thinner, it takes fewer tape strippings to decrease TEWL compared to blacks who take more tape strippings, while whites are in the middle. (Though some studies note no difference).
Rawlins (2006: 85) notes that Sugino, Imokawa, and Maibach (1993) state that TEWL is greater in the order of Blacks > Caucasians > Hispanics > Asians.
So why does it seem that blacks, on average, age less than whites in the fact? I can think of one main thing: Their darker skin protects them from the effects of photoaging due to the melanocytes their skin produces. The opposite holds for whites—white skin produces fewer melanocytes and therefore is less protected against UV rays from the sun. Therefore lighter ethnic groups are more likely to have damaged skin compared to darker ethnic groups, and the main driver of this is the number of melanocytes produced by the skin. Rawlings (2006: 87) even writes that “Overall I would expect less signs of aging, i.e. maintenance of skin elasticity in darker skinned individuals [Negroids are reported to have an intrinsic sun protection factor (SPF) value of approximately 13].”
Rawlings also writes (pg 89):
In African Americans photoaging appears primarily in lighter complexioned individuals and usually does not appear until the late fifth or sixth decade of life.
There is another factor when it comes to skin: sweat glans. I have covered in the past the fact that Asians have fewer apocrine sweat glands than whites and blacks, while blacks produce more chloride in their sweat compared to whites. Prokop-Prigge et al (2017) state “that an individual’s ethnicity has a significant impact on human axillary odor production.” Blacks also have around 70 percent more lipids in their hair, while having larger sebaceous glands than whites.
So skin color dictates numerous changes in the skin which are associated with aging. Skin aging is associated with lighter-skin, whereas hyperpigmentation is associated with darker skin. Asians have lower TEWL, highest water content, and highest skin color lipid levels while the opposite is seen for blacks. Blacks have greater gland pore size, and increased apocrine and apoeccrine sweat glands along with greater sebum excretion. White skin has an earlier onset of aging, skin wrinkling and loss of elasticity. So there are differences in ethnic skin color and structure and function, and this causes the differences we notice between ethnies and how they age.
Campiche et al (2019) write:
There is differential manifestation of aging signs in different ethnic groups.
[…]
Our results show that Africans from the African continent show delayed signs of aging compared to Caucasians.
They found no differences in forehead wrinkles between Caucasians and Africans, though there was a difference in depth of forehead wrinkles. Blacks showed less advanced crow’s feet than whites, while also having less depth. There were no differences in mouth frown lines with the exception of depth and wrinkle surface and volume parameter, of which there was an increase in Caucasian subjects compared to African subjects. Though when it comes to the length, surface and vertical lines in African subjects they showed more advanced aging but there was no difference in depth between the races. Caucasians had bigger nasiolabial folds (smile or laugh lines) than Africans, regarding length, surface, depth and volume. Africans had deeper pores than Caucasians. Africans had a greater homogeneity than Caucasians when it came to skin color. (Note that the cohorts came from France and Mauritius.)
Campiche et al (2019: 12) write:
This is also in line with the fact that photoaging in African Americans does not appear until the late fifth or sixth decade of life.22 This may explain why aging in our Black African cohort from Mauritius is less pronounced than in the Caucasian cohort although the Black African cohort is older.
[…]
The difference in age between our Caucasian and Black African cohorts (median age 46 years vs 56 years) could bring into question the comparisons of the two cohorts. Nevertheless, we mostly found that Caucasians displayed more severe signs of aging than Black Africans which is in line with the common understanding that the onset of aging in fair skin starts earlier than in darkly pigmented skin and that there were differences in the appearance of lip lines and facial pores.
So differences between the two ethnic groups come down to facial site, and measurement parameter. This study further buttresses the point that, at least when it comes to certain ethnic groups, whites age faster than blacks—even when the whites are younger than blacks (46 compared to 56 years, respectively).
When it comes to skin color and desirability, though, we see something else: light skin being prized, whereas dark skin is shunned. Jablonski (2010: 188) writes:
As we have seen, for much of recent history and around the world, pale skin has been prized to such a degree that people have been willing to risk illness and disfugurement to obtain it.
[and also on pg 177]
Preferences for light skin have arisen independently in many cultures, and they have been reinforced when different “cultures of lightness” have come into contact. Because having lighter skin has often been associated with higher social status, success, and happiness, people over the ages have sought to become lighter by various means.
I won’t ruminate on the causes of this, I just wanted to make a note of it at the end of this piece on black and white skin color.
In sum, there are many interesting differences between black and white—and even Asian—skin. Better understanding of these kinds of differences will lead to better skin care for all races, and dermatologists can then use that information to give better case based on race/ethnicity/skin color to a certain individual. We know what causes differences in skin color between individuals and groups—melanocytes. We also know that skin color and UVB radiation are strongly related. We know that there are numerous differences in skin biology when comparing different peoples whose ancestors have evolved in different climates. So understanding these differences can and will lead to better healthcare for all populations.
Watching from the Sidelines: More Thoughts on That High-School Running Competiton
2750 words
Two months ago, I wrote about the two transgender high-school athletes in Connecticut that competed in the in-door running competition. Of course, the two top-placers were the ones who went through male puberty. There is a short interview involving some of the competitors in that specific competition. One of the girls shows her face—the others do not, because they fear the repercussions of discussing this. They are scared of airing their grievances due to “the far left” as one of them says. And this is a completely rational thing to do, especially if they are attempting to make track a career and compete in college.
In any case, the one girl—Selina Soule—who does show her face in the interview levels some solid points. (The quotes are from Selena and they come from 8th Place: A High School Girl’s Life After Transgender Students Joined Her Sport.)
“When I’m at the start of the race, when I’m lining up and getting into my blocks, everyone already knows the outcome. Those two athletes are going to come one and two, and everyone knows it.”
Now, think back to what I wrote about the two individuals who took first and second place. You can see in the pictures from the competition that they have extremely narrow bodies—specifically narrow hips—compared to the actual female competitors. In the previous article on this matter, I discussed numerous variables that men have that are more conducive to success in running sports. Such as larger stroke volumes, smaller Q-angle, and larger hearts. Testosterone stimulates red blood cell production. This is important during exercise, since the more blood that can get to the muscle means that the muscle can work harder.
Sprinting is a full-body sport—each part of the body needs to work in harmony. So, if the whole of the system of individual A is better than B, then A will most likely win. Take A to be a transgender runner who went through puberty and “presents” as a “girl.” Take B to be a normal girl who went through a female puberty. They were exposed to differing levels of steroid hormones (estrogen is a steroid, too—the main differentiator between men and women). So, even if A takes hormones, A STILL had the physiological and anatomic advantages from going through male puberty.
So, to take the girl’s point that “everyone already knows the outcome”, this is on its face already true. In a competition like this, one can get a general idea on the results of the event by looking at the somatotype differences between the girls. Of course, some girls have a narrower frame than others—but the thing is is that they were not exposed to a male puberty, and so, while they do have certain (natural) advantages over other girls, they do not have the main advantage that these transgender runners had.
“No one thinks it’s fair, because we all know that males are physically stronger than females and they compete at a higher level.”
Men have 63 percent more muscle mass than women, which is related to their higher levels of exposure to testosterone both developmentally (in the womb) and during puberty. Most of this muscle mass is located in the upper-body, with men having around 75 percent more arm muscle mass than women. This difference then translates to about a 90 percent higher upper body strength in men over women. Sex also explains about 70 percent of the variance in muscle mass and upper body strength in humans. Men have 50 percent greater muscle mass than women and their lower body strength is about 65 percent greater (see Lassek and Gaulin, 2009).
Let’s get back to development and puberty. If testosterone explains a lot about why men have more muscle mass than women, and muscle mass is conducive to success in sport (in this instance, running), then if an individual is exposed to higher levels of testosterone during development and at puberty—along with the conducive somatotype that is involved with success in the sport—then they will necessarily be better. Even a transgender athlete that has “transitioned” or “presents as” a girl/woman WILL necessarily be stronger than any girl/woman who did not, on average, since they were exposed to way more of the hormone testosterone then they were.
Here’s the most ridiculous part about this. Back in March, House Speaker Nancy Pelosi passed the Equality Act. Now, of course, individuals should not be discriminated against, that is wrong. The relevant part about this, though, is that this Act can make it so that transgender athletes can just “declare to be” female without any evidence of any changes to their bodies. (And, I have argued at length that, even if they did go through such “changes” that they would still have inherent, unfair, advantages over bio-women).
This will mark the end of women sports if ONLY one’s gender identity is the basis for who they will compete with—there will be men’s sports and unisex sports, and if that is to be the case, then I feel that most girls would just stop competing.
“It’s giving the transgender females the right to compete with biological females and eventually it’s going to get to the point where the biological females will be on the sidelines, watching their own sports.”
“It’s very frustrating and hearbreaking when us girls are at the start of the race, and we already know these athletes are going to come out and win no matter how hard we try.”
This is the biggest problem of all. With the creation of the Equality Act, we can imagine this scenario. Individual A (a male) competing in competition C does not do well. They then change their gender identity to compete in women’s sport. They will then blow away the competition. How is that fair? If you were a girl who competed in, say, track, and you saw someone who you knew would win even before the starting gun, what would that do to your will to compete? What would that do to your confidence?
Now, I can already here trans-activists say “Just try harder! Train harder!” Statements like that are jokes. No matter how hard they train, no matter if they give it their all to win, the transgender females will just decimate them.
“My freshman year in outdoor, I saw at the 200 start, this girl who looked kind of masculine. Her arms were much more defined than the average girl’s, and same with her legs, but she had long hair, long braider hair, and I didn’t think much of it. And then I watched the race, and I saw that this girl was blowing away the competitors, and I thought, “Hey, this isn’t right. This usually doesn’t happen.” And then later, in that same meet, I found out that athlete was a transgender female.”
How the hell is this in any way, shape, or form, fair? Quite clearly, just by looking at this person’s anatomy—arms that “were much more defined than the average girls, and same with her legs”—we can make a very solid educated guess on what will go down at this competition. I want to know what is going through the minds of these athletic directors who allow this sort of thing. What are they thinking by allowing it? Do they not realize that they are—with others—setting a precedent to change girl’s and women’s sport forever?
“And then in outdoor last year, there was another transgender that came out and she competed as a male for three seasons, and was mediocre as a male. And then ended up transitioning over to female, and, again, blew everyone out of the competition.”
And there we have it: Any male who is mediocre can then “declare his gender to be” female and then compete with the females and then have way better standing in the competition that he is now competing in. Can’t cut it in the male event? Just say you’re a woman! (Think the movie Juwanna Mann.) That’s like me being a mediocre lifter, and then declaring my gender to be female so I can compete with the women and then I blow away the competition. Is that fair? No, it’s not.
Soul’s mother brought up a very good point: Selena placed 8th in State final, and the first two spots were taken by two “boys who identify as girls”. If those two competitors did not compete, then Selena could have more than likely taken the 6th spot and went on to the New England Championships. When it comes to high-school sport, this is really ridiculous. They are screwing girls who could get good scholarships and looks from scouts from different Universities around the country.
“No one thinks it’s fair, but everyone is afraid of retaliation from the media, from kids around their school, from other athletes, coaches, school administrators. They dont want to attract attention to themselves, and they don’t want to be seen as a target for potential bullying and threats.”
Of course, if the girls who were anonymously interviewed by The Daily Signal identified themselves, they could be screwing up future chances and their current relationships. The fact that Selena is doing this out in the open shows her courage and her will to fight for what she—and rational people—believes is right. Here is what the anonymous girls said:
Girl 1: “Watching them run was just heartbreaking. I mean, you almost don’t even want to watch, but how can you not? You can clearly see these two biological guys just absolutely crushing it and it almost brings you to tears.”
Girl 2: “We’ve competed head to head with these people many times, and it hurts to see them win when you know that you probably should’ve won.”
Girl 3: “There’s really nothing else you can do except get super frustrated and roll your eyes because it’s really hard to even come out and talk in public just because of the way with the far left and how immediately you’ll just be shut down. We are totally accepting of who they are and who they want to be. We just have an issue when it comes to sports.”
Each girl brings up a great point: (1) It would make one not want to watch AND not want to compete because they know that their attempts at winning are futile. (2) Girl 2 said that they’ve competed against them many times, and, of course, they have won. What would it due to one’s confidence knowing that there are individuals there with such unfair advantages? Yes, I know that the other day I said that sport is all about watching people with inherent advantages—watching the best-of-the-best. However, there is a difference here: The best-of-the-best when it comes to men and women are two completely different things. For, if this is the case, why not just eradicated women’s sport all together? (3) Makes perhaps the best point of all. One cannot come out and air their grievances because “the far left” as so succinctly stated by girl 3 would shut you down without even hearing what they would have to say and their feelings on the matter.
“With the case in Connecticut, it can be difficult showcasing my talents to coaches from around the country, as they only look at the results online. They see the first and/or second place girl so far ahead of the rest of the girls. And they’re going to reach out to and try to recruit those two top giels versus everyone else, since they’re so far behind in time.”
This is the most ridiculous part of this whole fiasco. Selena makes a good point that since recruiters only look at results online, that they will see the disparity between the top two placers and the others and only go to speak to the top two. For example, Miller’s (one of the transgender athletes) time in the 55 m dash was 6.96 seconds; Yearwood’s time was 7.01 seconds (the other transgender athlete); and the third place winner’s—a biological female—time was 7.23 seconds. A coach looking at this time online will not even look at the third placer and will only look at the top two—biological males. I wonder if those who allow these types of things in high-school sport truly understand what they are doing. I wonder if they truly understand that they are possibly screwing the careers of some of these girls since they may get overlooked by scouts.
I think it’s gotten to the point where some girls are starting to stray away from those events, and are hoping to go to other events, so then they actually have a fair chance of winning. In my case, I have my field event, long jump. That was my safe haven, if you want to call it, where the results were fair no matter what because it was girls competing against girls. But now, unfortunately, one of those [transgender] athletes has started to compete in long jump, so now none of my events are safe. It’s frustrating when you know that you run your best, and no matter what, your best is never going to be enough.
So even Selena’s other event is getting taken over now. Where will it end? Will we see the de facto elimination of girl’s sport throughout the country one day? Will it be men’s sport and co-ed sport eventually (with of course bio-males taking the top spots)? Take the long jump. Men have a larger abundance of type II (fast twitch) muscle fibers than women who have an abundance of type I (slow twitch) fibers. If Selena is now competing against bio-males, and muscle fiber typing DOES NOT CHANGE, then, of course, there is another unfair advantage that these competitors have since they went through male development and puberty. The same point on muscle fiber typing can then be made in regard to the 100 and 200 m competitions as well. No matter how hard they try or train, what they do will never be enough. How is that fair?
For these girls and others to feel better about this fiasco, they should—in their minds—know that the true competition was between the 3rd place and lower, even though it will not fix the problem that they will be overlooked by scouts since their times are so disparate compared to that of the “winners.” When will this be put to an end? When women are on the sidelines watching what is supposed to be their sport while they watch a slew of men who identify as females take over their sports? Will we eventually have co-ed sports and male sports with the de facto elimination of women’s sport that the Equality Act will put into effect? These types of questions are best answered by sport ethicists and philosophers of sport (I will discuss them in the future), and I, personally, await what some of them have to say about matters like this and similar ones.
I can, of course, see trans-activists clamoring about how “bigoted” and “trans-misogynist” that Selena and her teammates are being. That is irrelevant. They are airing their grievances about how they feel about their sport being taken over by boys—no matter if they “identify as” girls or not. For if girls do not speak out about this now, then they will eventually lose their sport and women’s sport will become co-ed sport—effectively eliminating women’s sporting events. Is that what people would truly want in the name of “equality”? Wouldn’t true “equality” be having separate events for trans-athletes? What about Kerr and Obel’s (2017) argument that sport should be segregated by attributes conducive to success in that sport? I think that’s a route that can and should be tried—and girls like Selena would then still get to have fair competitions.
However, as of today, it is complete bullshit that these girls are competing with boys and people look at it as OK. It is bullshit that the three girls had to conceal their identities because they fear repercussions from their classmates, teammates, and administrators. Selena is brave for airing her grievances publicly and putting her name and face out there on issues she feels strongly about. I hope all goes well for her in the future and that scouts will eventually look at her, and not the two blowing away the competition. Is it any surprise when men have so many physiologic and anatomic advantages over women (see Lassek and Gaulin, 2009 for muscle and strength differences)?
If nothing is changed, girls will be watching their own events from the sidelines.
Usain Bolt, Michael Phelps, and Caster Semenya: Should Semenya Take Drugs to Decrease Testosterone Levels?
1300 words
In the past week in the world of sport, all the rage has been over mid- to long-distance runner Caster Semenya. Semenya has won the 800 m in 1:56.72 and setting world records in the 400, 800, and 1500 m with times of 50.74, 1:58.45 and 4:10.93 respectively. In 2012 and 2016, Semenya won the gold for the 800 m with times of 1:57.23 and 1:55.28 respectively. I won’t really discuss the anatomic and physiologic advantages today. What I will discuss, though, is the fact that Semenya has been told that she has to take drugs to decrease her testosterone levels or she cannot compete anymore. Semenya was told to decrease her testosterone levels or she could face a ban in the 800 m. The new rules state that:
Female athletes affected must take medication for six months before they can compete, and then maintain a lower testosterone level.
If a female athlete does not want to take medication, then they can compete in:
- International competitions in any discipline other than track events between 400m and a mile
- Any competition that is not an international competition
- The male classification at any competition, at any level, in any discipline
- Any intersex, or similar, classification
But Semenya has declined taking these drugs—so her future is up in the air. So, if Semenya—or any other athlete—has to take drugs to decrease their levels since it gives an unfair advantage, then, in my opinion, this may lead to changes in other sports as well.
Look at Michael Phelps. Michael Phelps has won a record 28, winning 23 medals at Rio in 2016. Phelps has a long, thin torso which decreases drag in the water. Phelps’ wing span is 6’7” while he is 6’4”—which is disproportionate to his height. He has the torso of a 6’8” person, which gives him a greater reach per stroke. His lower body is 5’10” which lowers the resistance against the water. He has large hands and feet (with flexible ankles), which help with paddling capacity (size 14 shoe; yours truly wears a size 13).
There is one more incredible thing about Phelps: He produces around 50 percent lower lactic acid. Think of the last time that you have run for some distance. The burning you feel in your legs is a build up of lactic acid. Lactic acid causes fatigue and also slows muscle contractions—this occurs through lactic acid passing through the bloodstream, becoming lactate. (Note that it does not necessarily cause fatigue; Brooks, 2001.) Phelps does not produce normal levels of lactic acid, and so he is ready to go again shortly after a bout of swimming.
Phelps said “In between the 200m free and the fly heats I have probably had in total about 10 minutes to myself.” A normal person’s muscles would be too fatigued and cramped. I would also assume that Phelps has an abundance of type I muscle fibers as well.
Now take Usain Bolt. The 100 m dash is, mostly, an anaerobic race. What this means is that mitochondrial respiration has minimal effect on the type of energy used during the event (Majumdar and Robergs, 2011). So during anaerobic events, there is no free oxygen to drive energy—the energy stored in the muscle is used to perform movement through a process called glycolysis. Sprinting is an intense exercise—fuel choice during exercise is determined by the intensity of said exercise. “A 100-meter sprint is powered by stored ATP, creatine phosphate, and anaerobic glycolysis of muscle glycogen.”
Now we can look at the physical advantages they have. Swimmers and runners, on average, have different centers of mass (Bejan, Jones, and Charles, 2010). In all actuality, Phelps and Bolt are the perfect example of this phenomenon. Winning runners have a West-African origin and winning runners are more likely to be white. These somatotypic differences between the two races influence why they excel in these two different sports.
Usain Bolt is 6’5”. Since he is that height, and he has long legs, he necessarily has a longer stride—Bolt is the perfect example of Bejan, Jones, and Charles’ (2010) paper. So take the average white sprinter of the same height as Bolt. Ceteris paribus, Bolt will have a higher center of mass than the white athlete due to his longer limbs and and smaller circumference. Krogman (1970) found that, in black and white youths of the same height, blacks had shorter trunks and longer limbs, which lends credence to the hypothesis.
Phelps is 6’4”. As noted above, he has a long torso and long limbs. Long torsos are conducive to a lower center of mass—what whites and Asians have, on average. So long torsos mean that one will have taller sitting heights than those with short torsos. This means that whites and Asians have taller sitting heights than blacks, who have shorter torsos. This average taller sitting height is conducive to the longer torsos which is why whites excel in swimming. Bejan, Jones, and Charles (2010) also note that, if it were not for the short stature of Asians, they would be better swimmers than whites.
In any case, the different centers of mass on average between blacks and whites are conducive to faster times in the sports they excel at. For whites, the three percent increase in center of mass means that there would be a 1.5 percent increase in winning speed and a 1.5 percent decrease in winning time in the case of swimming. The same holds for blacks, but in the case of running: their higher center of mass is conducive to a 1.5 percent increase in winning speed and also a 1.5 percent decrease in winning time, which would be a .15 second decrease, or from 10 s to 9.85 s—which is a large differential when it comes to sprinting. (Note that this phenomenon also holds for black women and white women—black women are better sprinters and white women are better swimmers. Asian women excel in the 100 m freestyle, but not Asian men for reasons discussed above.)
Now put this all together. If Phelps and Bolt have such advantages over their competition and they—supposedly—win due to them, then if Semenya has to decrease her T levels, why shouldn’t Phelps and Bolt decrease X, Y, or Z since they have physiologic/anatomic advantages as well? Why does no one talk about Semenya’s anatomic advantages over, say, white women and why only bring up Semenya’s testosterone levels? Forcing Semenya to decrease T levels will set a bad precedent in sport. What would stop a losing competitor from complaining that the winner—who keeps winning—has an “unfair” physiologic/anatomic advantage and must do X to change it? (Or say that the anatomic advantage they possess is “unfair” and they should be barred from competition?)
Here’s the thing: Watching sport, we want to see the best-of-the-best compete. Wouldn’t that logically imply that we want to see Semenya compete and not rid herself of her advantage? If Semenya’s physiologic advantage(s) is being discussed, why not Semenya’s anatomic advantages? It does not make sense to focus on one variable—as all variables interact to produce the athletic phenotype (Louis, 2004). Phelps and Bolt perfectly embody the results of Bejan, Jones, and Charles (2010)—they have, what I hope are—well-known advantages, and these advantages, on average, are stratified between race due to anatomic differences (see Gerace et al, 1994; Wagner and Heyward, 2000).
Phelps and Bolt have anatomic and physiologic advantages over their competition, just as Semenya does, just like any elite athlete, especially the winners compared to their competition. If Semenya is forced to decrease her testosterone levels, then this will set a horrible precedent for sport, and people may then clamor for Phelps and Bolt to do X, Y, and Z due to their physical advantages. For this reason, Semenya should not decrease her testosterone levels and should be allowed to compete in mid-distance running.
Helmuth Nyborg on the Social Construction of Race
2000 words
Helmuth Nyborg published an article in Psych titled Race as Social Construct (Nyborg, 2019). In the article, he responds to a National Geographic article There’s No Scientific Basis for Race—It’s a Made-Up Label. In the article, Nyborg quotes, what apparently are quotations, from the article. Yet, for example when it comes to this:
‘There’s No Scientific Basis for Race’—‘It’s a Made-Up Label’… ‘Races do not exist because we are equals’, ‘the concept of race is not grounded in genetics’, etc.
The second quote “Races do not exist because we are equals” is not in the article. (Though this is probably a general call-out to so-called “social constructivists about race.”) Now, I won’t’ nit-pick about it, since he is apparently speaking to his critics who make these claims. In any case, Nyborg’s article is titled Race as Social Construct. Where are constructivists about race said to be anti-realists or eliminativists about race? If Nyborg is really speaking to constructivists about race, then he’s strawmanning their position. Because social constructivists about race are realists about race.
Take the new AAPA Statement on Race and Racism, where they write:
… race has become a social reality that structures societies and how we experience the world. In this regard, race is real, as is racism, and both have real biological consequences.
““race” as a social reality — as a way of structuring societies and experiencing the world — is very real.”
So, if constructivists about race claim that “Races do not exist”, then why are social constructivists about race literally saying “race is real” and “”race” as a social reality … is very real”? Weird… Almost as if Nyborg is strawmanning the constructivist position. Nyborg asks if “NG also think[s] of species as a social construct?“. See Elstein (2003) for a view that species are socially constructed. In any case, I don’t think that Nyborg is familiar with the philosophical literature on the status of species.
Here is Nyborg’s first syllogism:
Samuel Morton is a reprehensible model racist with a fixed defintion of race.
1. Samuel Morton is the father of scientific racism.
2. (We “know” that the father of scientific racism has THE correct understanding of race).
3. Morton thinks that races represent separate acts of creation.
4. Morton thinks that races are ranked in a divine hierarchy.
5. Morton did not think that races were closely related.
6. Morton thinks that races has distinct characters which:
(a) Are immutable or “fixed” across generations (i.e., no transmutation, aka evolution).
(b) Are homogenous of “fixed” (in these senses of fixation) across individuals within races.
Ergo,
Morton is wrong about 3-6, and thus represent the opposite of reality. We can then say, given 1-2 and 3-6, that races do not exist.
This is ridiculous. Where has anyone written anything like this, that since Morton was a “racist” that “races do not exist”? Did Gould make that claim in Mismeasure? I personally think that Morton’s analysis was flawed by his own biases, but I do not make the claim that “races do not exist” because of it.
In any case, when it comes to Gould’s critique of Morton’s skulls, contra Jensen (1982), Rushton (1997) , and Lewis et al (2011), Gould’s arguments about Morton were largely correct (Weisberg, 2014; Kaplan, Pigliucci, and Banta, 2015; Weisberg and Paul, 2016). Specifically, Weisberg (2014) writes that “Although Gould made some errors
and overstated his case in a number of places, he provided prima facia evidence, as yet unrefuted, that Morton did indeed mismeasure his skulls in ways that conformed to 19th century racial biases.”
Now when it comes to this one, we’re getting somewhere:
Race does not Relate to Geographic Location
1. There are no fixed traits with specific geographic locations …” because …
2. “… as often as isolation has created differences among populations, migration and mixing have blurred or erased them.
Ergo,
3. “… our pictures of past ‘racial structures’ are almost always wrong” and harmful.
This is a good argument. However, it fails, in my opinion. Yes, there is no sharp delineation in traits between what are purported to be racial groupings. However, for biological racial realism to be true, there do not need to be. Take my article You Don’t Need Genes to Delineate Race. By looking at average facial and morphological features that exist in any continent, we can say that, although there is no sharp gradation and there are clines in phenotypes, that does not mean that there is no what we can say “average look” for the group. (Nyborg discusses “IQ” there, but I won’t get into it.)
Now take this one:
Races do not exist: We are Equals and Africans
1. “… all humans are closely related.”
2. In a very real sense, all people alive today are Africans.”
3. Genetic diversity in Africa is much larger than outside this continent.”
4. Because they [migrants] were just a small subset of Africa’s population, the migrants took with them only a fraction of its genetic diversity.”
5. Admittedly, “… the longer two groups are separated, the more distinctive tweaks [mutations] they will acquire”, BUT …
6. “The concept of race has no genetic or scientific basis.” (NG here refers to a Craig Venter statement at a White House meeting, June 2000; see later).
Ergo,
7. “Science tells us there is no genetic or scientific basis for race. Races do not exist because we are [all] equals.”
1-5 are true; though 6-7 are false. In any case, the existence of race is not a scientific matter. The questions “What is race?”, “Is race real?”, and “If race is real, how many races are there?” are philosophical, not scientific, matters. Nyborg brings up “Lewontin’s fallacy”, but take what Hardimon (2017: 22-23) writes about the matter:
It is worth noting that the force of the argument against the existence of racialist races from Lewontin’s data analysis is unaffected by the critique A.W.F. Edwards made in his 2003 paper “Human Genetic Diversity: Lewontin’s Fallacy.” The fallacy Edwards imputes to Lewontin consists in inferring that racial classification has no taxonomic signifigance from the finding that the between-race component of human genetic diversity is very small. The inference is fallacious because the fact that the between-race component of human genetic diversity is small does not entail that racial classification has no taxonomic signifigance. Lewontin’s locus-by-locus analysis (which does not consider the possibility of a correlation between individual loci) does not preclude the possibility that individual loci might be correlated in such a way that people could be grouped into traditional racial categories. The underlying though is that racial classification would have “taxonomic signifigance” were it possible to group people into traditonal racial categories by making use of correlations between individual loci. However, Lewontin’s argument that there are no racialist races because the component of within-race genetic variation is larger than the component of between-race genetic variation is untouched by Edwards’ objection. That conclusion rests solely on Lewontin’s statistical analysis of human variation (the validity of which Edwards grants) and does not pressupose the absence of correlational structure in the genetic data. In short, Lewontin’s data do not preclude the possibility that raciual classification might have taxonomic signifigance but they do preclude the possibility that racialist races exist.
Nyborg is, obviously, pushing the concept of racialist races, though Hardimon has shown that they do not exist. Nyborg says that “Educability and IQ are arguable [sic] physiological (Spearman, 1927)“. Nope.
Nyborg then presents his next syllogism:
Admixture and Displacement Have Erased All Race Differences
1. Race implies unadmixed groups between which there are fixed—“fix”, in the sense of fixation index—traits.
2. (From Reich (2018) race implies “primeval” groups…separated tens of thousands of years ago”.
3. Genetics shows that mixture and displacement have happened again and again”… and … as a result “Differences have been blurred or erased”.
4. Thus, “there are no fixed traits associated with specific geographic locations…”
5. And “our pictures of past ‘racial structures’ are almost always wrong” and harmful.
Ergo
Since human descent groups are mixed and do not exhibit fixed trait differences and since there are no 10-thousand-year-old primeval groups, there are no races.
This one is strong, and if an eliminativist/anti-realist about race were to use this argument (remember, Nyborg doesn’t understand that social constructivists are realists about race), then it would be strong. But that human populations are mixed and do not exhibit trait differences does not mean that race does not exist, that does not follow. That is a carry-over from the racialist concept of race, which is false.
Nyborg then presents his fifth syllogism:
Race is only Skin Color Deep
1. “When people speak about race, usually they seem to be referring to skin color and, at the same time, to something more than skin color.”
2. “This is the legacy of people such as Morton, who developed the “science” of race to suit his own prejudices and got the actual science totally wrong.”
3. “Science today tells us that the visible differences between people a re accidents of history. They reflect how our ancestors dealt with sun exposure, and not much else.”
4. There is no homogenous African race.
Ergo,
Since race is only based on skin color, it is made up by racists.
I have heard an argument similar to this, and it fails. Race isn’t ONLY BASED ON skin color, but it is a marker of race, along with ancestry and location. Of course, morphology and other phenotypic traits ground the scientific concept of “race” (minimalist/populationist race). Race, of course, does not mean only skin color, there are many other ways to delineate races, with skin color being but one tell.
Nyborg then writes:
Ducrest, Keller, and Rouling, 2008) [79] thus observed that darker color is associated with greater aggressiveness in 10 mammal species, three kinds of birds, and more Lizard forms entirely evaded them. They condemned the color analogue with respect to humans, and reacted forcefully when Rushton and Templer (2009) [80] drew data from no less than 113 countries and found that “… murder, rape, and serious assault were associated with darker skin color, lower IQ, higher birth rate, higher infant mortality, higher HIV/AIDS rate, lower life expectancy, and lower income”
Yea, Ducrest, Keller, and Rouling (2008) is one study that Rushton loved, as it, supposedly, gave a basis for darker color being associated with aggressiveness in a slew of different animals. I rebutted Rushton and Templer, in any case. Their study was ridiculous and they did not even heed what Ducrest, Keller, and Rouling (2008: 507) stated “… that human populations are therefore not expected to consistently exhibit the associations between melanin-based coloration and the physiological and behavioural traits reported in our study.” Must be hard for Rushton and Templer to read.
In sum, Nyborg is wrong that racial constructivists claim that “Races do not exist”, for if they did not exist, then what would constructivists be fighting for? Nyborg seems to be talking to anti-realists/eliminativists about race. Nyborg pushes a racialist concept about race, which was refuted by Hardimon (2017: Chapter 1). Races exist in a minimal sense (Hardimon, 2017) and U.S. sense (Spencer, 2014), but not in the racialist “HBD” sense. In this case, biological racial realism (Spencer, 2011) is true, but if we are going by Kaplan and Winther’s (2014) definitions, Rushton, Jensen, Lynn, and Nyborg would be the biological racial realists, whereas myself, Hardimon and Spencer would be biogenomic/cluster race realists. It seems that Nyborg needs to brush up on the philosophical literature, because what he claims that social constructivists about race believe are not true; he just strawmanned their position. In any case, I’ve shown that constructivists about race do not believe that race is not real. They may not believe that race is real in a biological manner, but they do in a social one, and that is enough for them to be race realists and believe that race exists.
(Also note how Kaplan and Winther (2014) note that “Social racial realism defends the existence of distinct human groups in our ordinary discourse and social interactions. Such groups are often identified and stabilized by “surface” factors such as skin color or facial features.” So, again, those who push a socialrace-type concept do not deny that race exists, on the contrary, they are realists about race. Nyborg got it wrong, and some of his critiques are good against those who deny the reality of race, but his racial ontology is false.
Race, Medicine, and Epigenetics: How the Social Becomes Biological
2050 words
Race and medicine is a tendentious topic. On one hand, you have people like sociologist Dorothy Roberts (2012) who argues against the use of race in a medical context, whereas philosopher of race Michael Hardimon thinks that we should not be exclusionists about race when it comes to medicine. If there are biological races, and there are salient genetic differences between them, then why should we disregard this when it comes to a medically relevant context? Surely Roberts would agree that we use her socio-political concept of race when it comes to medicine, but not treat them like biological races. Roberts is an anti-realist about biological races, whereas Hardimon is not—he recognizes that there is a minimalist and social aspect to race which are separate concepts.
In his book Rethinking Race: The Case for Deflationary Realism, Hardimon (2017, Chapter 8) discusses race and medicine after discussing and defending his different race concepts. If race is real—whether socially, biologically, or both—then why should we ignore it when it comes to medical contexts? It seems to me that many people would be hurt by such a denial of reality, and that’s what most people want to prevent, and which is the main reason why they deny that races exist, so it seems counterintuitive to me.
Hardimon (2017: 161-162; emphasis his) writes:
If, as seems to be the case, the study of medically relevant genetic variants among races is a legitamate project, then exclusionism about biological race in medical research—the view that there is no place for a biological concept of race in medical research—is false. There is a place for a biological concept of race in the study of medically relevant genetic variants among races. Inclusionism about biological race in medical research is true.
So, we should not be exclusionists (like Roberts), we should be inclusionists (like Hardimon). Sure, some critics would argue that we should be looking at the individual and not their racial or ethnic group. But consider this: Imagine that an individual has something wrong and standard tests do not find out what it is. The doctor then decides that the patient has X disease. They then treat X disease, and then find out that they have Y disease that a certain ethnic group is more likely to have. In this case, accepting the reality of biological races and its usefulness in medical research would have caught this disease earlier and the patient would have gotten the help they needed much, much sooner.
Black women are more likely to die from breast cancer, for example, and racism seems like it can explain a lot of it. They have less access to screening, treatment, care, they receive delays in diagnoses, along with lower-quality treatment than white women. But “implicit racial bias and institutional racism probably play an important role in the explanation of this difficult treatment” (Hardimon, 2017: 166). Furthermore, black women are more than twice as likely to acquire a type of breast cancer called “triple negative” breast cancer (Stark et al, 2010; Howlader et al, 2014; Kohler et al, 2015; DeSantis et al, 2019). Of course, this could be a relevant race-related genetic difference in disease.
We should, of course, use the concepts of socialrace when discussing the medical effects of racism (i.e., psychosocial stress) and the minimalist/populationist race concepts when discussing the medically relevant race-related genetic diseases. Being eliminativist about race doesn’t make sense—since if we deny that race exists at all and do not use the term at all anymore, there would be higher mortality for these “populations.” Thus, we should use both of Hardimon’s terms in regard to medicine and racial differences in health outcomes as both concepts can and will show us how and why diseases are more likely to appear in certain racial groups; we should not be eliminativists/exclusionists about race, we should be inclusionists.
Hardimon discusses how racism can manifest itself as health differences, and how this can have epigenetic effects. He writes (pg 155-156):
As philosopher Shannon Sullivan explains, another way in which racism may be shown to influence health is by causing epigenetic changes in the genotype. It is known that changes in gene expression can have durable and even transgenerational effects on health, passing from parents to their children and their children’s children. This suggests that the biological dimensions of racism can replicate themselves across more than one generation through epigenetic mechanisms. Epigenetics, the scientific study of such changes, explains how the process of transgenerational biological replication of ill health can occur without changes in the underlying DNA sequence.
If such changes to the DNA sequences can be transmitted to the next generation in the developmental system, then that means that the social can—and does—has an effect on our biology and that it can be passed down through subsequent generations. It is simple to explain why this makes sense: for if the developing organism was not plastic, and genes could not change based on what occurs in the environment for the fetus or the organism itself, then how could organisms survive when the environment changes if the “genetic code” of the genome were fixed and not malleable? For example, Jasienska (2009) argues that:
… the low birth weight of contemporary African Americans not only results from the difference in present exposure to lifestyle factors known to affect fetal development but also from conditions experienced during the period of slavery. Slaves had poor nutritional status during all stages of life because of the inadequate dietary intake accompanied by high energetic costs of physical work and infectious diseases. The concept of ‘‘fetal programming’’ suggests that physiology and metabolism including growth and fat accumulation of the developing fetus, and, thus its birth weight, depend on intergenerational signal of environmental quality passed through generations of matrilinear ancestors.
If the environmental quality—i.e., current environmental quality—is “known” by the developing fetus through cues from the mother’s nutrition, stress etc, then a smaller body size may be adaptive in that certain environment and the organism may survive with fewer resources due to smaller body size. In any case, I will discuss this in the future but it was just an example of a possible epigenetic modification on current slaves. I, personally, have noticed that a lot of blacks are really skinny and have really low body fat—who knows, maybe this could be part of the reason why?
This is something that sociologist Maurizio Meloni (2018) calls “the postgenomic body”—the fact that biology is malleable through what occurs in our social lives. So not only is the human brain plastic, but so is the epigenome and microbiome, which is affected by diet and lifestyle—along with what we do and what occurs to us in our social lives. So our social lives, in effect, can become embodied in our epigenome and passed down to subsequent generations. Similar points are also argued by Ulijaszek, Mann, and Elton (2012). (Also see my article Nutrition, Development, Epigenetics, and Physical Plasticity.)So in effect, environments are inherited too, and so, therefore, the environments that we find ourselves in are, in effect, passed down through the generations. Meloni (2018) writes:
On the other hand, by re-embedding the individual within a wider lineage of ancestral experiences and reconfiguring it as a holobiontic assemblage, it may literally dissolve the subject of emancipation. Moreover, the power of biological heredity may be so expanded (as it includes potentially any single ancestral experience) to become stronger than in any previous genetic view. Finally, the several iterations of plasticity that emerge from this genealogy appear so deeply racialized and gendered that it is difficult to quickly turn them into an inherently emancipatory concept. Even as a concept, plasticity has an inertial weight and viscosity that is the task of the genealogist to excavate and bring into view.
Thus, current biological states can be “tagged” and therefore be epigenetically transmitted to future generations. Think about it in this way: if epigenetic tags can be transmitted to the next generation then it would be presumed that that environment—or a similar one—would be what newer generations would be born in. Thus, the plasticity of the organism would help it in life, especially the immediate plasticity of the organism in the womb. Likewise, Kuzawa and Sweet (2008) argue:
that environmentally responsive phenotypic plasticity, in combination with the better-studied acute and chronic effects of social-environmental exposures, provides a more parsimonious explanation than genetics for the persistence of CVD disparities between members of socially imposed racial categories.
Of course, if we look at race as both a biological and social category (i.e., Spencer, 2014), then this is not surprising that differences in disease acquisition can persist “between members of socially imposed racial categories.” Phenotypic plasticity is the big thing here, as noted by many authors who write about epigenetics. If the organism is plastic (if it can be malleable and change depending on external environmental cues), then disease states can—theoretically—be epigenetically passed to future generations. This is just like Jasienska’s (2009, 2013, Chapter 5) argument that the organism—in this case, the fetus—can respond to the environmental quality that it is developing in and, therefore, differences in anatomy and physiology can and do occur based on the plasticity of the organism.
Lastly, Jan Badke, author of Above the Gene, Beyond Biology: Toward a Philosophy of Epigenetics (Baedke, 2018), argues that, since the gene-centered view of biology has been upended (i.e., Jablonka and Lamb, 2005; Noble, 2006, 2011, 2012, 2017) for a postgenomic view (Richardson and Stevens, 2015). Genes are not closed off from the environment; all organisms, including humans, are open systems and so, there are relationships between the environment, developmental system, and the genome which affect the developing organism. Baedke and Delgado (2019) argue that the “colonial shadow … biologicizes as well as racializes social-cultural differences among human groups.” Since every race faces specific life challenges in its environment, therefore, each race shows a “unique social status that is closely linked to its biological status.” Thus, differing environments, such as access to different foods (i.e., the effects of obesifying foods) and discrimination can and are passed down epigenetically. Baedke and Delgado (2019: 9) argue that:
… both racial frameworks nutrition plays a crucial role. It is a key pathway over which sociocultural and environmental difference are embodied as racial difference. Thus, belonging to a particular race means having a particular biosocial status, since races include two poles – a social status (e.g., class, socio-economic status) and a biological status (disease susceptibility) – which are closely interlinked. Against this background, human populations in Mexico become an exemplar of types of bodies that are not only relocated to a destabilizing modernized world in which they suffer from socio-economic deprivation. What is more, they become paradigmatic primitive bodies that are unbalanced, biologically deprived, and sick. In short, in these recent epigenetic studies poor places and lifestyles determine poor bodies, and vice versa.
In sum, accepting the reality of race—both in a minimalist/populationist biological manner and social manner—can and will help us better understand disease acquisition and differing levels of certain diseases between races. Recognizing the minimalist/populationist concepts of race will allow us to discover genetic differences between races that contribute to variation in different diseases—since genes do not alone outright cause diseases (Kampourakis, 2017: 19). Being eliminativist/exclusionist about race does not make sense, and it would cause much more harm than good when it comes to racial disease acquisition and mortality rates.
Furthermore, acknowledging the fact that the social dimensions of race can help us understand how racism manifests itself in biology (for a good intro to this see Sullivan’s (2015) book The Physiology of Racist and Sexist Oppression, for even if the “oppression” is imagined, it can still have very real biological effects that could be passed onto the next generation—and it could particularly affect a developing fetus, too). It seems that there is a good argument that the effects of slavery could have been passed down through the generations manifesting itself in smaller bodies; these effects also could have possibly manifested itself in regard to obesity in Latin America post-colonialism. Gravlee (2009) and Kaplan (2010) also argue that the social, too, manifests itself in biology.
(For further information on how the social can and does become biological see Meloni’s (2019) book Impressionable Biologies: From the Archaeology of Plasticity to the Sociology of Epigenetics, along with Meloni (2014)‘s paper How biology became social, and what it means for social theory. Reading Baedke’s and Meloni’s arguments on plasticity and epigenetics should be required before discussing these concepts.)
Lupus and Race/Ethnicity
1000 words
I’m watching Mystery Diagnosis right now, and I heard the narrator say that lupus is three times more common in African Americans than Caucasian Americans. (The woman was black.) So let’s look into it.
Lupus is a long-term autoimmune disease where the body’s immune system becomes hyperactive and attacks healthy tissue. It can damage any part of the body, skin cells, joints, organs. Many symptoms of lupus exist, like kidney inflammation, swelling, and damage to the blood, heart, joints, and lungs. No cure exists for lupus, though there are ways to minimize inflammation through diet and lifestyle.
Lupus is two to three times more likely to occur in women of color—blacks, Hispanics/Latinos, Native Americans, and others—compared to white Americans. Somers et al (2014) state that lupus affects 1 in 537 black women, “with black patients experiencing earlier age at diagnosis, >2-fold increases in SLE incidence and prevalence, and increased proportions of renal disease and progression to ESRD as compared to white patients.” However, Somers et al (2016) note that medical records may be poor or missing while the reliability of diagnosis is low for non-whites and non-blacks. They also note that race and ethny data in the US is based on self-ID for the parents and child on the birth certificate, but self-ID has almost a perfect relationship with geographic ancestry (i.e., race) (Tang et al, 2005).
Guillermo et al (2017: 7) write that:
Ethnicity is a biological and social construct, including not only genetic ancestry, but also cultural characteristics (language, religion, values, social behaviors, country of origin) yet it is an arbitrary definition [120]. Race is oftentimes used interchangeable with ethnicity but it mainly refers to the biological features of groups of people. Given that there are differences in the clinical characteristics and prognosis among different populations, it is worth evaluating the impact of race/ethnicity in SLE. Genetic ancestry influences the risk for the incidence of SLE; for example, Amerindian ancestry is associated with an increased number of risk alleles for SLE [121], and also with an early age at onset [122], Amerindian and African ancestry are associated with a higher risk for kidney involvement [122,123] and European ancestry with a lower risk [124].
First, let’s look at ref [120], which is McKenzie and Crowcroft (1994), who Guillermo et al (2017) cite as saying that ethnicity is “an arbitrary definition.” They note that some researchers use Blumenbach’s terms (see Spencer, 2014). They claim that modern definitions class Asians as Caucasian or black … what? They state that modern definitions classify Asians as black because “all disadvantaged groups [are] “black populations,”
[since] the experience of racism is paramount.” This is ridiculous on so many levels.
In any case, Southern Europeans are more likely to have a higher risk of renal involvement, and antibody production but along with that a lower risk of discoid rash whereas Western Europeans while Ashkenazi Jews “seem to be protected from neurologic manifestations” (see Richman et al, 2009). Asians and Native Americans in Canada are less likely to have manifestations than Africans; a type of lupus known as cutaneous vasculitis is more common in Native Americans from Canada, while Asians from Canada had a lower rate of serotisis and arthritis compared to Caucasians, Native Americans and African descendants (Peschken et al, 2015). However, Peschken et al (2015) note that while ethnicity was not that strong a predictor of damage accrual, low income was.
Kidney involvement is a major factor in the development of lupus (Bagamant and Fu, 2009), while it is more frequent in “Hispanics”, African-descendants, and Asians. Further, “Hispanics” and blacks are more likely to have end-stage renal failure than whites (Ricardo et al, 2015). When it comes to lupus nephritis—inflammation of the kidneys caused by lupus—“Hispanics” also have a better response to mycophenolate mofetil, which is an immunosuppressive drug that prevents organ rejection (Appel et al, 2009). After the onset of the disease, the disease declines slowly in “Hispanics”, then Africans, and finally fastest in whites. There also seems to be an SES factor in the aetiology of the disease. Sule and Petri (2005) write that “Socioeconomic status can have a major impact on SLE disease manifestations and mortality, independent of ethnicity“, while saying that association with SES is all over the place, with there being no relationship with SES and lupus acquisition.
Vila et al (2003) studied “Hispanics” from Texas and Puerto Rico. They noted that those from Texas accrued more damage than those from Puerto Rico. This is not surprising. “Hispanics” are not a homogenous group (they are a socialrace with no minimalist correlate, they have differing admixture from all over; “Hispanics” can be of any race. Vila et al (2007: 362) note that:
This diversity appears to be areflection of the great variability that exists between these populations with regards to their genetic, environmental and sociodemographic backgrounds.
“Hispanics” from the southeast part of America are different ethnically than those from the southeast.
Blacks and “Hispanics” have a higher rate of mortality than whites, but these differences disappear once SES is accounted for (Ward, Pyun, and Studenski, 1995; Kasitanon, Magder, and Petri, 2006; Fernandez et al, 2007). There could be some genetic differences between races/ethnies that contribute to disease differences between them. But as Kampourakis (2017: 19) notes in his book Making Sense of Genes:
… genes do not alone produce characters or disease but contribute to their variation. This means that genes can account for variation in characters but cannot alone explain their origin.
In sum, there is a wide range of differences between races and ethnies when it comes to lupus. Is the main cause environmental or genetic? Neither, as genes and environment interact to form disease (and any other) phenotypes. So if one at-risk minority group has a low SES, that may be a risk factor. The fact that there are ethnic differences in response to autoimmune drugs when it comes to certain forms of lupus is interesting. The wide range of ethnic differences in the acquisition of the disease is interesting, with Ashkenazi Jews seemingly protected from the disease. In any case, there are racial/ethnic differences in the acquisition of this disease and to better treat those with this disease—and any other—we need to be realists about race, whether it’s biological or social, since there are very real disease and mortality outcomes between them.
What Rushton Got Wrong
1700 words
JP Rushton’s career was pretty much nothing but peddling bullshit. In the beginning of his career, he was a social learning theorist. He published a book Altruism, Socialization, and Society (Rushton, 1980). I bought the book a few years back when I was still a hardcore Rushton defender to see what he wrote about before he started pushing IQ and evolutionary theories about human races and I thought it was pretty good. In any case, Rushton got a lot wrong. So much so, that his career was, in my opinion, wasted peddling bullshit. Rushton was shown to be wrong time and time again on r/K theory and cold winter theory; Rushton was shown to be wrong time and time again on his crime theorizing; and Rushton’s and Jensen’s papers on the causes of the black-white IQ gap rest on a misunderstanding of heritability. In this piece, I will cover those three subjects.
Recently, two new papers have appeared that have a bone to pick with Rushton: One by Flynn (2019) and the other by Cernovsky and Litman (2019). Flynn discusses Rushton’s claims on the method of correlated vectors, his cold winter theory (that Asians and Europeans were subjected to harsher climates which led to higher levels of intelligence and therefore IQ) and his misuse of regression to the mean. He also discussed how the black-white IQ gap is environmental in nature (which is the logical position to hold, since IQ tests are tests of middle-class knowledge and skills (Richardson, 2002) and they are not construct valid).
Cold Winters Theory
Rushton theorized that, due to exposure to harsher environments, that Europeans and East Asians evolved to be more intelligent than Africans who stayed in the, what I assume to be, less harsh environments of Africa (Rushton, 1985). This is Rushton’s “Differential K theory.” Flynn (2019) writes that he “can supply an evolutionary scenario for almost any pattern of current IQ scores.” And of course, one can do that with any evolutionary adaptive hypothesis.
Even Frost (2019) admits that “there is no unified evolutionary theory of human intelligence, other than the general theory of evolution by natural selection.” But since “natural selection” is not a mechanism (Fodor, 2008; Fodor and Piattelli-Palmarini, 2010), then it cannot explain the evolution of intelligence differences, nevermind the fact that, mostly, these claims are pushed by differences in non-construct valid IQ test scores.
In any case, Rushton’s theory is a just-so story.
r/K selection
Judith Anderson (1991) refuted Rushton’s hypothesis on ecological grounds. Rushton asserted that Africans were r-selected whereas Asians and Europeans were more K-selected. Rushton, however, did not even use alpha-selection, which is selection for competitive ability. So r- and K selection is based on density-independence and density-dependence. K-selection is expected to favor genotypes that persist at high densities—increasing K—whereas r-selection is expected to favor genotypes that increase more quickly at low densities—increasing r. Alpha-selection can also occur at high or low population densities but is more likely in high densities. Though alpha-selection “favours genotypes that, owing to their negative effects on others, often reduce the growth rate and the maximum population size” (Anderson, 1991: 52). I further discussed the huge flaws with Rushton’s r/K model here. So Rushton’s theory fails on those grounds, along with many others.
Race
When it came to race, Rushton was a lumper, not a splitter. What I mean by these terms is simple: lumpers lump together Native Americans with East Asians and Pacific Islanders with Africans while splitters split them into further divisions. Why was Rushton a lumper? Because it fit more with his theory, of course. I remember back when I was a Rushton-ist, and I was, too, a lumper, that to explain away the low IQs of Native Americans—and in turn their achievements—was that they still had their intelligence from the cold winters and that’s when they did their achievements. Then, as they spent more time in hotter climates, they became dumber. In any case, there is no justification for lumping Native Americans with East Asians. Looking through Rushton’s book, he gives no justification for his lumping, so I can only assume that it is bias on his part. Now I will justify the claim that splitting is better than lumping. (Rushton also gave no definition of race, and according to Cernovsky and Litman (2019: 54), Rushton “failed to provide any scientific definition of race …”
Race is both a social and biological construct. I can justify the claim that Natives and East Asians are distinct races in one way here: ask both groups if the other is the same race. What do you think the answer will be? Now, onto genetics.
Spencer (2014) discusses the results from Tishkoff et al (2009), saying that when they added 134 ethnic groups to the ones found in the HDGP sample of 52, the K=5 partition clustered Caucasians, Mongoloids, and three distinct sets of Africans. Mongoloids, in this case, being East Asians, Native Americans, and Oceanians. But Tishkoff et al oversampled African ethnic groups. This, though, does not undercut my argument: of course when you oversample ethnic groups you will get the result of Tishkoff et al (2009) and since Africans were oversampled, the populations more genetically similar were grouped into the same cluster, which, of course, does not mean they are the same race.
Census racial discourse is just national racial discourse. The census uses defers to the OMB to define race. How does the OMB define race? The OMB defines “race” as “sets of” populations. Race in US racial discourse designates a set of population groups, thus, race is a particular, not a kind.
I can then invoke Hardimon’s (2017) argument for the existence of minimalist races:
1 There are differences in patterns of visible physical features which correspond to geographic ancestry.
2 These patterns are exhibited between real groups.
3 These groups that exhibit these physical patterns by geographic ancestry satisfy conditions of minimalist race.
C Race exists.
Now we can say:
1 If Native Americans and East Asians are phenotypically distinct, then they are different races.
2 Native Americans and East Asians are phenotypically distinct.
C Therefore Native Americans and East Asians are different races.
Crime
Rushton arbitrarily excluded data that did not fit his theory. How dishonest. Cernovsky and Litman (2019) write:
When Rushton presented crime statistics derived from 2 Interpol Yearbooks as allegedly supporting his thesis that Negroids are more crime inclined than Caucasoids, he arbitrarily excluded disconfirmatory data sets. When all data from the same two Interpol Yearbooks are re-calculated, most of the statistically significant trends in the data are in the direction opposite to Rushton’s beliefs: Negroids had lower crime rates than Caucasoids with respect to sexual offenses, rapes, theft, and violent theft or robbery, with most correlation coefficients exceeding .60. While we do not place much credence in such Interpol statistics as they only reproduce information provided by government officials of different countries, our re-analysis indicated that Rushton excluded data that would discredit his theory.
Further throwing a wrench into Rushton’s assertions is his claim that Mongoloids constitutes both East Asians and Native Americans. Well, Central America has some of the highest crime rates in the world—even higher than in some African countries. What is the ad-hoc justification for explaining away this anomaly if they truly are the same race? If they are the same race, why is the crime rate so much higher in Central America? Surely, Rushton’s defenders would claim something along the lines of recent evolution towards X, Y, and Z. But then I would say, then on what basis are they the same race? No matter what Rushton’s defenders say, they are boxed into a corner.
IQ
Lastly, Rushton and Jensen (2005) argued, on the basis of heritability estimates, and twin studies, that the black-white IQ gap is largely genetic in nature. But there are a few problems. They rely largely on a slew of trans-racial adoption studies, all of which have been called into question (Thomas, 2017). IQ tests, furthermore, are not construct valid (Richardson and Norgate, 2015; Richardson, 2017). Heritability estimates also fail. This is because, in non-controlled environments these stats do not tell us much, if anything (Moore and Shenk, 2016). Likewise, Guo (2000: 299) concurs, writing “it can be argued that the term ‘heritability’, which carries a strong conviction or connotation of something ‘heritable’ in everyday sense, is no longer suitable for use in human genetics and its use should be discontinued.” (For more arguments against heritability, read Behavior Genetics and the Fallacy of Nature vs Nurture.)
Rushton and Jensen (2005) also relied on the use of twin studies, however, all of the assumptions that researchers use to attempt to immunize their arguments from refutation are circular and ad hoc; they also agree that MZs experience more similar environments than DZs, too (Joseph et al, 2014; Joseph, 2016, see a summary here; Richardson, 2017). In any case, the fact that G and E interact means that heritability estimates are, in effect, useless in humans. Farm animals are bred in highly controlled environments; humans are not. Thus, we cannot—and should not—accept the results of twin studies; they cannot tell us whether or not genes are responsible for any behavioral trait.
Conclusion
There was a lot that Rushton got wrong. His cold winters theory is a just-so story; East Asians and Native Americans are not the same race; heritability estimates are not a measure of how much genes have to do with phenotypic variation within or between groups; IQ tests are not construct valid; r/K selection theory was slayed as early as 1991 and then again in 2002 (Graves, 2002); twin studies are not informative when it comes to how much genes influence traits, they only measure environmental similarity; and finally, Rushton omitted data that did not fit his hypothesis on racial differences in crime.
It’s sad to think that one can spend a career—about 25 years—spewing nothing but pseudoscience. One of the only things I agree with him on is that races are real—but when it comes to the nuances, I disagree with him, because there are five races, not three. Rushton got a lot wrong, and I do not know why anyone would defend him, even when these glaring errors are pointed out. (For a good look into Rushton’s lies, see Dutton’s (2018) book J. Philippe Rushton: A Life History Perspective and my mini-review on the book.)
