
Home » Posts tagged 'Diet'
Tag Archives: Diet
Vegans/Vegetarians vs. Carnivores and the Neanderthal Diet
2050 words
The vegan/vegetarian-carnivore debate is one that is a false dichotomy. Of course, the middle ground is eating both plants and animals. I, personally, eat more meat (as I eat a high protein diet) than plants, but the plants are good for a palate-switch-up and getting other nutrients in my diet. In any case, on Twitter, I see that there is a debate between “carnivores” and “vegans/vegetarians” on which diet is healthier. I think the “carnivore” diet is healthier, though there is no evolutionary basis for the claims that they espouse. (Because we did evolve from plant-eaters.) In this article, I will discuss the best argument for ethical vegetarianism and the evolutionary basis for meat-eating.
Veganism/Vegetarianism
The ethical vegetarian argument is simple: Humans and non-human animals deserve the same moral consideration. Since they deserve the same moral consideration and we would not house humans for food, it then follows that we should not house non-human animals for food. The best argument for ethical vegetarianism comes from Peter Singer from Unsanctifying Animal Life. Singer’s argument also can be extended to using non-human animals for entertainment, research, and companionship.
Any being that can suffer has an interest in avoiding suffering. So the equal consideration of interests principle (Guidi, 2008) asserts that the ability to suffer applies to both human and non-human animals.
Here is Singer’s argument, from Just the Arguments: 100 of the Most Important Arguments in Western Philosophy (pg. 277-278):
P1. If a being can suffer, then that being’s interests merit moral consideration.
P2. If a being cannot suffer, then that beings interests do not merit moral consideration.
C1. If a being’s interests merit moral consideration, then that being can suffer (transposition, P2).
C2. A being’s interests merit moral consideration if and only if that being can suffer (material equivalence, P1, C1).
P3. The same interests merit the same moral consideration, regardless of what kind of being is the interest-bearer (equal consideration of interests principle).
P4. If one causes a being to suffer without adequate justification, then one violates that being’s interests.
P5. If one violates a being’s interests, then one does what is morally wrong.
C3. If one causes a being to suffer without adequate justification, then one does what is morally wrong (hypothetical syllogism, P4, P5).
P6. If P3, then if one kills, confines, or causes nonhuman animals to experience pain in order to use them as food, then one causes them to suffer without adequate justification.
P7. If one eats meat, then one participates in killin, confining, and causing nonhuman animals to experience pain in order to use them as food.
C4. If one eats mea, then one causes nonhuman animals to suffer without adequate justification (hypothetical syllogism, P6, P7).
C5. If one eats meat, the one does what is morally wrong (hypothetical syllogism, C3, C4).
This argument is pretty strong, indeed it is sound. However, I personally will never eat a vegetarian/vegan diet because I love eating meat too much. (Steak, turkey, chicken.) I will do what is morally wrong because I love the taste of meat.
In an evolutionary context, the animals we evolved from were plant-eaters. The amount of meat in our diets grew as we diverged from our non-human ancestors; we added meat through the ages as our tool-kit became more complex. Since the animals we evolved from were plant-eaters and we added meat as time went on, then, clearly, we were not “one or the other” in regard to diet—our diet constantly changed as we migrated into new biomes.
So although Singer’s argument is sound, I will never become a vegan/vegetarian. Fatty meat tastes too good.
Nathan Cofnas (2018) argues that “we cannot say decisively that vegetarianism or veganism is safe for children.” This is because even if the vitamins and minerals not gotten through the diet are supplemented, the bioavailability of the consumed nutrients are lower (Pressman, Clement, and Hayes, 2017). Furthermore, pregnant women should not eat a vegan/vegetarian diet since vegetarian diets can lead to B12 and iron deficiency along with low birth weight and vegan diets can lead to DHZ, zinc, and iron deficiencies along with a higher risk of pre-eclampsia and inadequate fetal brain development (Danielewicz et al, 2017). (See also Tan, Zhao, and Wang, 2019.)
Carnivory
Meat was important to our evolution, this cannot be denied. However, prominent “carnivores” take this fact and push it further than it goes. Yes, there is data that meat-eating allowed our brains to grow bigger, trading-off with body size. Fonseca-Azevedo and Herculano-Houzel (2012) showed that metabolic limitations resulting from hours of feeding and low caloric yield explain the body/brain size in great apes. Plant foods are low in kcal; great apes have large bodies and so, need to eat a lot of plants. They spend about 10 to 11 hours per day feeding. On the other hand, our brains started increasing in size with the appearance of erectus.
If erectus ate nothing but raw foods, he would have had to eat more than 8 hours per day while hominids with neurons around our level (about 86 billion; Herculano-Houzel, 2009). Thus, due to the extreme difficulty of attaining the amount of kcal needed to power the brains with more neurons, it is very unlikely that erectus would have been able to survive on only plant foods while eating 8+ hours per day. Indeed, with the archaeological evidence we have about erectus, it is patently ridiculous to claim that erectus did eat for that long. Great apes mostly graze all day. Since they graze all day—indeed, they need to as the caloric availability of raw foods is lower than in cooked foods (even cooked plant foods would have a higher bioavailability of nutrients)—then to afford their large bodies they need to basically do nothing but eat all day.
It makes no sense for erectus—and our immediate Homo sapiens ancestors—to eat nothing but raw plant foods for what amounts to more than a work day in the modern world. If this were the case, where would they have found the time to do everything else that we have learned about them in the archaeological record?
There is genetic evidence for human adaptation to a cooked diet (Carmody et al, 2016). Cooking food denatures the protein in it, making it easier to digest. Denaturation is the alteration of the protein shape of whatever is being cooked. Take the same kind of food. That food will have different nutrient bioavailability depending on whether or not it is cooked. This difference, Herculano-Houzel (2016) and Wrangham (2009) argue is what drove the evolution of our genus and our big brains.
Just because meat-eating and cooking was what drove the evolution of our big brains—or even only allowed our brains to grow bigger past a certain point—does not mean that we are “carnivores”; though it does throw a wrench into the idea that we—as in our species Homo sapiens—were strictly plant-eaters. Our ancestors ate a wide-range of foods depending on the biome they migrated to.
The fact that our brain takes up around 20 percent of our TDEE while representing only 2 percent of our overall body mass, the reason being our 86 billion neurons (Herculano-Houzel, 2011). So, clearly, as our brains grew bigger and acquired more neurons, there had to have been a way for our ancestors to acquire the energy need to power their brains and neurons and, as Fonseca-Azevedo and Herculano-Houzel (2012) show, it was not possible on only a plant diet. Eating and cooking meat was the impetus for brain growth and keeping the size of our brains.
Take this thought experiment. An asteroid smashes into the earth. A huge dust cloud blocks out the sun. So the asteroid would have been a cause of lowering food production. This halting of food production—high-quality foods—persisted for hundreds of years. What would happen to our bodies and brains? They would, of course, shrink depending on how much and what we eat. Food scarcity and availability, of course, do influence the brain and body size of primates (Montgomery et al, 2010), and humans would be no different. So, in this scenario I have concocted, in such an event, we would shrink, in both brain and body size. I would imagine in such a scenario that high-quality foods would disappear or become extremely hard to come by. This would further buttress the hypothesis that a shift to higher-quality energy is how and why our large brains evolved.
Neanderthal Diet
A new analysis of the tooth of a Neanderthal apparently establishes that they were mostly carnivorous, living mostly on horse and reindeer meat (Jaouen et al, 2019). Neanderthals did indeed have a high-meat diet in northerly latitudes during the cold season. Neanderthals in Southern Europe—especially during the warmer seasons—however, ate a mixture of plants and animals (Fiorenza et al, 2008). Further, there was a considerable plant component to the diet of Neanderthals (Perez-Perez et al, 2003) (with the existence of plant-rich diets for Neanderthals being seen mostly in the Near East; Henry, Brooks, and Piperno, 2011) while the diet of both Neanderthals and Homo sapiens varied due to climatic fluctuations (El Zataari et al, 2016). From what we know about modern human biochemistry and digestion, we can further make the claim that Neanderthals ate a good amount of plants.
Ulijaszek, Mann, and Elton (2013: 96) write:
‘Absence of evidence’ does not equate to ‘evidence of absence,’ and the meat-eating signals from numerous types of data probably swamp the plant-eating signlas for Neanderthals. Their dietary variability across space and time is consistent with the pattern observed in the hominin clade as a whole, and illustrates hominin dietary adaptatbility. It also mirrors trends observed in modern foragers, whereby those populations that live in less productive environments have a greater (albeit generally not exclusive) dependance on meat. Differences in Neanderthal and modern human diet may have resulted from exploitation of different environments: within Europe and Asia, it has been argued that modern humans exploited marginal areas, such as steppe environments, whereas Neanderthals may have preferred more mosaic, Mediterranean-type habitats.
Quite clearly, one cannot point to any one study to support an (ideologically driven) belief that our genus or Neanderthals were “strictly carnivore”, as there was great variability in the Neanderthal diet, as I have shown.
Conclusion
Singer’s argument for ethical vegetarianism is sound; I personally can find no fault in it (if anyone can, leave a comment and we can discuss it, I will take Singer’s side). Although I can find no fault in the argument, I would never become a vegan/vegetarian as I love meat too much. There is evidence that vegan/vegetarian diets are not good for growing children and pregnant mothers, and although the same can be said for any type of diet that leads to nutrient deficiencies, the risk is much higher in these types of plant-based diets.
The evidence that we were meat-eaters in our evolutionary history is there, but we evolved as eclectic feeders. There was great variability in the Neanderthal diet depending on where they lived, and so the claim that they were “full-on carnivore” is false. The literature attests to great dietary flexibility and variability in both Homo sapiens and Neanderthals, so the claim that they ate meat and only meat is false.
My conclusion in my look into our diet over evolutionary time was:
It is clear that both claims from vegans/vegetarians and carnivores are false: there is no one “human diet” that we “should” be eating. Individual variation in different physiologic processes implies that there is no one “human diet”, no matter what type of food is being pushed as “what we should be” eating. Humans are eclectic feeders; we will eat anything since “Humans show remarkable dietary flexibility and adaptability“. Furthermore, we also “have a relatively unspecialized gut, with a colon that is shorter relative to overall size than in other apes; this is often attributed to the greater reliance on faunivory in humans (Chivers and Langer 1994)” (Ulijaszek, Mann, and Elton, 2013: 58). Our dietary eclectism can be traced back to our Australopithecine ancestors. The claim that we are either “vegetarian/vegan or carnivore” throughout our evolution is false.
There is no evidence for both of these claims from both of these extreme camps; humans are eclectic feeders. We are omnivorous, not vegan/vegetarian or carnivores. Although we did evolve from plant-eating primates and then added meat into our diets over time, there is no evidence for the claim that we ate only meat. Our dietary flexibility attests to that.
Is Diet and Exercise Eugenic?
1550 words
Eugenics can be defined as “the science of improving a human population by controlled breeding to increase the occurrence of desirable heritable characteristics.” Though, in his book Genetic Ethics: An Introduction, Farrelly (2018: 30) cites Bertrand Russel’s definition of eugenics. Eugenics is “the attempt to improve the biological character of a breed by deliberate methods adopted to that end.” So, eugenics does not have to be ‘bad’, if it is morally justifiable and defensible, if they treat all people as free and equal (which most eugenic movements in the past have not done. See my article Eugenics and the State for a history of eugenics and the policies that arose from it.)
Dieting (defined as “what one eats”, not the other commonly-used definition “when one is in caloric restriction under TDEE”) and exercise change the expression of genes in the genome. For example, mature skeletal muscle can adapt to numerous stressors—indeed, if it could not, then we would not be able to choose to gain (or lose) muscle mass. Exercise induces the activity of certain genes (Vissing, Anderson, and Schjerling, 2005). One study on endurance athletes showed that there are pronounced effects of gene expression on exercised and non-exercised muscles (Catoire et al, 2012). One study showed that the ingestion of glucose during exercise decreases the gene expression of genes associated with fatty acid metabolism (Civitarese et al, 2005). Numerous epigenetic changes are also induced by exercise (Ntanasis-Stathopoulos, Tzanninis, and Koutsilieris, 2013). Miyamoto-Mikami et al (2018) showed that young men who participated in high-intensity intermittent exercise training showed that 79 genes had an elevated expression whereas 73 genes were significantly reduced.
Williams and Neufer (1996) show that long-term responses in regard to adaptations in regard to a specific exercise “require changes in gene expression, mediated by changes in the rate of transcription of specific genes and in the rate of synthesis of
specific proteins.” Further, diet and exercise can change the transcriptional properties of skeletal muscle, which induce further physiological changes (Hargreaves and Cameron-Smith, 2002). There is even preliminary evidence that diet and exercise affects the epigenome over several generations (Barres and Zierath, 2016). Since changes occur to the epigenome due to environmental stressors, and exercise is an environmental stressor, it follows that exercise, too, can change the epigenome.
People visit the gym to change their biology. Since people visit the gym to change their biology, are they involved in “self-eugenics”? I would say yes, going with the definition from Russell quoted above. That one wants to change their biology means that they are most likely not currently happy with the way their biological phenotype currently is. So they visit the gym, begin a diet (defined here as “caloric restriction”) in order to change their biological phenotype since they are not happy with it. Methods like diet and exercise seek to improve the biological character of a breed through deliberate methods, and so, fall under the umbrella of “eugenics.”
But there is a difference between this type of “eugenics” and methods commonly thought of when “eugenics” are discussed. “When eugenic measures exemplify moral and epistemic virtue rather than vice, they are morally obligatory rather than simply morally permissible” (Farrelly, 2018: 42). Prescribing (a sensible) diet and exercise to a populace can and will improve their health; further, educating people on the right and wrong things to eat (“right and wrong things to eat” in regard to their current goals) and how these things we eat affect our physiology is not morally objectionable nor is it coercive.
Think of the eugenic policies I discussed in my article on eugenics and the State. The policies discussed (such as forced sterilization, infanticide, forced contraceptive measures, and selective breeding) are immoral: the State is attempting to force its ideals on the populace, and so it can be argued that it is immoral since individual autonomy is taken away (or attempted to be taken away). On the other hand, prescribing diet and exercise is not eugenic in this manner: it’s just a prescription, what one should do if they would like to live their life to the highest quality. This includes staying away from highly processed and refined foods (carbs) and other, “non-natural” foodstuffs. This is only a suggestion based on the current state of nutritional knowledge; if one wants to live the best-possible life then they should diet and exercise.
On the other hand, we can take a State-measure and, using the definition in this article from Russell, can say that this measure is eugenic, but its similarities to what is being argued here is irrelevant, since I am arguing for education, not forcing people to do something (though I will state my views on this matter at the end, which I still honestly think about since it conflicts with some of my views.)
Back in the beginning of this decade, then-mayor of NYC Michael Bloomberg “proposed [a] regulation that would bar food service establishments from selling certain sugary drinks in containers larger than sixteen ounces” in an effort to “reduce the city’s obesity rate.” When this law was proposed, I was all for it. People cannot make decisions for themselves, because when they do, they make the “wrong” (in regard to, what I would assume to be what people try to achieve—a healthy lifestyle) decisions, and so, I thought that a policy like this was a good idea, because who the hell needs a 64 oz. Big Gulp soda (which could have up to 700 kcal in the cup) from 7-11? Why would someone need to down almost 2 liters of soda in one go? Note that, I would assume, the individual would not be caught dead drinking out of a 2-liter bottle of soda (though I have seen quite a lot of people do so, even early in the morning). But there is no problem using the cup since its size is kind of deceptive—deceptive in the manner that it does not look like the 2-liter bottle of (family-sized) soda.
I loved this proposal when it was announced. It would, I thought, attempt to address one aspect of our obesity problem (since nearly 40 percent of all of the added sugars we consume come from sugary drinks). Back then, I was more libertarian in my politics, but I thought that the policy was a good idea, even though it conflicted with my views on politics. I now do not believe we should take these types of measures—I believe that education is sufficient, along with getting rid of food deserts which hamper the ability of those in those deserts to get access to good, high-quality food (which affects certain races over others; National Research Council, 2009).
The view held by Bloomberg, and now current NYC mayor Bill Deblasio, is an example of a policy that would take away one’s choice to drink what they would like. Bloomberg’s rationale was that, if people wanted more of the drink, then they can go over and refill their cup so that they can see what and how much they are actually drinking. This, on its face, is sensible. If one wants to drink the same amount they would have drank in, say, a 64 oz. Big Gulp, they can keep refilling their cup in order to get the same amount of liquid they would have gotten in the bigger cup. But, what if someone wants a 64 oz. Big Gulp? What about a 128 oz. Ultra Big Gulp? A 256 oz. Super Ultra Big Gulp? Is there anywhere we should draw this line? Should we?
In any case, I have shown that exercise and diet is “eugenic” in the sense of Russel’s definition. But it is not “eugenic” in the sense of, in my opinion, what most people mean when they discuss “eugenics”: taking away one’s individual autonomy to do what they want, forcing them to do something. (Though, they are not being told they cannot drink sugary drinks, they are being told that there is a size limit on how big their cup is; they would be forced to drink a sugary drink in a small cup.)
Bloomberg’s proposed measure is quite obviously eugenic since it “attempt[s] to improve the biological character of a breed by deliberate methods adopted to that end.” Is the health of the populace more important than individual autonomy to be able to buy their 256 oz. Super Ultra Big Gulp? Or is one’s ability to freely drink their 256 oz. Ultra Big Gulp more important? If it can be shown that this policy would reduce the number of obese people in the City, should it be attempted?
These are important (moral) questions to answer. I am honestly undecided here; this issue is incredibly complex. Though, we do know one thing: exercise and diet is “eugenic” in Russel’s sense, and the measures exemplify moral and epistemic virtue so it is not like “State-forced” eugenics of old. Whether or not there is a negative connotation to “eugenics” depends on whether or not it pursues sound and morally justifiable aims. Therefore, though prescribing diet and exercise is eugenic since they both influence the epigenome and gene expression (along with it falling under Russel’s definition of eugenics), it is not eugenic in a negative sense, since there are sound and morally justifiable aims in prescribing diet and exercise to the population at large.
Otzi Man’s Last Meal and the Diet of Neanderthals
1100 words
The debate on what type of diet in regard to macronutrient differences rages on. Should we eat high carb, low fat (HCLF)? Or low carb, high fat (LCHF) or something in between? The answer rests on, of course, the type of diets that our ancestors ate—both immediate and in the distant past. In the 1990s, a frozen human was discovered in the Otzal mountains, which gave him the name “Otzi man.” About 5,300 years ago, he was frozen in the mountains. The contents of his stomach have been analyzed in the 27 years since the discovery of Otzi, but an in-depth analysis was not possible until now.
A new paper was published recently, which analyzed the stomach contents of Otzi man (Maixner et al, 2018). There is one reason why it took so long to analyze the contents of his stomach: the authors state that, due to mummification, his stomach moved high up into his rib cage. The Iceman was “omnivorous, with a diet consisting both of wild animal and plant material” (Maixner et al, 2018: 2). They found that his stomach had a really high fat content, with “the presence of ibex and red deer” (pg 3). He also “consumed either fresh or dried wild meat“, while “a slow drying or smoking of the meat over the fire would explain the charcoal particles detected previously in the lower intestine content.“(pg 5).
The extreme alpine environment in which the Iceman lived and where he have been found (3,210 m above sea level) is particularly challenging for the human physiology and requires optimal nutrient supply to avoid rapid starvation and energy loss [31]. Therefore, the Iceman seemed to have been fully aware that fat displays an excellent energy source. On the other hand, the intake of animal adipose tissue fat has a strong correlation with increased risk of coronary artery disease [32]. A high saturated fats diet raises cholesterol levels in the blood, which in turn can lead to atherosclerosis. Importantly, computed tomography scans of the Iceman showed major calcifications in arteria and the aorta indicating an already advanced atherosclerotic disease state [33]. Both his high-fat diet and his genetic predisposition for cardiovascular disease [34] could have significantly contributed to the development of the arterial calcifications. Finally, we could show that the Iceman either consumed fresh or dried meat. Drying meat by smoking or in the open air are simple but highly effective methods for meat preservation that would have allowed the Iceman to store meat long term on journeys or in periods of food scarcity. In summary, the Iceman’s last meal was a well-balanced mix of carbohydrates, proteins, and lipids, perfectly adjusted to the energetic requirements of his high-altitude trekking. (Maixner et al, 2018: 5)
They claim that “the intake of animal adipose tissue fat has a strong correlation with increased risk of coronary artery disease“, of course, citing a paper that the AHA is involved in (Sacks et al, 2017) which says that “Randomized clinical trials showed that polyunsaturated fat from vegetable oils replacing saturated fats from dairy and meat lowers CVD.” This is nonsense, because dietary fat guidelines have no evidence (Harcombe et al, 2016; Harcombe, Baker, and Davies, 2016; Harcombe, 2017). Saturated fat consumption is not even associated with all-cause mortality, type II diabetes, ischemic stroke, CVD (cardiovascular disease) and CHD (coronary heart disease) (de Sousa et al, 2015).
Thus, if anything, what contributed to Otzi man’s arterial calcification seems to be grains/carbohydrates (see DiNicolantonio et al, 2017), not animal fat. Fats, at 9 kcal per gram, were better for Otzi to consume, as he got more kcal for his buck; eating a similar portion in carbohydrates, for example, would have meant that Otzi would have had to spend more time eating (since carbs have less than half the energy that animal fat does). Since his stomach had ibex (a type of goat) and red deer, it’s safe to say that many of his meals consisted mainly of animal fat, protein with some cereals and plants thrown in (he was an omnivore).
We can then contrast the findings of Otzi’s diet with that of Neanderthals. It has been estimated that, during glacial winters, Neanderthals would have consumed around 74-85 percent of their diet from animal fat when there were no carbohydrates around, with the rest coming from protein (Ben-Dor, Gopher, and Barkai, 2016). Furthermore, based on contemporary data from polar peoples, it is estimated that Neanderthals required around 3,360 to 4,480 kcal per day to winter foraging and cold resistance (Steegmann, Cerny, and Holliday, 2002). The upper-limit for protein intake for Homo sapiens is 4.0 g/bw/day while for erectus it is 3.9 g/bw/day (Ben-Dor et al, 2011), and so this shows that Neanderthals consumed a theoretical upper-maximum of protein due to their large body size. So we can assume that Neanderthals consumed somewhere near 3800 kcal per day. The average Neanderthal is said to have consumed about 292 grams of protein per day, or 1,170 kcal (with a lower end of 985 kcal and an upper end of 1,170 at the high end) (Ben-Dor, Gopher, and Barkai, 2016: 370).
Then if we further assume that Neanderthals consumed no carbohydrates during glacial winters, that leaves protein as the main source of energy, since the large game the Neanderthals hunted were not around. Thus, Neanderthals would have consumed between 2,812 and 3,230 kcal from animal fat with the rest coming from protein. We can also put this into perspective. The average American man consumes about 100 grams of protein per day, while consuming 2,195 kcal per day (Ford and Dietz, 2013). For these reasons, and more, I argued that Neanderthals were significantly stronger than Homo sapiens, and this does have implications for racial differences in athletic ability.
In sum, the last meal of Otzi man is now known. Of course, this is a case of n = 1, so we should not draw too large a conclusion from this, but it is interesting. I don’t see why the composition of the diets of any of Otzi’s relatives would have been any different (or that the contents of his normal diet would have been any different). He ate a diet high in animal fat like Neanderthals, but unlike Neanderthals, they ate a more cereal-based diet which may have contributed to Otzi’s CVD and arterial calcification. We can learn a lot about ourselves and our ancestors through the analysis of their stomach contents (if possible) and teeth (if possible), and maybe even genomes (Berens, Cooper, and Lachance, 2017) because if we learn what they ate then we can maybe begin to shift dietary advice to a more ‘natural’ way and avoid diseases of civilization. But, we have not had time to adapt to the new obesogenic environments we have constructed for ourselves. It’s due to this that we have an obesity epidemic, and by studying the diets of our ancestors, we can then begin to remedy our obesity and other health problems.
Is Diet An IQ Test?
1350 words
Dr. James Thompson is a big proponent of ‘diet being an IQ test‘ and has written quite a few articles on this matter. Though, the one he published today is perhaps the most misinformed.
He first shortly discusses the fact that 200 kcal drinks are being marketed as ‘cures’ for type II diabetes. People ‘beat’ the disease with only 200 kcal drinks. Sure, they lost weight, lost their disease. Now what? Continue drinking the drinks or now go back to old dietary habits? Type II diabetes is a lifestyle disease, and so can be ameliorated with lifestyle interventions. Though, Big Pharma wants you to believe that you can only overcome the disease with their medicines and ‘treatments’ along with the injection of insulin from your primary care doctor. Though, this would only exacerbate the disease, not cure it. The fact of the matter is this: these ‘treatments’ only ‘cure’ the proximate causes. The ULTIMATE CAUSES are left alone and this is why people fall back into habits.
When speaking about diabetes and obesity, this is a very important distinction to make. Most doctors, when treating diabetics, only treat the proximate causes (weight, symptoms that come with weight, etc) but they never get to the root of the problem. The root of the problem is, of course, insulin. The main root is never taken care of, only the proximate causes are ‘cured’ through interventions, however, the underlying cause of diabetes, and obesity as well is not taken care of because of doctors. This, then, leads to a neverending cycle of people losing a few pounds or whatnot and then they, expectedly, gain it back and they have to re-do the regimen all over again. The patient never gets cured, Big Pharma, hospitals et al get to make money off not curing a patients illness by only treating proximate and not ultimate causes.
Dr. Thompson then talks about a drink for anorexics, called ‘Complan“, and that he and another researcher gave this drink to anorexics, giving them about 3000 kcals per day of the drink, which was full of carbs, fat and vitamins and minerals (Bhanji and Thompson, 1974).
The total daily calorific intake was 2000-3000 calories, resulting in a mean weight gain of 12.39 kilos over 53 days, a daily gain of 234 grams, or 1.64 kilos (3.6 pounds) a week. That is in fact a reasonable estimate of the weight gains made by a totally sedentary person who eats a 3000 calorie diet. For a higher amount of calories, adjust upwards. Thermodynamics.
Thermodynamics? Take the first law. The first law of thermodynamics is irrelevant to human physiology (Taubes, 2007; Taubes, 2011; Fung, 2016). (Also watch Gary Taubes explain the laws of thermodynamics.) Now take the second law of thermodynamics which “states that the total entropy can never decrease over time for an isolated system, that is, a system in which neither energy nor matter can enter nor leave.” People may say that ‘a calorie is a calorie’ therefore it doesn’t matter whether all of your calories come from, say, sugar or a balanced high fat low carb diet, all weight gain or loss will be the same. Here’s the thing about that: it is fallacious. Stating that ‘a calorie is a calorie’ violates the second law of thermodynamics (Feinman and Fine, 2004). They write:
The second law of thermodynamics says that variation of efficiency for different metabolic pathways is to be expected. Thus, ironically the dictum that a “calorie is a calorie” violates the second law of thermodynamics, as a matter of principle.
So talk of thermodynamics when talking about the human physiological system does not make sense.
He then cites a new paper from Lean et al (2017) on weight management and type II diabetes. The authors write that “Type 2 diabetes is a chronic disorder that requires lifelong treatment. We aimed to assess whether intensive weight management within routine primary care would achieve remission of type 2 diabetes.” To which Dr. Thompson asks ‘How does one catch this illness?” and ‘Is there some vaccination against this “chronic disorder”?‘ The answer to how does one ‘catch this illness’ is simple: the overconsumption of processed carbohydrates, constantly spiking insulin which leads to insulin resistance which then leads to the production of more insulin since the body is resistant which then causes a vicious cycle and eventually insulin resistance occurs along with type II diabetes.
Dr. Thompson writes:
Patients had been put on Complan, or its equivalent, to break them from the bad habits of their habitual fattening diet. This is good news, and I am in favour of it. What irritates me is the evasion contained in this story, in that it does not mention that the “illness” of type 2 diabetes is merely a consequence of eating too much and becoming fat. What should the headline have been?
Trial shows that fat people who eat less become slimmer and healthier.
I hope this wonder treatment receives lots of publicity. If you wish to avoid hurting anyone’s feelings just don’t mention fatness. In extremis, you may talk about body fat around vital organs, but keep it brief, and generally evasive.
So you ‘break bad habits’ by introducing new bad habits? It’s not sustainable to drink these low kcal drinks and expect to be healthy. I hope this ‘wonder treatment’ does not receive a lot of publicity because it’s bullshit that will just line the pockets of Big Pharma et al, while making people sicker and, the ultimate goal, having them ‘need’ Big Pharma to care for their illness—when they can just as easily care for it themselves.
‘Trial shows that fat people who eat less become slimmer and healthier’. Or how about this? Fat people that eat well and exercise, up to 35 BMI, have no higher risk of early death then someone with a normal BMI who eats well and exercises (Barry et al, 2014). Neuroscientist Dr. Sandra Aamodt also compiles a wealth of solid information on this subject in her 2016 book “Why Diets Make Us Fat: The Unintended Consequences of Our Obsession with Weight Loss“.
Dr. Thompson writes:
I see little need to update the broad conclusion: if you want to lose weight you should eat less.
This is horrible advice. Most diets fail, and they fail because the ‘cures’ (eat less, move more; Caloric Reduction as Primary: CRaP) are garbage and don’t take human physiology into account. If you want to lose weight and put your diabetes into remission, then you must eat a low-carb (low carb or ketogenic, doesn’t matter) diet (Westman et al, 2008; Azar, Beydoun, and Albadri, 2016; Noakes and Windt, 2016; Saslow et al, 2017). Combine this with an intermittent fasting plan as pushed by Dr. Jason Fung, and you have a recipe to beat diabesity (diabetes and obesity) that does not involve lining the pockets of Big Pharma, nor does it involve one sacrificing their health for ‘quick-fix’ diet plans that never work.
In sum, diets are not ‘IQ tests’. Low kcal ‘drinks’ to ‘change habits’ of type II diabetics will eventually exacerbate the problem because when the body is in extended caloric restriction, the brain panics and releases hormones to stimulate appetite while stopping hormones that cause you to be sated and stop eating. This is reality; these studies that show that eating or drinking 800 kcal per day or whatnot are based on huge flaws: the fact that this could be sustainable for a large number of the population is not true. In fact, no matter how much ‘willpower’ you have, you will eventually give in because willpower is a finite resource (Mann, 2014).
There are easier ways to lose weight and combat diabetes, and it doesn’t involve handing money over to Big Pharma/Big Food. You only need to intermittently fast, you’ll lose weight and your diabetes will not be a problem, you’ll be able to lose weight and will not have problems with diabetes any longer (Fung, 2016). Most of these papers coming out recently on this disease are garbage. Real interventions exist, they’re easier and you don’t need to line the pockets of corporations to ‘get cured’ (which never happens, they don’t want to cure you!)
The Genomic Health of Our Ancestors: What Was It Like and Is It Relevant for Us Today?
1500 words
After I published my article Thoughts On Diseases of Civilization: Romanticizing the Hunter-Gatherer’s Diet the other day, someone dropped by and stated that we are ‘getting healthier and healthier’, citing an article by Berens, Cooper, and Lachance (2017) titled “The genomic health of ancient hominins” who show, through genetic analyses, that many of our ancestors had the ‘genes for’ diseases that plague us today in our societies. While this may be true, one important thing that the individual who left the paper did not say is that genotypic health does not equal phenotypic health.
The basic assumption of the paper is this: They genotyped the Altai Neanderthal, Denisovans, pastoralists and hunter-gatherers and computed their ‘GRS’ (genetic [disease] risk score). When focusing on the GRS, they found that the Altai Neanderthal had 97 percent worse ‘genomic health’ when compared to the genomes of people today, whereas Otzi man had a ‘genetic predisposition’ to cardiovascular and gastrointestinal disease.
Something important to keep in mind here is that GRS and sequencing the genomes of ancient hominins can only ‘predict’ what types of problems one would have based on their genomes; it cannot realiably state that this individual would have gotten/did get a certain disease because he had the alleles for it.
What they did was genotype ancient hominins and then compute their GRS and compare the ancient hominins GRS to that of a modern human and then match the set of “disease loci to generate standardized GRS percentiles“. The ancient samples they tested had a similar genetic risk when compared to modern samples, though the ancient samples may underestimate their genetic risk since there are numerous other alleles yet to be discovered that may cause or add to genetic disease risk.
Ancient hominins had lower risks for cancer, miscellaneous diseases and neurological/psychological diseases when compared to modern humans. According to their analysis, ancient hominins only had a higher risk for cardiovascular disease while “Risks of allergy/autoimmune, morphological/muscular, metabolism/weight, and dental/periodontal diseases were not significantly different between ancient and modern hominins” (Berens, Cooper, and Lachance, 2017). So ancient hominins seemed to have a reduced risk of cancer, neurological disease and other unclassified diseases.
The Altai Neanderthal was at high risk of immunological diseases, cancers, gastrointestinal problems, morphological and muscular problems, and other metabolic disorders. However, and this is important, this is only what his genome showed. This is only a risk assessment and DOES NOT state anything about phenotypic health. The Altai Neanderthal, however, did have a lower GRS for cardiovascular disease and average risk for dental diseases. This is in contrast with Otzi man, who had a genetic risk for cardiovascular disease. Otzi also had a high GRS score on immuno-related diseases, gastrointestinal diseases and other metabolic disorders—which I would assume would be similar to type II diabetes mellitus. However, Otzi had ‘normal’ risk for morphological and neurological disease.
I had to wait all paper to read this:
We note that genomic health does not necessarily equate to phenotypic health. Genetic risk scores are not deterministic, instead they merely indicate whether an individual has a predisposition to a particular disease. In addition, alleles that contribute to disease in modern environments may not have had the same effects in past environments.
This makes it an open and shut case. Just because you have the ‘predisposition’ for something doesn’t mean that it will occur to you. For example, if someone has a ‘genetic predisposition’ to become and alcoholic and he never drinks alcohol, will he become an alcoholic? If someone is extremely sensitive to carbohydrate intake and more susceptible to the allure of sugar and more likely to get addicted to it, but they never eat the carbs will they become obese and insulin resistant? The genes-as-destiny paradigm is wrong—especially in regard to human disease. Human disease is extremely complex and doctors are even having problems with GWAS and what it shows for the genetic basis for disease.
Further, in regard to disease, GWAS has a huge problem in detecting genetic variants: “many GWAS hits have no specific biological relevance to disease and wouldn’t serve as good drug targets. Rather, these ‘peripheral’ variants probably act through complex biochemical regulatory networks to influence the activity of a few ‘core’ genes that are more directly connected to an illness.” See also Boyle and Pritchard (2017): An Expanded View of Complex Traits: From Polygenic to Omnigenic. Disease-nomics will be much more complicated than identifying one or a few genes; gene networks interact with the environment—whether by what we eat or our immediate surroundings—and diseases arise through a complex interaction between genes and environment: GxE.
When our ancestors made the transition from a hunter-gatherer lifestyle to a more sedentary, agricultural one, this is what then started up the environmental mismatch between humans and our environments. Agriculturalists had the highest GRS for dental caries and other problems to do with dentition, though the number of alleles was small, it makes logical sense for the advent of agriculture to increase the incidence of dental caries and other problems with dentition, which would then be selected for due to the change of lifestyle from mobile hunter-gatherer to relatively sedentary agriculturalist. Hunter-gatherers have fewer dental caries than agriculturalists. It is also argued that when we began to eat fermentable plant foods, that this caused “changes in food processing caused an early shift toward a disease-associated oral microbiota in this population” (Humphrey et al, 2014). Adler et al (2013) also show that “Data from 34 early European skeletons indicate that the transition from hunter-gatherer to farming shifted the oral microbial community to a disease-associated configuration.” Clearly, the transition from the mobile hunter-gatherer lifestyle to the sedentary agriculturalist one was extremely bad for our health and dentition.
Though agriculture did increase the incidence of dental caries, evidence exists that, through dietary shifts in the Upper Paleolithic, dental caries appeared, probably due to the shift to more processed foods (keep in mind that processing food only has to mean, say, mashing food to make it easier to chew, not in the modern definition of ‘processing’). Nevertheless, the first toothpicks were discovered from the Late Upper Paleolithic, which implies that some human populations encountered some foods that then gave them dental caries to which our ancestors responded by making toothpicks (Oxilia et al, 2015). Hunter-gatherers had few—if any—dental caries which implies that their lifestyles did not give them the oral disease. It’s very peculiar that these have only been noticed, really, in populations that underwent the agricultural transformation. That’s yet another ‘disease of civilization’ that is low to nonexistent in those populations, which is attributed to their lifestyle and their diet.
Cultural evolution drives mismatch diseases as cultural evolution can greatly outstrip Darwinian evolution. This, especially in regard to our health, is bad for us since we did not have the time to biologically adapt to our new, novel diets. We still have yet to adapt genetically to the diets and lifestyle taken on by our ancestors 10kya, and I think it will be a long time—if ever—before we do adapt. I mean come on, can you really see whole groups of people adapting to constant insulin spikes brought on by highly processed carbohydrates and other foods? We are the running ape, so do you ever see us adapting to constantly sit? These are modern problems, which were brought on by our ancestors’ adoption of agriculture. I agree with Jared Diamond when he says that farming was ‘the worst mistake in the history of the human race‘, but, obviously not for the Marxist reasons he proposes. Clearly, hunter-gatherers had better phenotypic health while ours suffers.
In sum, the paper Berens, Cooper, and Lachance (2017) does not refute anything that I wrote in my previous article on diseases of civilization. If anything, most of what I wrote is strengthened, especially on the basis of genotypic health not equalling phenotypic health. This paper can be summed with three points:
1) genes aren’t destiny. 2) genes wouldn’t necessarily do the same things in different environments. 3) the GRS (genetic [disease] risk scores) are also not deterministic. This is the logical conclusion to draw. OK, so ancient hominins had a higher genetic risk for certain diseases. Here’s the catch: if they weren’t in the environments that would exacerbate the disease and cause it to express in the phenotype, does it really matter that they had ‘genetic predispositions’ for certain diseases? Of course it matters for us today due to our built food environments, but did it matter for them who did not have access to the novel environments that we do today?
This is a very interesting paper but my arguments on diseases of civilization still stand. Diseases of civilization will still plague our societies until we change the built food environment, but until then, we will have to live with the worst mistake we have made as a species: constructing obesogenic environments that then lead to a huge decrease in quality of life and life expectancy.
Diet and Exercise: Don’t Do It?
1800 words
On Twitter, JayMan linked to a video about a time traveling dietician who travels back to the 70s to give nutritional advice to a couple. He kept going back on what he said, re eggs and cholesterol, Paleo diet, etc. Then at the end of the video, the ‘time traveling dietician’ says “It turns out it’s genetic. It doesn’t matter whether you exercise or what you eat.”
I then asked JayMan if he was advising people to not diet or exercise—and if he was doing so—what credentials does he have to give such advice? “Appeal to authority!” So if some random guy gave me legal advice and I asked his credentials, is that an appeal to authority? Similarly, if someone is trying to give me medical advice, is asking where he got his medical license an appeal to authority? The thing is, people have specialties for a reason. I wouldn’t take diet and exercise advice from some anon blogger with no credentials, just like I wouldn’t take legal advice from a biologist. Anyway, I’ll review some studies on exercise, dieting, and sitting in regards to all-cause mortality.
Sitting and all-cause mortality
Listening to such advice—like not dieting or exercising—will lower your quality of life and life expectancy. The longer you sit, the more likely you are to have rolled shoulders among other postural imbalances. One of the biggest reasons that sitting is related to all-cause mortality (Chau et al, 2013; Biddle et al, 2016). So listening to this shitty advice to ‘not exercise’ will lead an individual to having a lower QoL and lower life expectancy.
Sitting is associated with all-cause mortality because if, say, one is sitting at a desk for 8 hours per day then goes home and sits for the rest of the day, circulation will not get not get to the lower extremities. Furthermore, even mild-to-moderate exercise attenuates the situation (Chau et al, 2013). Further, reducing sedentary behavior (and of course, watching less TV) can possibly raise life expectancy in the US (Katzmarzyk and Lee, 2012). They found that cutting daily sitting time to less than three hours can increase life expectancy by two years (and, of course, quality of life). There is a large body of research on sitting and all-cause mortality (Stamatakis et al, 2013). It’s also worth noting that too much sitting decreases life expectancy—even with exercise. So JayMan’s (unprofessional) advice will lead to someone having a shitty life quality and lower life expectancy.
Dieting, and all-cause mortality
This is a bit trickier. I know that dieting for weight loss doesn’t work (Aamodt, 2016; Fung, 2016)—that is, traditional dieting (high-carb diets). The traditional advice is to eat high-carb, low-fat and moderate protein—this is due to what occurred in the 70s—the demonization of fat and the championing of carbs. This, clearly, is wrong. This has led to the obesity epidemic and the cause is our evolutionary novel environments. The main reason is that we have constructed environments for ourselves that are novel, and thus we’ve not had enough time to adapt to what we eat/how we live our new lives in our modernized world.
Indeed, even hunter-gathers don’t have our disease rates that we have—having low to no cases of our diseases of civilization (see Taubes, 2007 for a review). Why is this? It’s because they are physically active and they do not eat the same processed carbohydrates that we in first-world societies do.
In regards to exercise and all-cause mortality, people who exercise more often have a lower chance of dying from all causes than more sedentary people (Oja et al, 2016; O’Donovan et al, 2017). So it’s becoming clear that JayMan is just talking out out his ass here. I’d love to hear any MD say to a patient “Don’t diet, don’t exercise. Don’t eat well. It doesn’t work.” Because that MD will be a shill for Big Food.
Further, when I say ‘diet’, I don’t mean eating below the BMR. Your ‘diet’ is what you eat, and by changing your diet, you’re changing to healthier habits and eating higher-quality foods. People like JayMan make it seem like you should eat whatever you want and not to exercise. Following this advice, however, will lead to deleterious consequences.
It DOES matter what you put into your body; it DOES matter if you exercise or not. If you do not, you will have a lower life expectancy than who does exercise and eats well.
On a side note, I know that dieting does not work for weight loss. Traditional dieting, that is. Dr. Jason Fung, world-renowned obesity, diabetes and intermittent fasting expert, has people lose and keep their weight off. He actually understands what causes obesity—insulin. Higher insulin levels are also tied to the obesity pathway through lack of glucagon receptors (Lee et al, 2014). Why is this important? First, we have to understand what insulin does in the body. Once you understand what insulin does in the body then you will see why JayMan is wrong.
Insulin inhibits the breakdown of fat in the adipose tissue by inhibiting the lipase that hydrolyzes (the chemical breakdown of a compound due to a reaction with water) the fat out of the cell. Since insulin facilitates the entry of glucose into the cell, when this occurs, the glucose is synthesized into glycerol. Along with the fatty acids in the liver, they both are synthesized into triglycerides in the liver. Due to these mechanisms, insulin is directly involved with the shuttling of more fat into the adipocyte. Since insulin has this effect on fat metabolism in the body, it has a fat-sparing effect. Insulin drives most cells to prefer carbohydrates for energy. Putting this all together, insulin indirectly stimulates the accumulation of fat into the adipose tissue.
Does this physiologic process sound that you can ‘eat whatever you want’? Or does it tell you that you should lower your carb intake as to not induce blood glucose spikes which lead to an increase in insulin? Over time, these constant blood glucose/insulin spikes lead to insulin resistance which has the body produce more insulin due to the insulin resistance resulting in a vicious cycle.
So, it seems that in order to have a higher QoL and life expectancy, one must consume processed carbs very sparingly.
These behaviors of over consuming processed carbohydrates come down to the environments we have constructed for ourselves—obesogenic environments. An obesogenic environment “refers to an environment that helps, or contributes to,
obesity” (Powell, Spears, and Rebori, 2010).
Our current obesogenic environment also contributes to dementia and cognitive impairment. What makes environments ‘obesogenic’ “is the increased presence of food cues and the increased consumption of a diet which compromises our ability to resist those cues” (Martin and Davidson, 2015). So if our obesogenic environments change, then we should see a reduction in the number of overweight/obese people.
Diet is very important for Type II diabetics. For instance, TII diabetics can manage, and even reverse, their disease with a low-carb ketogenic diet (LCKD) lowering their hBA1c, having a better lipid profile, cardiac benefits, weight loss etc (Westman et al, 2008; Azar, Beydoun, and Albadri, 2016; Noakes and Windt, 2016; Saslow et al, 2017). I wonder if JayMan would tell TII diabetics not to diet or exercise…. That’d be a recipe for disaster. TII diabetics need to keep their insulin down and eating an LCKD will do that; taking JayMan’s ‘advice’ not to diet or exercise will quickly lead to more weight gain, an exacerbation of problems and, eventually, death due to complications from not correctly managing the disease. JayMan needs to learn the literature and understand these papers to truly understand why he is wrong.
Exercise and all-cause mortality
The relationship between vigorous exercise and all-cause mortality is well studied. Gebel et al (2015) conclude that “Independent of the total amount of physical activity, engaging in some vigorous activity was protective against all-cause mortality. This finding applied to both sexes, all age categories, people with different weight status, and people with or without cardiometabolic disease.” Reduced exercise capacity also causes higher all-cause mortality rates (McAuley et al, 2016).
Unfit thin people had two times higher mortality rate than normal weight fit people. Further, overweight and obese fit people had similar mortality rates when compared to normal weight fit people (Barry et al, 2013). Clearly, physical activity needs to be heightened if one wants to live a longer, higher quality life. This runs completely opposite of what JayMan is implying.
Exercise into old age is also related to higher cognition and lower mortality rate in when compared to individuals who do not exercise. Exercise also protects against cognitive degeneration in the elderly (Bherer, Erikson and Lie-Ambrose, 2013; Carvalho et al, 2014; Paillard, 2015). If you want to keep your cognition into old age and live longer, it seems like your best bet is to exercise at a young age in order to stave off cognitive degeneration.
Strength and mortality
Finally, one last thing I need to touch on is strength and mortality. Strength is, obviously, increased through exercise. Stronger men live longer—and are protected from more disease such as cancer—than weaker men, even when controlling for cardiorespiratory fitness and other confounds (Ruiz et al, 2008).
As I have covered in the past, differences in grip strength account for differences in mortality in men—which also has a racial component (Araujo et al, 2010; Volkalis, Halle, and Meisinger, 2015). The stronger you are, the less chance you have of acquiring cancer and other maladies. Does the advice of ‘don’t exercise’ sound good now? It doesn’t, and I don’t know why anyone would seriously imply that dieting and exercise doesn’t work.
Conclusion
Dieting (meaning eating a higher quality diet, not attempting to lose weight) and exercise do work to increase life expectancy. The advice of “don’t do anything, it’s genetic” makes no sense at all after one sees the amount of literature there is on eating mindfully and exercising. I know that exercise does not induce weight loss, but it does contribute to living longer and staving off disease.
People should stay in their lane and leave things to the professionals—the people who are actually working with individuals every day and know and understand what they are going through. The canard of ‘eat whatever, don’t exercise, it’s genetic’ is very dangerous, especially today when obesity rates are skyrocketing. JayMan needs to learn the literature and how and why exercise and eating right leads to a higher quality of life and life expectancy. Thankfully, people like JayMan who say not to diet or exercise have no pull in the real world.
Clearly, to live longer, eat right, don’t sit for too long (because even if you exercise, sitting too long will lower your life expectancy) and exercise into old age and your chance of acquiring a whole slew of deleterious diseases will be lessened.
Rebutting Heartiste on the Twinkie Diet
1300 words
Nutritional myths run amok everywhere. One of the most persistent is that ‘a calorie is a calorie’, that is, every macronutrient will be processed the same by the body. Another assumption is that the body doesn’t ‘care’ about where the calories come from—they can come from fat, protein, or carbs and the response will be the same: bodyweight will be reduced until one reaches their goal. However, it’s not as simple as that. He also has the assumption that “diets work”, when the best meta-analysis I know of on the matter shows the opposite (Mann et al, 2007, see especially table 1). They control for studies where weight was self-reported. They conclude that dieting does not work. This is what, as Heartiste says, “iScience!” says on the matter, so he should believe everything I state in this article, which is backed by “iScience!”.
Chateau Heartiste published an article back in 2010 titled The Twinkies Diet Proves Fatty Fats Are Fat Because They Eat Too Much. He is referring to professor of human nutrition Mark Haub and his success on ‘the twinkies diet’, where 2/3rds of his caloric intake came from junk food such as Twinkies. He lost 27 pounds in a two month period while his LDL cholesterol decreased by 20 percent and his HDL cholesterol increased by 20 percent. His level of triglycerides also decreased by 37 percent, with his body fat decreasing from 33.4 to 24.9 percent. So he ate 1800 kcal per day—2/3rds of it being junk food—for two months and lost 27 pounds. Case closed, right? Eat junk food at a deficit and lose weight? A calorie is a calorie? There are a few problems with this contention which will be addressed below.
Heartiste writes:
Big bottom line: Being fat itself is bad for your health. “Fat and fit” is a myth. The change that counts the most is losing the weight, which can only be done by PUSHING AWAY FROM THE TABLE.
Except fit and overweight and obese individuals have similar mortality rates than their normal weight counterparts (Barry et al, 2014). However, more recently a study was published purporting that overweight and obese individuals being healthy despite excess weight is a myth. The researchers state that in a sample of millions of Britons that overweight and obese individuals had a higher risk of heart disease than their normal-weight counterparts. Unfortunately, I cannot locate the study since it wasn’t published in a journal (and thusly not peer reviewed). I wonder if variables such as diet, smoking and other lifestyle factors were taken into account. Nevertheless, the debate on fitness and fatness continues.
Another large meta-analysis shows that grade 1 obesity (BMI 30->35) had the same mortality risk as normal-weight individuals with grade 2 obese (BMI +35) having a significantly higher risk of death (Flegal, Kit, and Orpana, 2013).
Heartiste claims that ‘a calorie is a calorie’. This is a common fallacy. This suggests that the body will process all foods the same way—that is, processing them the same metabolically. This, however, is not the case. Haub himself is a sample size of 1. If Heartiste can use a sample size of 1 to make a claim, then I can too.
Sam Feltham ate +5,000 kcal per day for 21 days and only gained 1.3 kg when he should have gained 7.3 kg based on the amount of kcal he ate. A calorie is a calorie, right? This is a fallacious statement. The statement “a calorie is a calorie” violates the second law of thermodynamics (Feinman and Fine, 2004). Heartiste writes:
That first law of thermodynamics looms large over everything.
The first law of thermodynamics is irrelevant to human physiology. It only states that an organism gets bigger if it consumes more energy; it doesn’t state why this occurs, which is due to the hormone insulin which causes weight gain.
He does rightly state that an omega 3/6 imbalance is part of the reason but then handwaves it away. Western-like high-fat diets (i.e., diets with an imbalance of linoleic acids (LA; and n-6 fatty acid) with n-3) are sufficient enough to induce gradual enhancement in fat mass across the generations (Massiera et al, 2010). This obviously includes the average 55 percent carbohydrate diet that the AHA recommends (Eckel et al, 2014). The Standard American Diet (aptly named the “SAD diet”) has the n-3/n-6 imbalance along with being high in carbohydrates which spike insulin which impedes fat being unlocked from the adipocyte.
Heartiste doesn’t understand that if you reduce the ‘in’, the ‘out’ also decreases. This was noted in the famous starvation experiment headed by Ancel Keys. They took 36 healthy men who ate normally for three months while being their behavior and personality was monitored. In the next six months, they were reduced to eating half of their initial intake (they started at 2000 kcal and dropped to 1000 kcal; some individuals going lower than that) and their metabolic rate decreased by 40 percent (Keys et al, 1945). This is proof for the contention that the body decreases its metabolic rate due to what is ingested. A similar study was done on Vermont prisoners, except they were told to gorge on food. Since they were in a controlled setting, the prisoners could be monitored to ensure they ate all of the food.
At the end of the study, their metabolic rates had increased by 50 percent. This is evidence that the body was trying to get back to its original weight. In six months, the prisoners went back to their normal weight as they ate normally (Salas, Horton, and Sims, 1971) One man only gained ten pounds eating all of those calories. Clearly, the body was resisting weight gain and when they were allowed to eat normally, they effortlessly regained their normal weights.
Finally, on the topic of Haub, Big Food shill, I will address a few things about him and his ‘research’ that recently came to light.
Intermittent fasting and obesity expert Dr. Jason Fung showed that in 2016 after Coca-Cola released their funding reports after criticisms of transparency, Mark Haub was found to be one of the many researchers that were backed by Coca-Cola. This is an attempt to show that ‘a calorie is a calorie’ and that ‘all calories are created equal’. This has been rebutted above.
In 2016—six years after his ‘experiment—it was revealed that he was funded by Coca-Cola. No doubt in order to ‘prove’ that ‘a calorie is a calorie’ and have people continue to gorge on high carbohydrate/insulinogenic foods. However, the human body is a lot more complex than to just reduce it to simply calories in and calories out—which I have written about in depth.
People like Heartiste need to get an actual understanding of the literature and what Coca-Cola has been trying to do for years, which is to make eating junk food ‘OK’ because ‘it doesn’t cause obesity’. Children consume 45 percent more food when exposed to advertisements (Harris, Bargh, and Brownell, 2009). So to begin to curb obesity rates we don’t need to ‘eat junk food’, we need to not eat junk food and eat a diet more ancestral to us—that is, one lower in processed carbs and higher in animal fat and protein. Big Food shills like Haub need to be exposed for what they are—people who do ‘research’ for a quick buck, i.e., not furthering our understanding of a complex issue as he would like you to believe. Exercise also doesn’t induce weight loss. So the claims of ‘eat less and move more’ (eat less according to the 55 percent carbohydrate recommendations) is bound to fail.
If Heartiste can make a claim using one man as an example then so can I. Read the above article by Sam Feltham in which he writes about hs experience eating 5,000 kcal per day for 21 days while only gaining 1.3 kg. I can use this example to say that eating low carb and high fat at 5,000 kcal per day will lead to negligible weight gain, however, I don’t use n=1 sample sizes to make claims and no one else should either.
Are Flynn Losses in France Due to Immigration?
1850 words
Over a ten year period in France, from 1999 to 2008-9, IQ has declined in France by almost 4 points. What is the cause? Immigration? Dysgenics? A reversal of the Flynn Effect? No doubt that numerous people would attribute the decline in intelligence in France due to MENA and SSA immigration. But is this true?
Lynn and Dutton (2015) show how differing studies show both positive and negative gains in IQ. To prevent further evidence of these negative Flynn gains, they looked to the IQ of France from 1999-2009.
The WAIS-III was standardized in France in 1999 while the WAIS-IV was standardized in 2009. This was a great opportunity to see if the intelligence of the French dropped using the new WAIS-IV. The sample was of 79 people who were of a different sample than that of the broader WAIS-IV French standardization. The average age of the sample was 45, ranging between 30 and 63 years of age. Half of this sample took the WAIS-IV first while the other half took the WAIS-III first to control for practice effects. They used a separate sample to compare the norms of generated by the two standardizes samples.
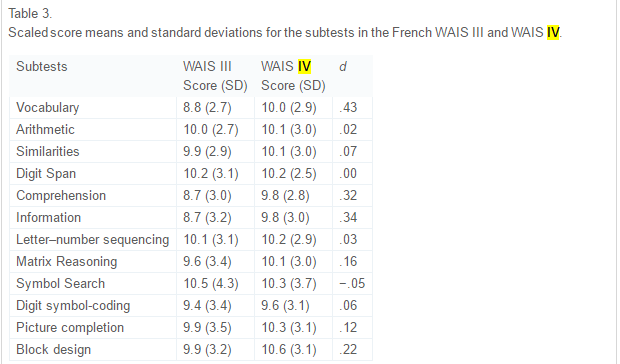
The above table from the paper, table 3, shows the comparison between the two WAIS tests. Positive ds indicate lower scaled scores on the III in comparison to the IV and thusly higher scores. What these data show is that the IV is harder than the III and IQ declined because the test got ‘tougher’ (because full-scale intelligence declined). As noted above, this phenomenon of decreasing IQ scores has been noticed for about 20 years now. The symbol search showed the smallest decline while there was no change in digit span. The biggest gain was in vocabulary.
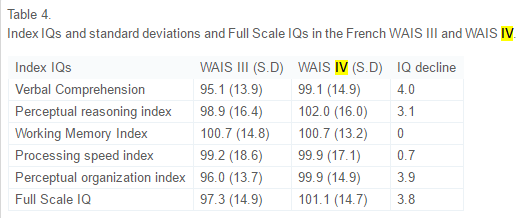
This is pretty shocking. In ten years, verbal comp decreased by 4 points, perceptual reasoning index by 3.1 points, no change in working memory index, processing speed index decreased by .7 points, perceptual organization index decreased by 3.9 and the whole full-scale IQ decreased by 3.8 points. Lynn and Dutton discuss the results:
In addition, the Full Scale IQ on the WAIS IV sample of 79 subjects was calculated based on a comparison with the WAIS IV sample of 876 subjects, which was representative of the French population on key variables such as education and region. The scores of this sample of 876 subjects were set at 100 and a comparison made with the sample of 79 subjects. As can be seen in Table 4, on this basis the IQ of the sample of 79 subjects was 101.1 with an SD of 14.7, where the French norm would be 100 and the SD 15. As such, the smaller sample can be regarded as representative of the French population in terms of intelligence.
So this small sample can be regarded as representative of the French population. Lynn and Dutton say that the digit span showing no increase corroborates findings from another researcher that showed that there was no change in forward or backward digit span in 85 years. They then say:
. . .improvements in the quality of nutrition during the twentieth century made a major contribution to increasing IQs. But it seems improbable that the quality of nutrition declined in recent years in France and in the other economically developed countries in which declining IQs have been reported.
So one possible cause is that nutrition has declined in France. From Dubuisson et al, 2010:
These repeated surveys highlighted the fact that trends in French food habits have moved towards an average European diet at the crossroads between Mediterranean and Northern diets, and that food consumption changes impacted, to a lesser extent, nutritional intake.
It shows that the French diet is in between Med and Nord diets. Really, as Lynn and Dutton asserted, there was no decline in nutritional quality for the French.
Another possible cause is a decrease in quality of schools. Flynn says a part of the reason for the rise in IQ was due to the advent of scientific thinking. However, this is not a good explanation either since school quality seems to not have been affected.
Flynn also talks about the media and its role. Lynn and Dutton say:
However, this would not explain declines in other forms of intelligence and, moreover, it might be argued that the desire and ability to read such literature would be underpinned by general intelligence and so a decline in the consumption of such literature would partly reflect a decline in general intelligence, as vocabulary is a measure of intelligence.
It is also worth noting that, apparently, reading may actually increase general intelligence (post coming on that soon).
Now, finally, the theory we’ve all been waiting for: Is it increased immigration?
Lynn and Dutton state:
This increase has occurred throughout western Europe and a number of studies have shown that immigrants from North Africa and south-west Asia typically have an average IQ of around 85 to 90 (Lynn, 2006, Lynn, 2008, Lynn and Vanhanen, 2012 and Rindermann and Thompson, 2014; for a large meta-analysis see te Nijenhuis, de Jong, Evers, & van der Flier, 2004). This conclusion has been confirmed by Kirkegaard (2013) who has shown that in Denmark the number of non-European immigrants increased from approximately 50,000 in 1980 to 400,000 in 2012 and the IQ of non-European immigrants in 18–19 year old military conscripts was 86.3, relative to 100 for indigenous Danes. These immigrants are likely to have had some impact on reducing the average IQ of the populations, but it is doubtful whether the increase in the number of immigrants with lower IQs has been sufficiently great to have had a major effect.
I personally don’t think that migration into Europe from MENA and SSA countries has been enough to put that big of a dent (over 1/3rd of an SD) in average IQ in France, and Europe as a whole. Since people are coming from areas closer to the equator and have higher rates of children since they are r-selected, could this be why France has seen a decrease in intelligence?
No.
Woodley of Menie and Dunkel (2015) reviewed Lynn and Dutton’s paper and said:
Replacement migration in France involving populations exhibiting lower means of IQ and higher rates of total fertility, such as Algerians, Moroccans, Tunisians and Roma (Čvorić, 2014 and Lynn and Vanhanen, 2012) may be increasing the rate of secular losses at the level of g, consistent with speculations advanced in Dutton and Lynn (2015), however the additional loss in g due to this process is anticipated to be very small. Based on a simulation, Nyborg (2012) estimates that in Denmark, replacement migration may be reducing heritable g by .28 points per decade, which would increase the overall loss in g to 1.51 points per decade ( Woodley of Menie, 2015), this still being only 37.75% of the loss observed in the French cohort.
An Environmental Explanation?
Since we still need an explanation for 62.25 percent of the 3.8 decrease in full-scale IQ other than dysgenic fertility, are there any environmental explanations? Environmental explanations can be anything from child abuse, to poor schooling, to poor nutrition, etc. Was there an increase in any of these or other variables that negatively affect IQ which would explain the 3.8 point decline in IQ?
One of the most likely candidates is nutrition. Lack of certain vitamins, especially in childhood, would prevent the brain from receiving the proper nourishment to grow.
The INCA study took record of food consumption from 2,373 people aged 4 to 92 from a 7-week period and from that they saw which nutrients they were deficient in (Touvier et al 2006). To measure if and how much they were nutrient deficient, they used the Estimated Average Requirement (EAR). The vitamins used were calcium, magnesium, iron, vitamins C, A, B6, and B12, thiamin, riboflavin, niacin, pantothenic acid, and folate. A lot of these have to do with proper brain functioning and ability to reach its full-size potential. For instance like the B vitamins and iron. Being deficient in those nutrients depresses brain size and with it IQ. For instance, being deficient in vitamin B 12 and folate leads to decreased brain size in childhood. The negative effects of being deficient in these nutrients may partially explain some of the 3.8 point decrease in full-scale IQ.
Regarding the prevalence of the aforementioned nutrient deficiencies in these populations, the authors state:
We also calculated daily consumption of 44 food groups by age and gender. This paper shows how the combination of both data sets, i.e., inadequacy and food consumption data, allows a preliminary screening of potential food vehicles in order to optimize fortification. The prevalence of inadequacy was particularly high for the following groups: for calcium, females aged 10-19 years (73.5%) or aged 55-90 years (67.8%), and males aged 15-19 years (62.4%) or aged 65-92 years (65.4%); for magnesium, males aged 15-92 years (71.7%) and females aged 10-90 years (82.5%); for iron, females aged 15-54 years (71.1%); and for vitamin C, females aged 15-54 years (66.2%). Two examples are provided to illustrate the proposed method for the optimization of fortification.
Most vitamins and minerals have positive effects on brain functioning, some more than others, but notice the prevalence of iron defieciency in the females aged 15-54 years (71.1 percent). With the cohort cited by Lynn and Dutton (2015) and Woodley of Menie and Dunkel (2015) being aged 30 to 63 with an average age of 45, the prevalence of iron deficiencies in the INCA study, along with the other deficiencies in the cohort, may partially be responsible for the decline in IQ.
The Flynn Effect
PumpkinPerson describes it well here:
One of the biggest mysteries in psychology is the Flynn Effect; the fact that over the 20th century, people have been performing better and better on IQ tests. Of course, the average IQ in Western countries by definition is always about 100, however because people keep scoring higher every decade, the tests routinely have to be made more difficult and the norms must be regularly updated to keep the mean IQ from rising far above 100.
However, in first-world countries, in the past 20 or so years, it has been in decline, particularly in France. It’s due to a mix of dysgenic fertility and nutrient deficiencies. Since Flynn gains are largely due to advancements in better nutrition, Flynn loses would then be attributed in part to nutrient deficiencies as well as dysgenic fertility.
The cause for the 3.8 decrease in IQ in France is low fertility rates amongst the French population as well as nutrient deficiencies. Clearly, ameliorating this decrease in IQ can be reversed by the K-selected having more children and healthier eating habits. Drops in IQ won’t be attributed to MENA and SSA populations until the future, but for now, the cause for the decrease is the French themselves.
HBD and Diet Advice: Anglin Paleo Refutation Part 2
2300 words
A lot of people seem to have wrong views on nutrition. It’s not really taught in school, people think that it doesn’t matter so they do no independent research of their own and they believe anything and everything that comes out in the MSM as gospel. The thing is, the average person doesn’t read studies, or anything nutrition related for that matter, and believes most everything they read and hear in the MSM. I have talked about nutrition a bit here. I refuted Andrew Anglin’s atrocious writing and arguments for the Paleo Diet here and wrote on obesity and ethnicity including genetic and environmental causes. I also wrote on how nutrition is important prenatally as well as postnatally in developing children. I will also touch on comments in that Dailystormer article that jump out to me that need refuting.
Today I will talk about HBD and diet advice.
Steve Sailer wrote an article on HBD and Diet Advice back in September. He claims a few things that need to be disproven.
It’s common for nutrition scientists to give advice to white Americans based on studies done of what is good for nonwhites to eat. For example, in the 1980s, one of the most fashionable studies was of Japanese in Hawaii. The first generation ate mostly rice with little fat, and they had relatively few heart attacks. The next generation ate cheeseburgers and had higher rates of coronary disease than their parents.
I have covered this in the Dailystormer refutation.
Noted in this study are:
- High interpersonal variability in post-meal glucose observed in 800-person cohort
- Using personal and microbiome features enable accurate glucose response prediction
- Prediction is accurate and superior to common practice in an independent cohort
- Short-term personalized dietary interventions successfully lower post-meal glucose
You can see from the above bullet points that there is high interpersonal variability in post-meal glucose. What that means is, that between each individual in the cohort, there were different glucose spikes in each person.
They can accurately predict glucose response with certain tools. They devised a machine-learning algorithm that uses blood parameters, dietary habits, anthropometrics, physical activity, and gut microbiota measured in the cohort and showed that it accurately predicted personalized postprandial (post-meal) glycemic response to real-life meals.
They validated the prediction using a 100 person cohort.
Personalized dietary interventions showed interventions successfully lowered post-meal glucose. (Emphasis mine). This shows that each person should be on an individual diet and not on a one-size-fits-all diet.
Of course the next generation had higher rates of coronary disease than their parents. High carb, high fat diets lead to coronary blockage, leading to heart attacks and other coronary implications.
That is due to the demonization of fat starting in the 70s. We were told that fat is bad and carbs were fine. That turned out not to be the case. That’s what led to the obesity explosion. People think that eating fat “makes you fat”. Well if that’s the case, eating protein leads to kidney failure and eating carbs leads to Diabetes Mellitus. It’s stupid to think of it that way. Anything in excess is bad for you.
The RDA (Recommended Daily Values) for women is as follows:
69 grams of fat, which comes out to 585 kcal, 300 grams CHO which comes out to 1200 kcal and 53 grams of protein which comes out to 215 kcal. For men, it’s 80 grams of fat which comes out to 720 kcal, 375 grams CHO which comes out to 1500 kcal and 70 grams of protein which comes out to 280 kcal. This is data from the FDA on dietary recommendations for the average America.
Protein is nowhere near high enough. Protein is the main macronutrient you want to eat if you want to stay fuller longer as it has a higher TEF (Thermic Effect of Food). In the linked study, they come to the conclusion that TEF contributed to the satiating power of foods. Protein has the highest TEF of all of the macros, and because of this, some researchers have lobbied to have protein count as 3.2 kcal instead of 4 kcal. So if you want to stay fuller, eat more protein, fewer carbs and more fat. Carbs spike your insulin leading to insulin spikes, which lead to you feeling hungry sooner, as most people ingest fast digesting carbohydrates.
Sailer then cites this NYT article that says:
Today, at least 10 percent of Americans regularly take fish oil supplements. But recent trials have failed to confirm that the pills prevent heart attacks or stroke. And now the story has an intriguing new twist.
Wrong. So, so wrong. Controlled studies clearly show that omega-3 consumption had a positive influence on n-3 (fatty acid) intake. N-3 has also been recognized as a modulator of inflammation as well as the fact that omega-3 fatty acids down-regulate genes involved in chronic inflammation, which show that n-3 is may be good for atherosclerosis.
Studies have shown an increase in omega-3 consumption leads to decreased damage from heart attacks.
Omega-3 may also reduce damage after a stroke.
Dietary epidemiology has also shown a link between n-3 and mental disorders such as Alzheimers and depression. N-3 intake is also linked to intelligence, vision and mood. Infants who don’t get enough n-3 prenatally are at risk for developing vision and nerve problems. Other studies have shown n-3’s effects on tumors, in particular, breast, colon and prostate cancer.
Omega-3’s are also great for muscle growth. Omega-3 intake in obese individuals along with exercise show a speed up in fat-loss for that individual.
Where do these people get their information from? Not only are omega-3’s good for damage reduction after a stroke and a heart attack, they’re also good for muscle growth, breast, colon and prostate tumor reduction, infants deficient in omega-3 prenatally are at risk for developing nerve and vision problems. Increase in omega-3 consumption is also linked to increases in cognition, reduces chronic inflammation and is linked to lower instances of depression.
Omega-3’s are fine. As I said with the Anglin refutation, do not listen to those with no background in nutrition as they most likely have no idea what they are talking about.
Rasmus Nielsen, a geneticist at the University of California, Berkeley, and an author of the new study, said that the discovery raised questions about whether omega-3 fats really were protective for everyone, despite decades of health advice. “The same diet may have different effects on different people,” he said.
See above links on omega-3 intake and all of the positive/negative factors.
In the future, maybe you’ll be able to get your DNA analyzed and be given a list of diets in rank order of their likelihood that they will work for you. But, right now, you can still try different diets. In particular, ask your relatives about what has worked and not worked for them.
That doesn’t matter, as diets should be tailored to the individual, as seen in the Cell study.
Oh, wow. I just found that Anglin wrote a refutation to those who deny the Paleo Diet. Let’s see what that’s about.
And maybe these people have scientific research and/or personal experience to back up what they’re saying. I’m not insulting them for disagreeing with me on diet, that is clearly their right.
The evolutionary argument for Paleo does not line up with your statements. As I noted in my previous article, if you want to eat Paleo because it works with what you like to eat, good for you. But doing it for any magic benefits is stupid, as there are none.
I know for a fact that at least 9 out of 10 people who dare to take this challenge will report back positively if they follow it properly for a month, and this means a whole lot more than someone’s opinion about what it might or might not do, theoretically.
Want to know why people will report back positively? Any time you begin a new diet, especially one on a kcal restriction, your body will drop weight quickly. That’s what piranha personal trainers use on unknowing people. Telling them that they’re doing a “great job”, when in actuality, that happens to everyone who begins a new diet.
Instead, they are arguing theoretically, making highly debatable statements like “White people have evolved to be able to consume dairy products.”
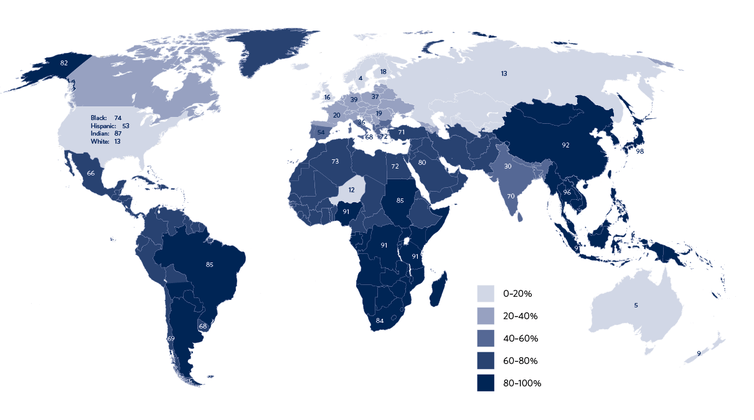
The above map shows lactose intolerance for countries around the world. Ancient Europeans began dairying around 7500 ya and were lactose intolerant when starting to drink milk. But along with faster evolution, which includes no gene flow from other parts of the world, that led to Europeans evolving to, on average, have lower rates of lactose intolerance.
People should really learn what they’re talking about before they say it.
The way to know whether or not they are beneficial is to quit them for a period and see how you feel.
Placebo effect.
Currently, because the scientific literature on these topics is so convoluted and debated on, there is no other conceivable way to prove it one way or another than through our own testing.
The science is pretty solid on this. Anecdotes don’t mean anything to studies.
Many have referred to paleo as a “fad diet.” And it may be a diet that is a fad, but it is also a diet with a thousands upon thousands of years long precedent. One might even suggest that it is the consumption of grains and dairy that are the “fad,” as it is a relatively new trend, in the scope of things.
It IS A FAD DIET ; with NO basis in science that Europeans should eat that way.
If you feel as if you are at peak physical health eating grains and dairy, and have no desire to spend time trying to improve on this, than by all means skip the challenge.
Is he implying that the Paleo Diet is the only diet that doesn’t allow grains and dairy? Not true at all. The Slow Carb Diet is the same, as well as any other high fat, high protein low-carb diet.
We should also note that the definitions of vegetarianism were different then, and Hitler did eat eggs and probably wasn’t completely meat-free.
That’s vegetarianism. Veganism is the more extreme one you’re thinking of where absolutely no animal products are consumed at all.
Vegetarian diets are shown to lead to vitamin inadequacies such as zinc, calcium, iron, manganese, selenium, and copper. Vegetarianism works, it just has to be well-planned. You need to make sure you get the right amount of essential as well as non-essential amino acids, high amounts of protein and make sure you’re not nutrient deficient.
Last time I wrote that White rice and potatoes are good carbs, but I want to be clear that they are not necessary unless you are both already at 5% body weight and you are highly active.
They are not ‘good carbs’. They are white carbs, which are bad for us if we don’t go to the gym to utilize the CHO being ingested. Five percent body-fat? That’s for competition bodybuilders and marathon and distance runners. The average person will never cut down to the level of body-fat. CHO is extremely useful if you’re highly active and go to the gym.
Even if you are not active, you need to consume a decent amount of carbs once a week in order to keep your metabolism from slowing down too much. However, it is probably preferable to use fruits for this purpose, as they contain more micronutrients.
Correct. If you eat a low-carb diet, you need a CHO refeed once a week to keep metabolism high. Though, using fruits is stupid. I know the Paleo thing, but there are many reasons why fructose (the sugar found in fruit) is bad for you. Sugar is just as addictive as cocaine. So telling the average person to ‘use fruits for this purpose’ is stupid, as the average person doesn’t know when to stop eating.
Yes, this diet will technically cost more than a processed foods and grain-based diet, all things being equal. The only reason anyone ever ate grains in the first place is because they were cheap, and processed foods were invented for the same reason. Any natural and healthy diet is going to cost more, all things being equal. However, things don’t have to be equal.
Wrong. Whole foods are not more expensive. The conclusion that was (obviously) reached is that there is expensive and non-expensive junk food as well as whole foods. I personally spend 70 dollars a week on food for myself, with all of my meals planned out. Natural diets will not cost more, all things being equal. If you know how to eat and how to buy food, you will avoid spending too much money.
I tried to answer most of the questions people had in the last thread, but it was so filled up with denialism I could have missed something. So ask here.
I hope you answer this, as well as my other refutation of your horrible nutrition article. I doubt it though.
How did we really evolve to eat?
The most common form of eating, 3 meals a day, is abnormal from an evolutionary perspective. We didn’t evolve eating 3 times a day. We evolved eating intermittently. The study says that intermittent energy restriction periods of up to 16 hours are fine. Long-term calorie restriction is highly effective in reducing the risk for atherosclerosis in humans. Again, another huge benefit for intermittent fasting. As the data comes out on human cohorts, we will be able to see all of the great effects that IF has for us, because that’s how any human population, no matter where they evolved, evolved eating.
There are beneficial effects to IF including reduced oxidative damage and increased cellular stress resistance. Rats put on an IF diet show heightened life-spans. IF is also extremely useful to keep a youthful brain as you age.
There are a mountain of studies that show how beneficial IF is to us and is the TRUE way humans evolved to eat, not any specialized diets. We evolved eating intermittently, and with our hedonistic society we live in now, along with low ability to delay gratification, as well as other factors I have covered in my previous nutrition articles, have led to the effects we see in America, and around the world today.
In conclusion, don’t listen to people who have no background in nutrition. They tell clearly wrong information, and those who aren’t privy to new information in the nutrition world, won’t know that they are being lied to and or manipulated into believing things based on shoddy evidence.
