
Home » Posts tagged 'Nutrition' (Page 2)
Tag Archives: Nutrition
Agriculture and Diseases of Civilization
2350 words
It is assumed that since the advent of agriculture that we’ve been better nourished than our hunter-gatherer ancestors. This assumption stems from the past 130 years since the advent of the Industrial Revolution and the increase in the quality of life of those who had the benefit of the Revolution. However, over a longer period of time, the advent of agriculture is linked to poorer health, vectors of disease and lower quality of life (in terms of intractable disease). Despite what I have claimed in the past about hunter-gatherer societies, they do have lower or nonexistent rates of the diseases that currently plague our first-world societies. Why do we have such extremely high rates of disease that they don’t?
Contrary to popular belief, agriculture has caused decreases in many facets of our lives. These diseases, more aptly termed ‘diseases of civilization‘ are directly caused by agricultural and societal ways of living. This increases disease rates as it’s easier for diseases to spread faster through bigger populations. Moreover, we haven’t had time to evolve to the current diet we now eat in first-world countries which has lead to what is termed an ‘evolutionary mismatch‘ between genes and environment. We evolved to eat a certain diet and the introduction of easily digestible carbohydrates which spike insulin the highest. Since insulin causes weight gain, and carbohydrate intake has dramatically increased since the 70s, obesity has increased as a result as countries begin to industrialize and more processed foods are available to the populace.
However, since the Industrial Revolution, height has increased along with IQ. Researchers argue that in first-world countries, high rates of obesity are not preventable due to the excess amounts of highly refined and processed foods. There is data for this theory. In first-world countries, the heritability of BMI is between .76 and .85. Since first-world countries are industrialized, we would expect them to hit their ‘genetic height and weight’ along with having the ability to reach their IQ potential. However, with the excess amount of highly processed and refined foods, this would also, in theory, have the population hit their ‘genetic weights’. This is what we see in first-world countries.
To see how first-world, industrialized societies cause these gene-environment mismatches, we can compare the disease acquisition rate—or lack thereof—to that of Europeans eating an industrialized, first-world diet (high in carbohydrates).
In his 2013 book The Story of the Human Body: Evolution, Health, and Disease, Paleoanthropologist Daniel Lieberman talks at length about evolutionary mismatches. The easiest way to think about this is to think about how one evolved to their environment and think how the processes that alter the environment. A perfect example is African farmers. They may dig a trench to divert water to better irrigate their crops, but this then would cause a higher rate of mosquitoes due to the increase in still water and then selection for genes that protect against malaria would be selected for. This is one example of an evolutionary mismatch turning into an advantage for a population. Most mismatch diseases are caused by changes in the environment which change how the body functions. In other words, the current first-world diet is correlated very highly with diseases of civilization and drive most of the mismatch diseases. Most likely, you will die from one of these mismatch diseases.
If you’re born in a hotter environment, you will have more sweat glands than if you were born in a cooler environment. If you grow up eating soft, processed food, your face will be smaller than if you ate harder foods. These are two ways in which ‘cultural evolution’ (cultural change) have an effect on how the human body grows and adapts to certain stimuli based on the environment around it.
The largest cause of the higher disease rate between industrialized peoples and those in hunter-gatherer societies is shifts in life history. As our life spans increased through modernization, so to did our chance of acquiring more diseases. Of course living longer affects how many children you have but it also raises your chances of acquiring an evolutionary mismatch and your chances of dying from one.
Daniel Lieberman writes on page 190 of his book The Story of the Human Body:
A typical hunter-gatherer adult female will manage to collect 2,000 calories a day and a male can hunt between 3,000 and 6,000 calories a day. (24) A hunter-gatherer groups combined efforts yield just enough food to feed small families. In contrast, a household of early Neolithic farmers from Europe using solely manual labor before the invention of the plow could produce an average if 12,800 calories per day over the course of a year, enough to feed families of six. (25) In other words, the first farmers could double their family size.
Thusly, you can see how evolutionary mismatches would occur with the advent of an agricultural diet that we didn’t evolve to be accustomed to. This is one of the biggest examples of the negative effects of agriculture, our inability to adapt quickly to our new diets which then accelerated after the Industrial Revolution. Further, hunter-gatherers will eat anything edible while agricultural societies will largely eat only what they grow. This would have huge implications for farmers if a few pests ruined their crops since they relied on a few crops to survive.
The thing about farming is that as the Agricultural Revolution began, this increased the population size as well as making that population pretty much stable in terms of migrating. This, then, led to higher rates of disease as larger populations foster new kinds of infectious diseases. Large populations didn’t happen until the advent of farming, and with it came the first plagues. The first farming villages were small, but “as the Reverend Malthus pointed out in 1798, even modest increases in a population’s birthrate will cause rapid increases in overall population size in just a few generations.” (Lieberman, 2013: 197) So as even small increases in population size would cause a boom in future generations, which along with it would drive disease acquisition and plagues in that new and stationary society.
Lieberman further writes on pages 199-200:
Not surprisingly, farming ushered in an era of epidemics, including tuberculosis, leprosy, syphilis, plague, smallpox and influenza. (44) This is not to say that hunter-gatherers did not get sick, but before farming, human societies primarily suffered from parasites such as lice, pinworms they acquired from contaminated food, and viruses or bacteria, such as herpes simplex, which they got from contact with mammals. (45) Diseases such as malaria and yaws (the nonvenereal precursor of syphilis) were probably also present among hunter-gatherers, but at much lower rates than in farmers. In fact, epidemics could not exist prior to the Neolithic because hunter-gatherer populations are below one person per square kilometer, which is below the threshold necessary for virulent diseases to spread. Smallpox, for example, is an ancient viral disease that humans apparently acquired from monkeys or rodents (the disease’s origins are unresolved) that was able to spread appreciably until the growth of large, dense settlements. (46)
Moreover, another evolutionary mismatch is the lack of sanitation that comes with stationary societies. Hunter-gatherers could just go and defecate in a bush, whereas with the advent of civilization, waste and refuse began to pile up in the area. As noted above, when farmers clear space for irrigation to plant crops, this introduces mosquitoes into the area which then causes more disease. Furthermore, we have also acquired about 50 diseases from living near animals (Lieberman, 2013: 201). There are more than 100 evolutionary mismatch diseases that agriculture has brought to humanity.
We can compare disease rates of people in industrialized societies and people in modern-day hunter-gatherer societies. In his 2008 book Good Calories, Bad Calories, Gary Taubes documents numerous instances of hunter-gatherer societies that have no to low rates of the same modern diseases that we have:
In 1914, Hoffman himself had surveyed physicians working for the Bureau of Indian Affairs. “Among some 63,000 Indians of all tribes,” he reported, “there occurred only 2 deaths from cancer as medically observed from the year 1914.” (Taubes, 2008: 92)
“There are no known reasons why cancer should not occasionally occur among any race of people, even though it be below the lowest degree of savagery and barbarism,” Hoffman wrote. (Taubes, 2008: 92)
“Granting the practical difficulties of determining with accuracy the causes of death among the non-civilized races, it is nevertheless a safe assumption that the large number of medical missionaries and other trained medical observers, living for years among native races throughout the world, would long ago have provided a substantial basis of fact regarding the frequency of malignant disease among the so-called “uncivilized” races, if cancer were met with among them to anything like the degree common to practically all civilized countries. Quite the contrary, the negative evidence is convincing that in the opinion of qualified medical observers cancer is exceptionally rare among the primitive peoples.” (Taubes, 2008: 92)
These reports, often published in the British Medical Journal, The Lancet or local journals like the East African Medical Journal, would typically include the length of service the author had undergone among the natives, the size of the local native population served by the hospital in question, the size of the local European population, and the number of cancers involved in both. F.P. Fouch, for instance, district surgeon of the Orange Free State in South Africa, reported to the BMJ in 1923 that he had spent six years at a hospital that served fourteen thousand natives. “I never saw a single case of gastric or duodenal ulcer, colitis, appendicitis, or cancer in any form in a native, although these diseases were frequently seen among the white or European population.” (Taubes, 2008: 92)
As a result of these modern processed foods, noted Hoffman, “far-reaching changes in bodily functioning and metabolism are introduced which, extending over many years, are the causes or conditions predisposing to the development of malignant new growths, and in part at least explain the observed increase in cancer death rate of practically all civilized and highly urbanized countries.” (Taubes, 2008: 96)
The preponderance of evidence shows that these people have low rates of disease that are endemic to our societies due to the advent of agriculture. There is one large difference between hunter-gatherer societies and industrialized ones: the type and amount of food we eat.
Along with the boom of agriculture, we see a slight decrease in height the longer people live in these types of societies. As the Neolithic began 11,500 years ago, height increased about 1.5 inches for males and slightly less for females. But around 7,500 years ago, stature began to decrease and we began noticing evidence of nutritional stress and skeletal markers of disease. There is evidence that as maize was introduced into eastern Tennessee about 1,000 years ago, a decrease of .87 inches in men and 2.4 inches in women were seen. Further, the height of early farmers in China and Japan decreased by 3.1 inches as rice farming progressed, with similar height decreases being seen in Mesoamerica in men (2.2 inches) and women (3.1 inches).
Anti-hereditarian Jared Diamond asks the question “Was farming worth it?” in which he writes:
With agriculture came the gross social and sexual inequality, the disease and despotism, that curse our existence.
The first two things he brings up are pretty Marxist in nature, though they are true. He implies that agriculture causes so-called ‘sexual inequalities’ in which women are made ‘beasts of burden’, made to do the work while men walk by ’empty handed’. This seems to be one negative to a society that is, supposedly, smarter than Europeans.
Regular readers may remember me criticizing Andrew Anglin and his stance on the paleo diet—with how it’s ‘how European man evolved to eat’. However, I am a data-driven person and I try to not let any bias get involved in my thought processes. I know do believe that we should eat a diet that closely mimics our hunter-gatherer ancestors, though we shouldn’t go overboard like certain people in the paleo community, we should be mindful of the quality of food we do it as we will greatly increase our life expectancy along with our quality of life. Indeed, researchers have proposed that we should adopt diets that are close in composition to what our hunter-gatherer ancestors ate in order to battle diseases of civilization. Based on what I’ve read over the past few months, I am inclined to agree. Indeed, evidence for this is seen in a sample of ten Australian Aborigines who were introduced back to their traditional lifestyle (O’Dea, 1984). In a 7 week period, they showed improvement in carbohydrate and lipid metabolism, effectively becoming diabetes-free in almost 2 months.
In sum, there were obviously both positive and negative effects on human life due to the advent of agriculture (leaning more towards negative). These range from diseases to increased population size, to ‘social inequalities’ to higher rates of obesity (this evolutionary mismatch will be extensively covered in the future) to a whole myriad of other diseases. These then lower the quality of life of the individual inflicted. However, the rates of these diseases are low to non-existent in hunter-gatherer societies due to them being nomadic and eating more plentiful foods. Agricultural societies become dependent on a few staple crops so when an endemic occurs, there is mass death since they do not know how to subsist on anything but what they have become accustomed to. The advent of agriculture leads to a decrease in stature as well as brain size. Further, agriculture and the processed foods that came with it caused us to become more susceptible to obesity, which was further exacerbated by the industrial revolutions and the ‘nutritional guidelines’ of the 60s and 70s that led to higher rates of coronary heart disease. It is the lifestyle change from agriculture that we have not adapted to yet that causes disease these diseases of civilization that shorten our life expectancies. I do now believe that all people should eat a diet as close to hunter-gatherer diet as possible, as that’s what the preponderance of evidence shows.
By the way, to my knowledge, contrary to what The Alternative Hypothesis says, there are no differences in carbohydrate metabolism between races (save for a few populations such as the Pima).
Agriculture and Evolution: A Reply to The Alternative Hypothesis
2050 words
I love nutrition science. So much so that I read a new book on it every week. The Alternative Hypothesis has a pretty old video on agriculture and evolution. I strongly disagree with his main thesis. I strongly disagree with his denigration of Gary Taubes. Most of all, I strongly disagree with what he says about the East Asian rice eaters because since that video has been made, the carbohydrate/insulin hypothesis of obesity has changed to the insulin hypothesis of obesity.
In the very beginning of the video he brings up Gary Taubes’s research on low-carb diets and how people tend to be healthier than those who eat higher carb diets. He brings up the East Asians who eat a lot of rice. However, it’s clear he doesn’t know that the percent of carbohydrate intake is nowhere near as important as the absolute amount of carbohydrate consumed:
- They consume a fraction of the sugar we do. More sugar consumption leads to greater insulin resistance, more fat creation, less fat breakdown, and more fat accumulation.
- They consume less total glucose, AND the glucose they consume is accompanied by less sugar (and less omega-6 PUFA, if it matters).
- They consume a ratio of omega-6 to omega-3 PUFA that is much lower than we do. This mayfurther reduce any insulin resistance brought on by the glucose they do consume (in smaller doses and with less sugar).
The fact that East Asians didn’t have high rates of diabesity (diabetes and obesity) was a big blow to the carbohydrate insulin hypothesis. However, the East Asian rice paradox is simply explained by low, if non-existent, consumption of refined carbohydrates. Those populations actually consume fewer total carbohydrates than Western diets, and have lower levels of glycemic load as a result. To quote Mark Sisson:
Before recently, Asians ate less refined sugar and used animal fats for cooking. Sugar intake is rising now, of course, and cooking oils made from corn and soybean have largely replaced lard and tallow, but rice in the context of a low-sugar, no-HFCS (remember, the oft-cited 55/45 fructose/glucose breakdown for HFCS is highly misleading and actually quite often incorrect), low-vegetable oil, nose-to-tail nutrient-dense diet is (or was) acceptable. You can’t reduce a food down to its constituent parts and focus on, say, the bit of fructose in a blueberry and then condemn the entire berry because of it. Similarly, you can’t reduce a diet down to a single constituent food and condemn – or praise – it based on that single food. You have to look at the entire picture, and the Asian diet is largely a nutritious one.
These paradoxes where one population seems to disprove a certain hypothesis are pretty easily explainable with the existing data. There are numerous reasons why East Asian rice eaters have lower rates of diabesity. Dr. Jason Fung also explains why:
Wheat, particularly in the modern iteration may be particularly fattening for numerous reasons. The high level of amylopectin means that most of the starch contained in flour is efficiently converted to glucose. This deadly combination of wheat and sugar has been introduced into the Chinese diet. The result is a Chinese diabetes catastrophe. The prevalence of diabetes in China has now even outstripped the USA.
This is the answer to the paradox of the Asian Rice eater puzzle. Why didn’t the Chinese have a diabetes epidemic in 1990 with all their white rice? Well, because they didn’t eat any sugar (fructose), they were not developing insulin resistance. Because they were not snacking all the time, they had periods of low insulin level that helped prevent the development of insulin resistance. So the high rice intake by itself was not enough to cause either of diabetes or obesity.
Then he says that whites intake more total carbs in comparison to blacks and ‘Hispanics’ (1:32 in the video). This is wrong.
Diaz et al (2005) showed that minority populations are more likely to be affected by diabetes mellitus which may be due to less healthy diets and/or genetic factors. Using the National Health and Nutrition Survey for 1999-2000, they analyzed overweight, healthy adults, calculating dietary intake variables and insulin sensitivity by ethnicity. They characterized insulin resistance with fasted insulin, as those who are more likely to become insulin resistant have higher fasted insulin levels (levels taken after waking, with the subject being told not to eat the night before as to get a better reading of fasted insulin levels). Non-‘Hispanic’ whites had higher energy and fat intake while ‘Hispanics’ had higher carb intake with blacks having lower fiber intake. Blacks and ‘Hispanics’ were more likely to have lower insulin sensitivity. However, ‘Hispanics’ were more likely to have lower insulin sensitivity even after controlling for diet, showing that metabolic differences exist between ethnicities that affect carbohydrate metabolism which leads to higher rates of diabetes in those populations.
Diaz et al state in the results of the study:
Dietary differences are seen by ethnicity, with non-Hispanic whites having higherenergy, saturated fat and total fat intake, while Hispanics had higher carbohydrate intake and African-Americans had lower fibre intake.Both African-Americans and Hispanics had higher levels of fasting insulin, demonstrating lower insulin sensitivity in comparison with non-Hispanic whites.
So now that I’ve established that blacks and ‘Hispanics’ consume more total carbohydrates from refined foods, now I’ll show the physiologic effects of insulin.
Insulin inhibits the breakdown of fat in the adipose tissue by inhibiting the lipase that hydrolyzes (the chemical breakdown of a compound due to a reaction with water) the fat out of the cell. Since insulin facilitates the entry of glucose into the cell, when this occurs, the glucose is synthesized into glycerol. Along with the fatty acids in the liver, they both are synthesized into triglycerides in the liver. Due to these mechanisms, insulin is directly involved with the shuttling of more fat into the adipocyte. Since insulin has this effect on fat metabolism in the body, it has a fat-sparing effect. Insulin drives most cells to prefer carbohydrates for energy. Putting it all together, insulin indirectly stimulates the accumulation of fat into the adipose tissue.
Do you see why blacks and ‘Hispanics’ are more susceptible to obesity?
Another glaring error he commits is not separating refined carb consumption with natural carb consumption. Refined carbs spike insulin much more than those foods with natural carbohydrates. East Asians do not have a “higher carbohydrate tolerance than Europeans” (2:06 in the video). This one huge error he commits completely discredits his hypothesis.
He then goes on to talk about India’s diabetes rates. But why is it increasing? Because of Western diets. It’s not about a “lower carbohydrate tolerance” as he says at 3:07, it’s about consuming more refined carbohydrates.
Then at 5:05, he says that he’s “solved Gary Taubes’s race problem in regards to diet”. He did nothing of the sort.
I, of course, have no problem with his IQ data. I have a problem with the conclusions he jumps to in regards to carbohydrates and diabetes. He clearly didn’t look at other factors that would explain why East Asians have lower rates of diabesity (which is increasing as they adopt a Western lifestyle… Weird…). The same thing explains it with the Australian Aborigines.
I have absolutely no problem with the second half of his video. My problem is the first half of it–his denigration of Taubes, non-understanding of insulin spikes in comparison to the quality of carbohydrate ingested and not controlling for refined carbs– as it’s clear he didn’t do extensive research into these populations (which Taubes and others have) to show why they don’t have higher rates of diabesity.
What he doesn’t touch on are “obesogenic environments” which is defined as “the sum of influences that the surroundings, opportunities, or conditions of life have on promoting obesity in individuals or populations”. What a huge coincidence that most of the populations he cited today with higher rates of diabesity live in first-world nations, otherwise known as obesogenic environments.
He should have spoken about the Pima Indians and their rates of diabesity. They didn’t have rates of diabesity as high 100 years ago. Why? The introduction of the obesogenic environment. Prisancho (2003) in his study on the Pima and reduced fat oxidation in first-world countries showed how the Pima preferentially burn carbs and not body fat for energy. Fat-burning would account for 9 kcal lost and CHO for 4. Since they preferentially burn carbs for energy and not fat, this shows why they have higher rates of diabesity. It’s not that it’s a genetic susceptibility to burn CHO for energy over fat (there may be a small genetic component, but it doesn’t override the effects of the actual diet). I’ve shown insulin’s role in fat storage above, do you see why the Pima have this diabesity epidemic after the introduction of refined carbohydrates and the obesogenic environment?
Added sugars and salts in foods causes us to want more of those foods. As I alluded to above, food scientists continuously work to find out which combinations of sugar, salt and fat will be more hyperpalatable to us and make us eat them more. Whites nor East Asians have a ‘higher carb tolerance’, they just eat different types of carbs (mostly unrefined, in comparison to blacks and ‘Hispanics’ anyway). If any individual were to overeat on high carb foods they would become diabetic and obese. Whites nor East Asians are exempt from that.
In sum, he didn’t look at where the carbs came from, only total carb intake. Refined carbs and unrefined carbs do different things in the body. The whiter a processed food is, the more it is refined. The more a food is processed, the more its natural nutrients such as fiber are taken out. These low-fat refined foods are one cause of obesity. However, it’s way too complicated to say that only refined carbohydrates cause diabesity.
I strongly recommend he read Taubes’s and Fung’s books. If he did, he wouldn’t have said what he said about Taubes’s theory and completely disregard the absolute total amount of carb intake and not the total amount of carbohydrates ingested.
Are Flynn Losses in France Due to Immigration?
1850 words
Over a ten year period in France, from 1999 to 2008-9, IQ has declined in France by almost 4 points. What is the cause? Immigration? Dysgenics? A reversal of the Flynn Effect? No doubt that numerous people would attribute the decline in intelligence in France due to MENA and SSA immigration. But is this true?
Lynn and Dutton (2015) show how differing studies show both positive and negative gains in IQ. To prevent further evidence of these negative Flynn gains, they looked to the IQ of France from 1999-2009.
The WAIS-III was standardized in France in 1999 while the WAIS-IV was standardized in 2009. This was a great opportunity to see if the intelligence of the French dropped using the new WAIS-IV. The sample was of 79 people who were of a different sample than that of the broader WAIS-IV French standardization. The average age of the sample was 45, ranging between 30 and 63 years of age. Half of this sample took the WAIS-IV first while the other half took the WAIS-III first to control for practice effects. They used a separate sample to compare the norms of generated by the two standardizes samples.
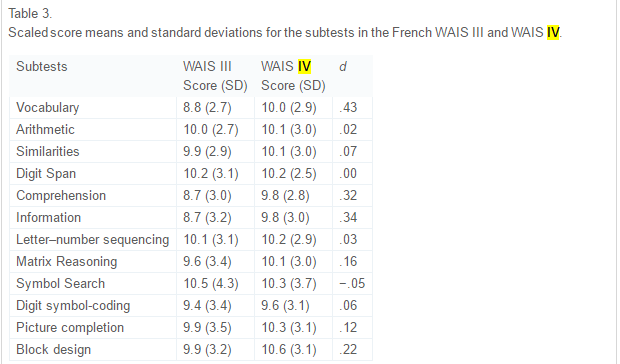
The above table from the paper, table 3, shows the comparison between the two WAIS tests. Positive ds indicate lower scaled scores on the III in comparison to the IV and thusly higher scores. What these data show is that the IV is harder than the III and IQ declined because the test got ‘tougher’ (because full-scale intelligence declined). As noted above, this phenomenon of decreasing IQ scores has been noticed for about 20 years now. The symbol search showed the smallest decline while there was no change in digit span. The biggest gain was in vocabulary.
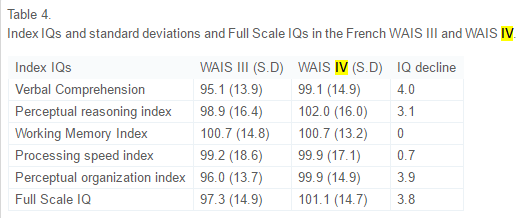
This is pretty shocking. In ten years, verbal comp decreased by 4 points, perceptual reasoning index by 3.1 points, no change in working memory index, processing speed index decreased by .7 points, perceptual organization index decreased by 3.9 and the whole full-scale IQ decreased by 3.8 points. Lynn and Dutton discuss the results:
In addition, the Full Scale IQ on the WAIS IV sample of 79 subjects was calculated based on a comparison with the WAIS IV sample of 876 subjects, which was representative of the French population on key variables such as education and region. The scores of this sample of 876 subjects were set at 100 and a comparison made with the sample of 79 subjects. As can be seen in Table 4, on this basis the IQ of the sample of 79 subjects was 101.1 with an SD of 14.7, where the French norm would be 100 and the SD 15. As such, the smaller sample can be regarded as representative of the French population in terms of intelligence.
So this small sample can be regarded as representative of the French population. Lynn and Dutton say that the digit span showing no increase corroborates findings from another researcher that showed that there was no change in forward or backward digit span in 85 years. They then say:
. . .improvements in the quality of nutrition during the twentieth century made a major contribution to increasing IQs. But it seems improbable that the quality of nutrition declined in recent years in France and in the other economically developed countries in which declining IQs have been reported.
So one possible cause is that nutrition has declined in France. From Dubuisson et al, 2010:
These repeated surveys highlighted the fact that trends in French food habits have moved towards an average European diet at the crossroads between Mediterranean and Northern diets, and that food consumption changes impacted, to a lesser extent, nutritional intake.
It shows that the French diet is in between Med and Nord diets. Really, as Lynn and Dutton asserted, there was no decline in nutritional quality for the French.
Another possible cause is a decrease in quality of schools. Flynn says a part of the reason for the rise in IQ was due to the advent of scientific thinking. However, this is not a good explanation either since school quality seems to not have been affected.
Flynn also talks about the media and its role. Lynn and Dutton say:
However, this would not explain declines in other forms of intelligence and, moreover, it might be argued that the desire and ability to read such literature would be underpinned by general intelligence and so a decline in the consumption of such literature would partly reflect a decline in general intelligence, as vocabulary is a measure of intelligence.
It is also worth noting that, apparently, reading may actually increase general intelligence (post coming on that soon).
Now, finally, the theory we’ve all been waiting for: Is it increased immigration?
Lynn and Dutton state:
This increase has occurred throughout western Europe and a number of studies have shown that immigrants from North Africa and south-west Asia typically have an average IQ of around 85 to 90 (Lynn, 2006, Lynn, 2008, Lynn and Vanhanen, 2012 and Rindermann and Thompson, 2014; for a large meta-analysis see te Nijenhuis, de Jong, Evers, & van der Flier, 2004). This conclusion has been confirmed by Kirkegaard (2013) who has shown that in Denmark the number of non-European immigrants increased from approximately 50,000 in 1980 to 400,000 in 2012 and the IQ of non-European immigrants in 18–19 year old military conscripts was 86.3, relative to 100 for indigenous Danes. These immigrants are likely to have had some impact on reducing the average IQ of the populations, but it is doubtful whether the increase in the number of immigrants with lower IQs has been sufficiently great to have had a major effect.
I personally don’t think that migration into Europe from MENA and SSA countries has been enough to put that big of a dent (over 1/3rd of an SD) in average IQ in France, and Europe as a whole. Since people are coming from areas closer to the equator and have higher rates of children since they are r-selected, could this be why France has seen a decrease in intelligence?
No.
Woodley of Menie and Dunkel (2015) reviewed Lynn and Dutton’s paper and said:
Replacement migration in France involving populations exhibiting lower means of IQ and higher rates of total fertility, such as Algerians, Moroccans, Tunisians and Roma (Čvorić, 2014 and Lynn and Vanhanen, 2012) may be increasing the rate of secular losses at the level of g, consistent with speculations advanced in Dutton and Lynn (2015), however the additional loss in g due to this process is anticipated to be very small. Based on a simulation, Nyborg (2012) estimates that in Denmark, replacement migration may be reducing heritable g by .28 points per decade, which would increase the overall loss in g to 1.51 points per decade ( Woodley of Menie, 2015), this still being only 37.75% of the loss observed in the French cohort.
An Environmental Explanation?
Since we still need an explanation for 62.25 percent of the 3.8 decrease in full-scale IQ other than dysgenic fertility, are there any environmental explanations? Environmental explanations can be anything from child abuse, to poor schooling, to poor nutrition, etc. Was there an increase in any of these or other variables that negatively affect IQ which would explain the 3.8 point decline in IQ?
One of the most likely candidates is nutrition. Lack of certain vitamins, especially in childhood, would prevent the brain from receiving the proper nourishment to grow.
The INCA study took record of food consumption from 2,373 people aged 4 to 92 from a 7-week period and from that they saw which nutrients they were deficient in (Touvier et al 2006). To measure if and how much they were nutrient deficient, they used the Estimated Average Requirement (EAR). The vitamins used were calcium, magnesium, iron, vitamins C, A, B6, and B12, thiamin, riboflavin, niacin, pantothenic acid, and folate. A lot of these have to do with proper brain functioning and ability to reach its full-size potential. For instance like the B vitamins and iron. Being deficient in those nutrients depresses brain size and with it IQ. For instance, being deficient in vitamin B 12 and folate leads to decreased brain size in childhood. The negative effects of being deficient in these nutrients may partially explain some of the 3.8 point decrease in full-scale IQ.
Regarding the prevalence of the aforementioned nutrient deficiencies in these populations, the authors state:
We also calculated daily consumption of 44 food groups by age and gender. This paper shows how the combination of both data sets, i.e., inadequacy and food consumption data, allows a preliminary screening of potential food vehicles in order to optimize fortification. The prevalence of inadequacy was particularly high for the following groups: for calcium, females aged 10-19 years (73.5%) or aged 55-90 years (67.8%), and males aged 15-19 years (62.4%) or aged 65-92 years (65.4%); for magnesium, males aged 15-92 years (71.7%) and females aged 10-90 years (82.5%); for iron, females aged 15-54 years (71.1%); and for vitamin C, females aged 15-54 years (66.2%). Two examples are provided to illustrate the proposed method for the optimization of fortification.
Most vitamins and minerals have positive effects on brain functioning, some more than others, but notice the prevalence of iron defieciency in the females aged 15-54 years (71.1 percent). With the cohort cited by Lynn and Dutton (2015) and Woodley of Menie and Dunkel (2015) being aged 30 to 63 with an average age of 45, the prevalence of iron deficiencies in the INCA study, along with the other deficiencies in the cohort, may partially be responsible for the decline in IQ.
The Flynn Effect
PumpkinPerson describes it well here:
One of the biggest mysteries in psychology is the Flynn Effect; the fact that over the 20th century, people have been performing better and better on IQ tests. Of course, the average IQ in Western countries by definition is always about 100, however because people keep scoring higher every decade, the tests routinely have to be made more difficult and the norms must be regularly updated to keep the mean IQ from rising far above 100.
However, in first-world countries, in the past 20 or so years, it has been in decline, particularly in France. It’s due to a mix of dysgenic fertility and nutrient deficiencies. Since Flynn gains are largely due to advancements in better nutrition, Flynn loses would then be attributed in part to nutrient deficiencies as well as dysgenic fertility.
The cause for the 3.8 decrease in IQ in France is low fertility rates amongst the French population as well as nutrient deficiencies. Clearly, ameliorating this decrease in IQ can be reversed by the K-selected having more children and healthier eating habits. Drops in IQ won’t be attributed to MENA and SSA populations until the future, but for now, the cause for the decrease is the French themselves.
Ethnic Differences in Sleep, Obesity, and Metabolic Syndromes
2300 words
Ethnic differences in the prevalence of obesity occur, majorly in part due to differences in the rates of metabolic syndrome (which is actually a few variables including high blood pressure, high blood sugar which leads to insulin resistance, excess visceral fat around the waist which is the ‘skinny fat‘ phenomenon, and abnormal blood pressure levels) and obesity. Ethnic differences in these variables do, in part, show how the three ethnies differ in rates of obesity. I will discuss the differences between each ethny in regards to metabolic syndrome and sleep and how it leads to the differences in ethnic obesity rates.
Sleep Differences
There is a ‘missing hour of sleep‘ when comparing blacks and whites. On average, blacks get 6.05 hours of sleep while whites get 6.85 hours of sleep. Of course, the same old racism argument comes up, which, if one ‘percieves’ discrimination, I wouldn’t doubt that it would have an effect on sleep due to a rise in cortisol, which affects sleep due to the raised levels making you restless and not able to fall asleep. Insulin levels then rise due to the rise in cortisol, which is the cause of obesity.
Some studies may try to say that racism and other forms of discrimination are a factor, without even thinking of genetic factors. Another study that Frost cites says that duration of deep sleep and duration of stage 2 (light sleep) is correlated correlated in African Americans with perceived discrimination. The authors defined ‘perceived discrimination’ as the extent to which one believes that their ethnic group have been discriminated against by society. Still even when controlling for discrimination, there were still marked differences between blacks and whites and how long they slept.
Frost then talks about how sleep patterns are heritable and cites studies done on Africans in Africa. One study found that there was an hour sleep difference between Ghanaians and Norwegians on the week days and between a quarter to half hour less on weekends. He shows another study showing that Nigerian college students sleep 6.2 hours a day while getting 70-minute naps in the afternoon.
Frost concludes that the African sleep patterns is normal on Africa. Africans are more active during the cooler times of the day and sleep during the bitter periods. Frost says those who evolved in more northerly climes are particularly adapted to a certain sleep pattern with the same holding true for Africans.
However, these sleep patterns in first world countries have negative effects on metabolism and rates of obesity.
Here are some more studies showing that blacks sleep less than whites:
The sleep of African Americans: a comparative review: The researchers found that blacks take longer to fall asleep than whites, report poorer sleep quality, have more light and less deep sleep, and nap more often and longer. This is a huge recipe for risk factors for obesity, and it shows in their demographics.
Unfair Treatment is associated with Poor Sleep in African American and Caucasian Adults: Pittsburgh SleepSCORE Project: This is one of the studies spoken about above that show that discrimination leads to less sleep. Though, it holds for both black and white adults. The researchers conclude:
Taken together, the confluence of perceived unfair treatment as a chronic stressor and poor sleep and the interplay between the two may have critical roles in long-term health problems.
African Genetic Ancestry is Associated with Sleep Depth in Older African Americans: The researchers hypothesized that “racial differences in sleep phenotypes would show an association with objectively measured individual genetic ancestry in AAs.” They conclude that the slow wave sleep may have genetic underpinnings.
Mexican Americans sleep less than do Mexican immigrants. US-born Mexicans are 40 percent more likely to be short sleepers. This is attenuated by environmental factors such as smoking and stress, which shorten the duration of sleep (smoking decreases the Body Set Weight, whereas cortisol along with insulin in tandem increase it).
Also, in this study by Roane et al (2014) looked at the link between sleep disturbances and stress in Mexican Americans (average age 55) and non-‘Hispanic’ whites (average age 66). Mexicans reported higher levels of sleep disturbance (25 percent) compared to whites (17 percent). They conclude that disturbed sleep was positively correlated with depression.
So both blacks and Mexicans sleep less than whites. These differences in sleep between these three ethnies also affect the prevalence of obesity in these populations.
Obesity and Sleep
It’s long been known that poor sleep habits make people fat. This is due to the effects of insulin and cortisol. Increased insulin comes before increased cortisol–increased insulin is the cause for obesity. Sleeping less is linked to obesity. Since, as described above, the three ethnies differ in sleep patterns, the same also holds true for obesity rates (Ogden at al, 2014). The trends are as follows: 67.3% for whites, 75.6% for blacks, and 77.9% for Hispanics. Though, sleep is only one factor involved with obesity.
Getting adequate sleep is extremely important. Not doing so can lead to a myriad of negative health implications:
Sleep is an important modulator of neuroendocrine function and glucose metabolism and sleep loss has been shown to result in metabolic and endocrine alterations, including decreased glucose tolerance, decreased insulin sensitivity, increased evening concentrations of cortisol, increased levels of ghrelin, decreased levels of leptin, and increased hunger and appetite. Recent epidemiological and laboratory evidence confirm previous findings of an association between sleep loss and increased risk of obesity.
So a lack of sleep leads to an increase in ghrelin levels, decreased levels of leptin (the same effects as caloric restriction over time), increased appetite and hunger, increased evening cortisol (which insulin spikes then follow), decreased insulin sensitivity (the cortisol brings it back up and most people are insulin resistant independent of diet), decreased glucose tolerance, etc. We can see that these ethnic differences in sleep, which are partly genetic in nature, can and would have great effects on metabolism, contributing to the ethnic differences in obesity rates.
And from Harvard:
For example, in the Nurses’ Health Study, researchers followed roughly 60,000 women for 16 years, asking them about their weight, sleep habits, diet, and other aspects of their lifestyle. (2) At the start of the study, all of the women were healthy, and none were obese; 16 years later,women who slept 5 hours or less per night had a 15 percent higher risk of becoming obese, compared to women who slept 7 hours per night. Short sleepers also had 30 percent higher risk of gaining 30 pounds over the course of the study, compared to women who got 7 hours of sleep per night.
Damn!! This, pretty much, mirrors the black-white difference. I’d love to see a racial breakdown of this cohort and will keep an eye out for one, but in the meantime, those who were short sleepers had a 30 percent higher risk of gaining 30 pounds over the course of the study in comparison to women who got 7 hours of sleep per night. Blacks are the most likely group to be overweight and obese in the US, and this data from the Nurses Health Study (which tons of data can be drawn from this study) shows one reason why, however the driver is cortisol > insulin > processed carbs > increased insulin > insulin resistance > increased insulin > vicious cycle > obesity. These differences in sleep almost perfectly mirror the ethnic differences in obesity.
There are several possible ways that sleep deprivation could increase the chances of becoming obese. (1) Sleep-deprived people may be too tired to exercise, decreasing the “calories burned” side of the weight-change equation. Or people who don’t get enough sleep may take in more calories than those who do, simply because they are awake longer and have more opportunities to eat; lack of sleep also disrupts the balance of key hormones that control appetite, so sleep-deprived people may be hungrier than those who get enough rest each night.
Ah the old ‘exercise to increase the Calories Out part of the equation’. however, Calories Out does not stay constant. This also rebuts the ‘Eat Less and Move More’ CICO (Calories In/Calories Out) model of obesity, showing that because it doesn’t take insulin into account, it’s doomed to fail.
Speaking of insulin, it’s about time I focused on metabolic syndrome.
Metabolic Syndrome
As I discussed in a previous post, Race, Obesity, Poverty, and IQ, metabolic differences exist between race/ethnicity. ‘Hispanics’ metabolize carbohydrates differently, blacks have a lower fiber intake (increased fiber protects against obesity, another correlate) while whites have a more high fat diet. Contrary to popular belief, dietary fat doesn’t make you fat as it’s the macro that spikes your insulin the least.
Diaz et al (2005) showed that minority populations are more likely to be affected by diabetes mellitus which may be due to less healthy diets and/or genetic factors. Using the National Health and Nutrition Survey for 1999-2000, they analyzed overweight, healthy adults, calculating dietary intake variables and insulin sensitivity by ethnicity. They characterized insulin resistance with fasted insulin, as those who are more likely to become insulin resistant have higher fasted insulin levels (levels taken after waking, with the subject being told not to eat the night before as to get a better reading of fasted insulin levels). Non-‘Hispanic’ whites had higher energy and fat intake while ‘Hispanics’ had higher carb intake with blacks having lower fiber intake. Blacks and ‘Hispanics’ were more likely to have lower insulin sensitivity. However, ‘Hispanics’ were more likely to have lower insulin sensitivity even after controlling for diet, showing that metabolic differences exist between ethnicities that affect carbohydrate metabolism which leads to higher rates of diabetes in those populations.
In ‘Hispanics’, several loci were discovered that play a role in hepatic (relating to the liver) fat content. Along with showing that ‘Hispanics’ have lower insulin (which due to low insulin, blood glucose builds up in the blood stream leading to diabetes) and showing that they metabolize glucose in the liver differently due to differing loci leading to more cases of fatty liver, this shows how and why ‘Hispanics’ have higher rates of Type II Diabetes Mellitus (TIIDM).
Since TIIDM affects Mexican Americans more, better measures to address their differences in carbohydrate metabolism need to be taken. Racial and ethnic differences in TIIDM are as follows:
7.6% of non-Hispanic whites
9.0% of Asian Americans
12.8% of Hispanics
13.2% of non-Hispanic blacks
15.9% of American Indians/Alaskan Natives
Whites eat a higher fat diet, which means a decrease in carbs. Asians eat white rice which spikes blood glucose eliciting a high insulin response leading to TIIDM, ‘Hispanics’, non-‘Hispanic’ blacks, and Indians and Alaskan Natives (I wish they separated Indians and Alaskan Natives as I’m almost positive that Alaskan natives have a lower rate) all eat high carb, low fat, low protein diets. Carbohydrates are a main staple, and since they spike insulin the most, they are the cause for obesity and TIIDM rates in these populations.
Turning my attention over to metabolic syndrome and blacks and whites, we can see that black women with PCOS have an increased risk for cardiovascular disease and metabolic syndrome in comparison to white women with PCOS. The researchers say that after controlling for age and body mass index (BMI) “black women with PCOS had a significantly increased prevalence of low high-density lipoprotein and high glucose. The general CVD risk was significantly increased in black adults with PCOS.” Though, a longitudinal study needs to be carried out to assess the independent impact of race and PCOS with CVD (Cardiovascular Disease).
Blacks have a higher chance to be diagnosed with metabolic syndrome since they are also at increased risk to have elevated blood pressure (hypertension), become obese, and be diabetic. This is due to their diet, which is due to their low IQ (obesity is correlated with intelligence), and different metabolism in comparison to whites.
There are also metabolic differences between race and sex. Fat oxidation is lower in black than white men and in African American men/women and white men/women, they have a lower metabolic rate!!! 24-hour energy expenditure is lower in black women in comparison to white women, whereas physical activity energy expenditure (PAEE) is the same as whites. Contrasted with women, black men had higher PAEE than white men. The authors conclude:
In conclusion, this comparative study of 24-h energy metabolism in African Americans and whites with use of a respiratory chamber not only confirms the previous findings from ventilated-hood studies of a lower resting metabolic rate, but also suggests a lower 24EE in African American women than in white women. Although only marginal ethnic differences in metabolic rate were found in men, African American men seem to have a lower rate of fat oxidation than do white men. The underlying mechanisms for these sex differences and the significance of these findings with respect to the development and maintenance of obesity remains to be investigated in longitudinal studies.
Metabolic Syndrome and Obesity
The Weston A. Price Foundation and Nutritional Myths
1350 words
There is a ‘foundation’ called the Weston A. Price Foundation. They push heavily questionable data, along with not updating their material when refuted or new studies come out. It was started in 1999 by Sally Fallon and nutritionist Mary Enig (Ph.D.). The Price Foundation advocates drinking raw milk, yet they have been criticized by the FDA for saying this.
Dr. Weston A. Price was a well-respected dentist from Cleveland. His son died from tooth decay which got him interested in the causes for tooth decay in modern populations. In 1939, he wrote Nutrition and Physical Degeneration. He and his wife traveled around the world and conducted various studies on modern populations living in isolated areas and compared them to those of the same country of origin in modern populations.
The countries he conducted studies in include: isolated and modernized Swiss, isolated and modernized Gaelics, isolated and modernized Eskimos primitive and modernized North American Indians, isolated and modernized Melanesians isolated and modernized Polynesians, isolated and modernized African tribes, isolated and modernized Australian Aborigines, Isolated and modernized Torres Strait islanders, isolated and modernized New Zealand Maori, ancient civilizations of Peru, isolated and modernized Peruvian Indian. He found that despite having no forms of dental hygiene that they had better dental crests and a lower, almost non-existent case of cavities in their population. He states that primitive people lived longer, but, this is not the case.
In private, Dr. Price told his family to eat a vegetarian diet. That has its problems as well. Since the average American doesn’t know how to correctly supplement certain vitamins and minerals, this will lead to nutrient deficiencies and eventually, less ability to fight off disease.
Though, the type of ‘science’ that the Price Foundation pushes will lead you to sickness and even, maybe, eventual death. They tell people to consume raw milk (this site is affiliated with the Price Foundation). They recommend diets high in saturated fats and no fruits and vegetables for children. However, it’s been very well-established that lack of those aforementioned foods leads to an increase in cancer in adulthood.
The WAPF recommends people to eat high amounts of saturated fat, which is the type of fat found in animals. Using data taken from the Food and Agricultural Organization of the United Nations (FAO) study done in 38 countries from 1979-1981, Kestelhoot, Lessafire and Joossens (1991) discovered that per person supply of fat from dairy products and lard cancer mortality were significantly correlated with total, breast, prostate, colorectal and lung cancer. Their findings support the concept of the role of saturated fat in the elevation of cancer risk.
A prominent name for the WAPF is Dr. Joseph Mercola, doctor of osteopathic medicine. The FDA has issued an order to Dr. Mercola to stop his illegal claims. He’s a snake oil salesman, just like the rest of the WAPF and those affiliated with them. Back in 2009, Dr. Mercola made unsubstantiated scientific claims about the nature of the H1N1 (Swine Flu) virus. It’s clear that Mercola, though he does have actual information on his website, is just getting paid by the WAPF to be just a name and put forth false claims so people will believe him since he has the title of “Doctor”.
They even make claims with some serious implications for babies if parents follow their advice. They recommend that a baby be given a blend of cow’s milk with heavy cream and oil and another blend of cow’s liver, beef broth, whey protein and various other oils. However, this type of diet for a newborn infant is extremely dangerous. Infants deficient in iron can begin to have a whole slew of health problems including anemia and damage to intelligence, behavior and motor functioning. Putting a baby on this diet will lead to lifelong problems that will not reverse even with a correct amount of iron. Lack of iron is correlated with diminished intelligence in children, but in children aged 5 and up it is possible to reverse the effect with increased supplementation of iron. The cause for the irreversibility of intelligence in those younger than five years of age is due to that being one of the most critical time for brain development where the brain needs all of the right amount of vitamins and nutrients it can get.
The WAPF is about as unscientific as you can get. They push old and outdated studies which only conform to their agenda. However, they do have good intentions. What Dr. Price saw when he visited the isolated peoples was that they had good dental hygiene despite not taking care of their teeth. This then inspired the two women who then started the WAPF. The WAPF may have been started with good intentions based on Dr. Price’s data, but it’s archaic in comparison to the type of data we have today. The diet pushed by the WAPF will lead to health implications and eventual death due to heart attack, cancer or some other type of disease correlated with high saturated fat intake. Most people become blind and have tunnel vision with their beliefs. No matter how many times they’re shown that they’re wrong and here is why they still hold on to their beliefs. It leads to artery clogging, which then does not allow correct blood flow which leads to heart attack or stroke and eventual death. These claims need to be thrown in the trash as soon as they come out, because due to the lack of nutritional information on the average American, they will see the word “Organization” and “.org” and think it’s a reputable place for information, where if you listen to it you will suffer severe health consequences.
Most people become blind and have tunnel vision with their beliefs. No matter how many times they’re shown that they’re wrong and here is why they still hold on to their beliefs. People don’t like to hear that they are wrong. When people are presented with contrary information, they gather support for their beliefs with “paradoxical enthusiasm”.This is because people have become so invested in their worldview that when provided contradictory evidence they lack the self-esteem to admit they were wrong and change their view. There is also something called “the backfire effect“, in which correcting of a wrong perception actually increases misperceptions.
The tunnel vision that people with huge misconceptions have, in this case nutrition, leads to them attempting to find anything they can to substantiate their claims, even if they’re objectively false. To take nutritional advice from one who is not a registered dietician (like Andrew Anglin and his pushing for the Paleo Diet, even when refuted on the clear false pretenses he makes in regards to his ‘articles’ like Europeans not evolving to eat tropical fruits and is therefore not natural [citation needed]. This also goes hand-in-hand with his look at the table showing the X/A ratio between Europeans, Africans, the Pan Ancestor and Bonobos, which he took to say that the African genome is closer to that of bonobos which is clearly untrue). Don’t follow what these ‘health gurus’ say because they are not up to date on the newest information and push shoddy and outdated ‘nutritional information’ to the average American who doesn’t know any better about nutrition.
This organization is dangerous to the health of those who give heed to their claims which are not based in science. It is dangerous to young infants whose parents believe their scientific double-talk. It is dangerous to those who drink raw milk and eat an excess of saturated fat which increases cancer rates. They have legitimate doctors who write in favor of them, yet one of the better-known names has been given statements by the FDA to stop illegal claims. The WAPF is full of snake oil salesman who want nothing more than to make a profit off of the nutritional ignorance of the average American. Get nutritional information from a verified source, not a place that denies science like the WAPF.
