
Home » Posts tagged 'overweight'
Tag Archives: overweight
Ethnic Differences in Sleep, Obesity, and Metabolic Syndromes
2300 words
Ethnic differences in the prevalence of obesity occur, majorly in part due to differences in the rates of metabolic syndrome (which is actually a few variables including high blood pressure, high blood sugar which leads to insulin resistance, excess visceral fat around the waist which is the ‘skinny fat‘ phenomenon, and abnormal blood pressure levels) and obesity. Ethnic differences in these variables do, in part, show how the three ethnies differ in rates of obesity. I will discuss the differences between each ethny in regards to metabolic syndrome and sleep and how it leads to the differences in ethnic obesity rates.
Sleep Differences
There is a ‘missing hour of sleep‘ when comparing blacks and whites. On average, blacks get 6.05 hours of sleep while whites get 6.85 hours of sleep. Of course, the same old racism argument comes up, which, if one ‘percieves’ discrimination, I wouldn’t doubt that it would have an effect on sleep due to a rise in cortisol, which affects sleep due to the raised levels making you restless and not able to fall asleep. Insulin levels then rise due to the rise in cortisol, which is the cause of obesity.
Some studies may try to say that racism and other forms of discrimination are a factor, without even thinking of genetic factors. Another study that Frost cites says that duration of deep sleep and duration of stage 2 (light sleep) is correlated correlated in African Americans with perceived discrimination. The authors defined ‘perceived discrimination’ as the extent to which one believes that their ethnic group have been discriminated against by society. Still even when controlling for discrimination, there were still marked differences between blacks and whites and how long they slept.
Frost then talks about how sleep patterns are heritable and cites studies done on Africans in Africa. One study found that there was an hour sleep difference between Ghanaians and Norwegians on the week days and between a quarter to half hour less on weekends. He shows another study showing that Nigerian college students sleep 6.2 hours a day while getting 70-minute naps in the afternoon.
Frost concludes that the African sleep patterns is normal on Africa. Africans are more active during the cooler times of the day and sleep during the bitter periods. Frost says those who evolved in more northerly climes are particularly adapted to a certain sleep pattern with the same holding true for Africans.
However, these sleep patterns in first world countries have negative effects on metabolism and rates of obesity.
Here are some more studies showing that blacks sleep less than whites:
The sleep of African Americans: a comparative review: The researchers found that blacks take longer to fall asleep than whites, report poorer sleep quality, have more light and less deep sleep, and nap more often and longer. This is a huge recipe for risk factors for obesity, and it shows in their demographics.
Unfair Treatment is associated with Poor Sleep in African American and Caucasian Adults: Pittsburgh SleepSCORE Project: This is one of the studies spoken about above that show that discrimination leads to less sleep. Though, it holds for both black and white adults. The researchers conclude:
Taken together, the confluence of perceived unfair treatment as a chronic stressor and poor sleep and the interplay between the two may have critical roles in long-term health problems.
African Genetic Ancestry is Associated with Sleep Depth in Older African Americans: The researchers hypothesized that “racial differences in sleep phenotypes would show an association with objectively measured individual genetic ancestry in AAs.” They conclude that the slow wave sleep may have genetic underpinnings.
Mexican Americans sleep less than do Mexican immigrants. US-born Mexicans are 40 percent more likely to be short sleepers. This is attenuated by environmental factors such as smoking and stress, which shorten the duration of sleep (smoking decreases the Body Set Weight, whereas cortisol along with insulin in tandem increase it).
Also, in this study by Roane et al (2014) looked at the link between sleep disturbances and stress in Mexican Americans (average age 55) and non-‘Hispanic’ whites (average age 66). Mexicans reported higher levels of sleep disturbance (25 percent) compared to whites (17 percent). They conclude that disturbed sleep was positively correlated with depression.
So both blacks and Mexicans sleep less than whites. These differences in sleep between these three ethnies also affect the prevalence of obesity in these populations.
Obesity and Sleep
It’s long been known that poor sleep habits make people fat. This is due to the effects of insulin and cortisol. Increased insulin comes before increased cortisol–increased insulin is the cause for obesity. Sleeping less is linked to obesity. Since, as described above, the three ethnies differ in sleep patterns, the same also holds true for obesity rates (Ogden at al, 2014). The trends are as follows: 67.3% for whites, 75.6% for blacks, and 77.9% for Hispanics. Though, sleep is only one factor involved with obesity.
Getting adequate sleep is extremely important. Not doing so can lead to a myriad of negative health implications:
Sleep is an important modulator of neuroendocrine function and glucose metabolism and sleep loss has been shown to result in metabolic and endocrine alterations, including decreased glucose tolerance, decreased insulin sensitivity, increased evening concentrations of cortisol, increased levels of ghrelin, decreased levels of leptin, and increased hunger and appetite. Recent epidemiological and laboratory evidence confirm previous findings of an association between sleep loss and increased risk of obesity.
So a lack of sleep leads to an increase in ghrelin levels, decreased levels of leptin (the same effects as caloric restriction over time), increased appetite and hunger, increased evening cortisol (which insulin spikes then follow), decreased insulin sensitivity (the cortisol brings it back up and most people are insulin resistant independent of diet), decreased glucose tolerance, etc. We can see that these ethnic differences in sleep, which are partly genetic in nature, can and would have great effects on metabolism, contributing to the ethnic differences in obesity rates.
And from Harvard:
For example, in the Nurses’ Health Study, researchers followed roughly 60,000 women for 16 years, asking them about their weight, sleep habits, diet, and other aspects of their lifestyle. (2) At the start of the study, all of the women were healthy, and none were obese; 16 years later,women who slept 5 hours or less per night had a 15 percent higher risk of becoming obese, compared to women who slept 7 hours per night. Short sleepers also had 30 percent higher risk of gaining 30 pounds over the course of the study, compared to women who got 7 hours of sleep per night.
Damn!! This, pretty much, mirrors the black-white difference. I’d love to see a racial breakdown of this cohort and will keep an eye out for one, but in the meantime, those who were short sleepers had a 30 percent higher risk of gaining 30 pounds over the course of the study in comparison to women who got 7 hours of sleep per night. Blacks are the most likely group to be overweight and obese in the US, and this data from the Nurses Health Study (which tons of data can be drawn from this study) shows one reason why, however the driver is cortisol > insulin > processed carbs > increased insulin > insulin resistance > increased insulin > vicious cycle > obesity. These differences in sleep almost perfectly mirror the ethnic differences in obesity.
There are several possible ways that sleep deprivation could increase the chances of becoming obese. (1) Sleep-deprived people may be too tired to exercise, decreasing the “calories burned” side of the weight-change equation. Or people who don’t get enough sleep may take in more calories than those who do, simply because they are awake longer and have more opportunities to eat; lack of sleep also disrupts the balance of key hormones that control appetite, so sleep-deprived people may be hungrier than those who get enough rest each night.
Ah the old ‘exercise to increase the Calories Out part of the equation’. however, Calories Out does not stay constant. This also rebuts the ‘Eat Less and Move More’ CICO (Calories In/Calories Out) model of obesity, showing that because it doesn’t take insulin into account, it’s doomed to fail.
Speaking of insulin, it’s about time I focused on metabolic syndrome.
Metabolic Syndrome
As I discussed in a previous post, Race, Obesity, Poverty, and IQ, metabolic differences exist between race/ethnicity. ‘Hispanics’ metabolize carbohydrates differently, blacks have a lower fiber intake (increased fiber protects against obesity, another correlate) while whites have a more high fat diet. Contrary to popular belief, dietary fat doesn’t make you fat as it’s the macro that spikes your insulin the least.
Diaz et al (2005) showed that minority populations are more likely to be affected by diabetes mellitus which may be due to less healthy diets and/or genetic factors. Using the National Health and Nutrition Survey for 1999-2000, they analyzed overweight, healthy adults, calculating dietary intake variables and insulin sensitivity by ethnicity. They characterized insulin resistance with fasted insulin, as those who are more likely to become insulin resistant have higher fasted insulin levels (levels taken after waking, with the subject being told not to eat the night before as to get a better reading of fasted insulin levels). Non-‘Hispanic’ whites had higher energy and fat intake while ‘Hispanics’ had higher carb intake with blacks having lower fiber intake. Blacks and ‘Hispanics’ were more likely to have lower insulin sensitivity. However, ‘Hispanics’ were more likely to have lower insulin sensitivity even after controlling for diet, showing that metabolic differences exist between ethnicities that affect carbohydrate metabolism which leads to higher rates of diabetes in those populations.
In ‘Hispanics’, several loci were discovered that play a role in hepatic (relating to the liver) fat content. Along with showing that ‘Hispanics’ have lower insulin (which due to low insulin, blood glucose builds up in the blood stream leading to diabetes) and showing that they metabolize glucose in the liver differently due to differing loci leading to more cases of fatty liver, this shows how and why ‘Hispanics’ have higher rates of Type II Diabetes Mellitus (TIIDM).
Since TIIDM affects Mexican Americans more, better measures to address their differences in carbohydrate metabolism need to be taken. Racial and ethnic differences in TIIDM are as follows:
7.6% of non-Hispanic whites
9.0% of Asian Americans
12.8% of Hispanics
13.2% of non-Hispanic blacks
15.9% of American Indians/Alaskan Natives
Whites eat a higher fat diet, which means a decrease in carbs. Asians eat white rice which spikes blood glucose eliciting a high insulin response leading to TIIDM, ‘Hispanics’, non-‘Hispanic’ blacks, and Indians and Alaskan Natives (I wish they separated Indians and Alaskan Natives as I’m almost positive that Alaskan natives have a lower rate) all eat high carb, low fat, low protein diets. Carbohydrates are a main staple, and since they spike insulin the most, they are the cause for obesity and TIIDM rates in these populations.
Turning my attention over to metabolic syndrome and blacks and whites, we can see that black women with PCOS have an increased risk for cardiovascular disease and metabolic syndrome in comparison to white women with PCOS. The researchers say that after controlling for age and body mass index (BMI) “black women with PCOS had a significantly increased prevalence of low high-density lipoprotein and high glucose. The general CVD risk was significantly increased in black adults with PCOS.” Though, a longitudinal study needs to be carried out to assess the independent impact of race and PCOS with CVD (Cardiovascular Disease).
Blacks have a higher chance to be diagnosed with metabolic syndrome since they are also at increased risk to have elevated blood pressure (hypertension), become obese, and be diabetic. This is due to their diet, which is due to their low IQ (obesity is correlated with intelligence), and different metabolism in comparison to whites.
There are also metabolic differences between race and sex. Fat oxidation is lower in black than white men and in African American men/women and white men/women, they have a lower metabolic rate!!! 24-hour energy expenditure is lower in black women in comparison to white women, whereas physical activity energy expenditure (PAEE) is the same as whites. Contrasted with women, black men had higher PAEE than white men. The authors conclude:
In conclusion, this comparative study of 24-h energy metabolism in African Americans and whites with use of a respiratory chamber not only confirms the previous findings from ventilated-hood studies of a lower resting metabolic rate, but also suggests a lower 24EE in African American women than in white women. Although only marginal ethnic differences in metabolic rate were found in men, African American men seem to have a lower rate of fat oxidation than do white men. The underlying mechanisms for these sex differences and the significance of these findings with respect to the development and maintenance of obesity remains to be investigated in longitudinal studies.
Metabolic Syndrome and Obesity
Race, Obesity, Poverty, and IQ
2100 words
America has a current and ongoing obesity epidemic. Some ethnicities are more likely to be obese or overweight than others due to lower intelligence which means a lack of ability to delay gratification, lack of ability to think into the future, lower funds which translates to eating more refined carbohydrates which means more blood glucose spikes which then leads to obesity as I will show. Insulin has a causal relationship with obesity so those who lack funds to buy healthier food then turn to refined foods high in carbohydrates as they are cheaper and more abundant in low-income neighborhoods.
Adult obesity rate by State (top 5) is: 1) Louisiana (36.2 percent), 2) Alabama (35.6), West Virginia (35.6), and Mississippi (35.6), and 5) Kentucky (34.6) with the 5 least obese States being 51) Colorado (20.2), 49) Hawaii (20.7), 48) Montana (23.6), 47) California (23.2), and 46) Massachusetts (24.3). Notice how the States with higher rates of obesity are in the South and the States with the lower rates are in the North, give or take. The average IQ for these States as follows: Lousiana: 95.3, Alabama: 95.7, West Virginia 98.7, Mississippi 94.2 (lowest IQ State in the country, largest black population at 37 percent), and Kentucky at 99.4. The average IQ for those States is 96.66. The average IQs for the States with the lowest obesity rates are: Colorado 101.6, Hawaii 95.6, Montana 103.4, California 95.5, and Massachusets 104.3 (highest IQ State). The average for these States being 100.08. So there is a 4 point IQ difference between the top 5 States with the highest and lowest percentage of obese people, which goes with the North/South gradient of higher IQ people living in the North and lower IQ people living in the South. Back in 2014, a California real estate group took 500,000 Tweets using a computer algorithm and estimated intelligence based on spelling, grammar, and word choice and found a difference in State by State intelligence. Notice how the further North you go the higher the average intelligence is, which is then correlated with the obesity levels in that State.
With poverty rates by State, we can see how the States in the South have less intelligent people in them which then correlates to the amount of obesity in the State. Though, there are some anomalies. West Virginia and Kentucky have a super majority of whites. This is easily explained by the fact that less intelligent whites live in those States, and since both the poverty rates and obesity rates are high, it follows that the State will be less intelligent than States that have more intelligent people and less obesity.
It is known that intelligence is correlated with obesity at around -.25 (Kanazawa, 2014). The negative correlation between intelligence and obesity means that they are inversely related so, on average, one with higher intelligence has less of a chance of being obese than one with lower intelligence. The States with the lowest IQ people having those with the highest BMIs corroborates this. In America, obesity rates by ethnicity are as follows: 67.3% for whites, 75.6% for blacks, and 77.9% for ‘Hispanics’.
Now that we know the average intelligence rates by State, the percentage of obese by State and the demographics by State, we can get into why obesity rates correlate with intelligence and race.
Diaz et al (2005) showed that minority populations are more likely to be affected by diabetes mellitus which may be due to less healthy diets and/or genetic factors. Using the National Health and Nutrition Survey for 1999-2000, they analyzed overweight, healthy adults, calculating dietary intake variables and insulin sensitivity by ethnicity. They characterized insulin resistance with fasted insulin, as those who are more likely to become insulin resistant have higher fasted insulin levels (levels taken after waking, with the subject being told not to eat the night before as to get a better reading of fasted insulin levels). Non-‘Hispanic’ whites had higher energy and fat intake while ‘Hispanics’ had higher carb intake with blacks having lower fiber intake. Blacks and ‘Hispanics’ were more likely to have lower insulin sensitivity. However, ‘Hispanics’ were more likely to have lower insulin sensitivity even after controlling for diet, showing that metabolic differences exist between ethnicities that affect carbohydrate metabolism which leads to higher rates of diabetes in those populations.
Drewnowski and Specter (2004) showed that 1) the highest rates of obesity are found in populations with the lowest incomes and education (correlated with IQ), 2) an inverse relationship between energy density and energy cost, 3) sweets and fats have higher energy density and are more palatable (food scientists work feverishly in labs to find out different combinations of foods to make them more palatable so we will eat more of them), and 4) poverty and food insecurity are associated with lower food expenditures, lower fruit and vegetable intake, and lower-quality diet. All of these data points show that those who are poor are more likely to be obese due to more energy-dense food being cheaper and fats and sugars being more palatable.
Now that I’ve shown the relationship between race and IQ by state, obesity rates by state, insulin sensitivity by race, and that those in poverty are more likely to be obese, I can now talk about the actual CAUSE of obesity: insulin.
The conventional wisdom is that if you consume more kcal than you expend, you will gain weight, whereas if you consume less than your daily needs you will lose weight. This has been unchallenged for 50 years. Also known as Calories In and Calories Out (CICO), this mantra “eat less and move more!!!” has been bleated over and over with horrendous results. The CICO model only concerns itself with calories and not insulin which is a causal factor in obesity.
In this study, participants in the basal insulin group which received the lowest average insulin dose gained the least average amount of weight at 4.2 pounds. Those on prandial insulin gained the most weight at 12.5 pounds. The intermediate group gained 10.3 pounds. More insulin, more weight gain. Moderate insulin, moderate weight gain. Low insulin, low weight gain.
Researchers compared a standard dose of insulin to tightly control blood sugars in type 1 diabetic patients. At the end of the 6 years, the study proved that intensive control of blood sugars resulted in fewer complications for those patients.
Though, in the high dose group, they gained on average 9.8 pounds more than those in the standard group.
More than 30 percent experienced major weight gain! Prior to the study, both groups were equal in weight. But the only difference was the amount of insulin administered. Were the ones given high levels of insulin all of a sudden more lazy? Were those who gained weight suddenly lacking in willpower? Were they lazier before the study? We’re they more gluttonous? No, no, and no!!
(source)
Finally, Henry et al (1993) took Type II diabetics and started them off with no insulin. They went from 0 units of insulin a day to 100 units at 6 months. As higher rates of insulin were administered, weight rose in the subjects. Insulin was given, people gained weight. A direct causal relationship (see figure above). However, what’s interesting about this study is that the researchers measured the amount of kcal ingested, the number of kcal ingested was reduced to 300 per day. Even as they took in less kcal, they gained 20 pounds! What’s going on here? Well, insulin is being administered and if you know anything about insulin it’s one of the hormones in the body that tells the body to either store fat or not burn it for energy. So what is occurring is the body is ramping down its metabolism in order for the subject to store more fat due to the exogenous insulin administered. Their TDEE dropped to about 1400 kcal, while they should have been losing weight on 1700 kcal! The CICO model predicts they should have lost weight, however, adaptive thermogenesis, better known as metabolic slow down, occurred which dropped the TDEE in order for the body to gain fat, as insulin directly causes obesity by signaling the body to store fat, so the body drops its metabolism in an attempt to do so.
Putting this all together, blacks and ‘Hispanics’ are more likely to be in poverty, have lower intelligence, and have higher rates of obesity and diabetes. Furthermore, blacks are more likely to have metabolic diseases (adaptive thermogenesis aka metabolic slowdown is a metabolic disease) which are related with obesity due to their muscle fiber typing which leads to lower maximal aerobic capacity (less blood and oxygen get around the body). Type II skeletal muscle fibers’ metabolic profile contributes to lower average aerobic capacity in blacks. It also is related to cardiometabolic diseases, in my opinion because they don’t have the muscle fiber typing to run long distances, thus increasing their aerobic capacity and VO2 max.
Due to the diets they consume, which, due to being in poverty and having lower intelligence, they consume more carbohydrates than whites, which jacks their blood glucose levels up and the body then releases insulin to drive the levels glucose in the body down. As insulin levels are spiked, the body becomes insulin resistant due to the low-quality diet. Over time, even a change in diet won’t fix the insulin resistance in the body. This is because since the body is insulin resistant it created more insulin which causes insulin resistance, a vicious cycle.
Poverty, intelligence and race both correlate with obesity, with the main factor being lower intelligence. Since those with lower IQs have a lack of foresight into the future, as well as a lower ability to delay gratification which also correlates with obesity, they cannot resist low-quality, high-carb food the same way one with a higher IQ can. This is seen with the Diaz et al study I linked, showing that whites have higher levels of fat intake, which means lower levels of carbohydrate intake in comparison to blacks and ‘Hispanics’. As I’ve shown, those in poverty (code word for low intelligence) ingest more refined carbohydrates, they have higher levels of obesity due to the constant spiking of their insulin, as I have shown with the 3 aforementioned studies. Since blacks and ‘Hispanics’ have lower levels of intelligence, they have lower levels of income which they then can only afford cheap, refined carbs. This leads to insulin being constantly spiked, and with how Americans eat nowadays (6 times a day, 3 meals and snacks in between), insulin is being spiked constantly with it only dipping down as the body goes into the fasted state while sleeping. This is why these populations are more likely to be obese, because they spike their insulin more. The main factor here, of course, is intelligence.
Another non-CICO cause for obesity is exposure to BPA in the womb. Researchers carried out BPA testing in three differing subjects: 375 babies invitro, (3rd trimester) children aged 3 (n=408) and aged 5 (n=518) (Hoepner, et al, 2016). They measured the children’s bodies as well as measuring body fat levels with bioelectrical impedance scales.Prenatal urinary BPA was positively associated with waist circumference as well as fat mass index, which was sex-specific. When analyzed separately, it was found that there were no associated outcomes in body fat for boys (however it does have an effect on testosterone), but there was for girls (this has to do with early onset puberty as well). They found that after controlling for SES and other environmental factors there was a positive correlation with fat mass index – a measure of body fat mass adjusted for height, body fat percentage and waist circumference. The researchers say that since there was no correlation between BPA and increased obesity, that prenatal exposure to BPA indicates greater vulnerability in that period. The sample was of blacks and Dominicans from New York City. Whites drink less bottled water, which has higher levels of BPA. Blacks and ‘Hispanics’ consume more, and thus have higher levels of obesity.
In conclusion, blacks and ‘Hispanics’ are more likely to be in poverty, have lower intelligence, higher rates of obesity and lower incomes. Due to lower incomes, cheap, refined carbohydrates is what they can afford in bulk as that’s mostly what’s around poor neighborhoods. Ingesting refined carbohydrates more often consistently jacks up blood glucose which the body then releases insulin to lower the levels. Over time, insulin resistance occurs, which then leads to obesity. As I’ve shown, there is a direct causal relationship between the amount of insulin administered and weight gain. With the aforementioned factors with these two populations, we can see how the hormonal theory of obesity fits in perfectly with what we know about these ethnic groups and the obesity rates within them. Since people in poverty gravitate more towards cheap and refined carbohydrates, they’re constantly spiking their insulin which, over time, leads to insulin resistance and obesity.
Black American Men with More African Ancestry Less Likely to Be Obese
1300 words
Black American men are the least likely male ethnic group to be overweight or obese in America (69.2 percent) compared to ‘Hispanic’ men (78.6 percent) and white men (71.4 percent) (Ogden et al, 2014). As a result of being less likely to be obese, black men as a whole suffer from diabetes and other diseases that are correlated with higher body fat. Conversely, for women the rate for white women is 63.2 percent, 77.2 percent for ‘Hispanic’ women and 82.4 percent for black women. Why do black men have lower rates of obesity and chronic health diseases?
Klimentidis et al (2016) set out to find why black men have lower rates of obesity than black women despite having the same socioeconomic and environmental factors. Using 2814 self-identified African Americans from the Atherosclerosis Risk in Communities study, they estimated each individual’s degree of African ancestry using 3,314 genetic markers. They then tested whether sex modifies the association of West African genetic ancestry and body mass index, waist circumference, and waist to hip ratio. Also, they adjusted for income and education as well as examined associations of ancestry with the phenotypes of males and females separately. They recreated their results with the Multi-Ethnic Study of Atherosclerosis (n= 1611 AA).
They discovered that West African ancestry is negatively correlated with obesity as well as central obesity, which is obesity around the midsection, among black men but not black women. Also noted, was that black men with more African ancestry had a lower waist to hip ratio and less central adiposity than black men with less African ancestry. They conclude that their results suggest that a combination of male gender and West African ancestry is correlated with protection against central obesity and suggests that a portion of the difference in obesity (13.2 percent difference) may be due, in part to genetic factors. The study also suggests that there are specific genetic and physiologic differences in African and European Americans.
This study confirms two things. 1) Black women are more likely to be obese than black men as well as the general population. 2) Black men have less of a chance of becoming obese or overweight as well as less of a chance of incurring the risks that come along with being obese or overweight. The degree of African ancestry is the cause in both black men and black women for these differences in the rate of overweight and obese individuals in both populations. One of my theories also got confirmed. Since obesity is partly genetic in African Americans, and black girls have an earlier menarche (period) than white girls due to higher body fat which activates the hormone leptin, which precedes an increase in body fat to prepare for eventual menstruation, I theorize that black girls have earlier menarche than white girls due to r/K Selection Theory. It’s an evolutionary advantage to be able to have children earlier, as the population dies younger.
Evolutionarily speaking, black men needed to be more fit in order to protect the clan from predators. This is also why blacks evolved narrower hips (Rushton, 1995). Higher body fat allows for more protection for a baby in vitro, which is why an increase in leptin precedes an increase in body fat, which then causes black girls to have an earlier puberty.
One of the questions I would like answered is whether it’s the actual degree of African ancestry that is the cause of black men being less likely to be obese or it’s the cause of higher degree of European ancestry. European American men do have a slightly higher risk of being overweight or obese than African American men, so there is some credence to this hypothesis. Three SNPs were found to be correlated with obesity in African American populations as well as European American populations; this could be one cause.
Wagner and Heyward (2000) discovered biological differences exist between blacks and whites. They reviewed the literature on the differences between blacks and whites in fat-free body mass (water, mineral, and protein) fat patterning and body dimensions and proportions. Blacks, in general, have greater bone mineral density and body protein content than do whites, resulting in lower fat-free bone density. They also note racial differences in the differences of subcutaneous body fat, which is the body fat that’s just below the skin, as opposed to visceral body fat which is found in the peritoneal cavity, which can be measured with calipers to give a rough estimate of total body fat adiposity. The conclusion reached in the study was that differences in FFB (fat-free body) was statistically significant between blacks and whites. They also have a greater BMC (bone mineral content) and BMD (bone mineral density) than do whites. They also argue that for a given BMI (body mass index), blacks might have less adiposity because they tend to be more mesomorphic. Researchers push for the development of racial-specific equations to better see differences in FFB.
With the above study noting that there is a substantial difference between blacks and whites in FFB, there may be some truth to a negative effect of European ancestry on blacks in terms of obesity acquisition. However, lower FFB in black men is one reason why black men can’t swim as well as whites.
One of the causes for both racial and gender discrepancies in obesity is genetic in origin. The difference between black men and black women is 13.2 percent whereas for white men and white women the difference is 8.2 percent. There is a clear genetic difference between races that is the cause for this discrepancy. Black men and black women have the same socioeconomics status and live in the same environment, so some of the differences in obesity noticed in this population must be genetic in origin.
Freedman et al (2004) observed that, as expected, black men were more likely to choose heavier figures as an ideal body for women than white men. Also expected was that both groups would choose figures with a low waist to hip ratio, but black men would choose a lower waist to hip ratio as ideal. They also show weight to be a more important cue than waist to hip ratio in mate selection as well as supporting the theory that black men’s preferences may serve as a protective factor against eating and body image pathology in black women.
To give an example of the above study in action, we can look at Mauritania. They force feed their women up to 16,000 kcal a day in an effort to make them obese, as that’s what is seen as attractive in their society. Mauritanian love songs also describe the ideal woman as fat. Obesity is so celebrated in their society that parents beam at the fact that their daughters look obese, as they have a better chance of getting partners.
The higher the degree of West African ancestry in black men, the lower the chance they have for obesity. I do wonder, though, if it’s because they have less European ancestry or because they have more African ancestry. Black men with more African ancestry are less likely to be obese than black men with less African ancestry, so there is a correlation there that I would like to see explored in the future. Differences in fat-free body mass have been noticed between blacks and whites, but this is one of the first studies to my knowledge that shows that genetic differences between black men and black women may be part of the cause for obesity differences in that population. Cultural differences in perception of beauty, of course, come into play in regards to differences between black and white men, however, the cause of black women having higher rates of obesity is due in part to genetic factors, which then leads to black men liking that as their beauty standard.
Science Daily: Mom’s Exposure to BPA During Pregnancy Can Put Her Baby on Course to Obesity
1750 words
Science Daily came out with an article today that exposure to BPA invitro for babies is correlated with obesity at age 7. 94 percent of the women tested had detectable levels of BPA. BPA is also linked with early onset puberty, which I will also speak on later in this article as it has implications for one of my theories.
I briefly touched on BPA in my article What’s the Cause of the Cucking of Europe? where I said:
I advise all of you (women included, there are many deleterious effects of BPA on the mother as well as the baby prenatally), to discontinue use of plastics with BPA in them.
The above-linked study shows that preeclampsia is correlated with elevated levels of BPA in the blood levels in the pregnant mothers, fetal blood, and the placenta. BPA was found to be elevated in mother’s fetal tissue with preeclampsia in comparison to the mothers with lower levels of BPA in their fetal tissue. I will come back to the BPA link with preeclampsia later in the article as it has implications for ethnic groups in America.
The paper, which was just released on the 17th, called Bisphenol A and Adiposity in an Inner-City Birth Cohort, carried out tested BPA in three differing subjects: 375 babies invitro, (3rd trimester) children aged 3 (n=408) and aged 5 (n=518) (Hoepner, et al, 2016). They measured the children’s bodies as well as measuring body fat levels with bioelectrical impedance scales.** Prenatal urinary BPA was positively associated with waist circumference as well as fat mass index, which was sex-specific. When analyzed separately, it was found that there were no associated outcomes in body fat for boys (however it does have an effect on testosterone), but there was for girls (this has to do with early onset puberty as well). They found that after controlling for SES and other environmental factors, they discovered that there was a positive correlation with fat mass index – a measure of body fat mass adjusted for height, body fat percentage and waist circumference. The researchers say that since there was no correlation between BPA and increased obesity, that prenatal exposure to BPA indicates greater vulnerability in that period.
The researchers then conclude that BPA exposure invitro “may be an important underlying factor in the obesity epidemic” and that “Endocrine disrupting chemicals like BPA may alter the baby’s metabolism and how fat cells are formed early in life.”
If true, this has huge implications for the way we look at the obesity epidemic in this country. Who are the most likely to be obese? “Hispanics” and blacks (Ogden et al, 2014).
Returning to what I brought up earlier about early onset puberty: in my article on the hormone leptin being a cause for earlier menarche in black girls, I noted that since black girls were more likely to be heavier as well as mature faster than white girls, that differences in leptin were the cause of differences in menarche between the two groups. Elevated levels of serum leptin were correlated with body fat and differences in maturation between the two groups. Differences remained, but lessened, after controlling for differences in fat mass, maturation, age, and physical fitness.
Since BPA is correlated with adiposity in children and black girls have earlier menarche DUE to there being a higher chance of black girls being overweight in comparison to white girls, BPA is yet another piece to the puzzle of this phenomena, along with, of course, evolution. Ingestion of BPA is an environmental factor, however, with these changes in body chemistry in the children invitro due to increased BPA consumption by the pregnant mothers, it leads to one cause that can be prevented from further occurring due to our new knowledge.
The study was carried out on a cohort from NYC. In 2010 in NYC, the city was: 44 percent white, 25.5 percent black, 12.7 percent Asian with the rest being filled out by ‘Hispanics’ (not a racial category) and mixed-race people. Even after they matched for SES and other environmental factors, these differences persisted. However, this study was only carried out on those women who self-identified as either Dominican (basically African) and black. To quote the researchers:
Women were included if they self-identified as either African American or Dominican and had resided in Northern Manhattan or the South Bronx for at least 1 year before pregnancy. Exclusion criteria included mother’s report of: cigarette smoking or use of other tobacco products during pregnancy, illicit drug use, diabetes, hypertension, known HIV, or a first prenatal visit after the 20th week of gestation.
So, we have a full sample of Caribbean Africans and African Americans in this study. What else can we learn about those two populations and their consumption of things with BPA in them?
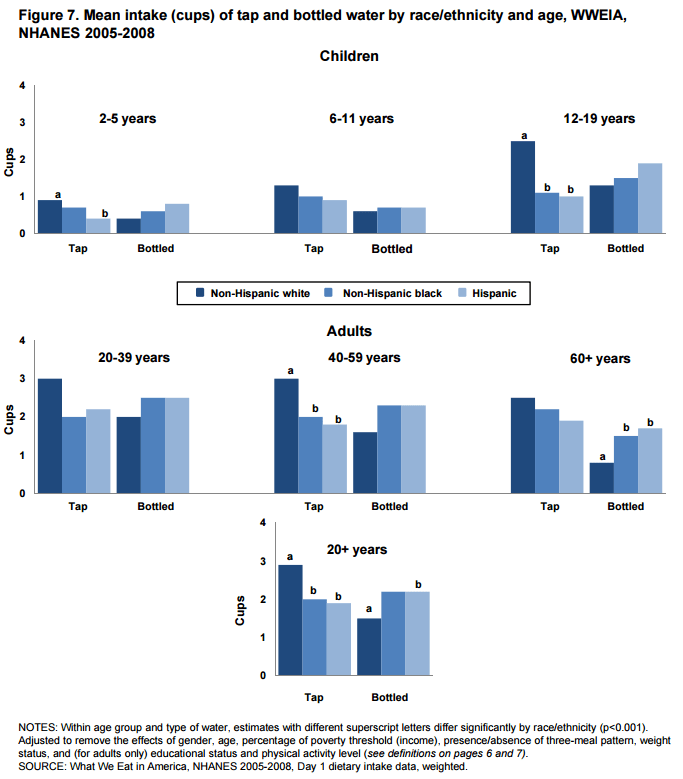
The above Figure (7) is taken from the U.S. Department of Agriculture and the Food Surveys Research Group study on differences in drinking tap and bottled water.in different populations in the country. As you can see in this figure (what is notable is the ages 12-19 and 20 to 60 in the table), whites at all age groups drink more tap water. Blacks and ‘Hispanics’ were pretty much even in consumption of bottled water. However, Mexican American girls, like black girls, are also entering puberty earlier. Since both populations have a substantial percentage of them overweight and obese (factor for serum leptin production which then causes early onset puberty), this again shows a strong correlation between body fat gain and early onset puberty. Moreover, this also shows that both Dominican and black populations consume more bottled water than do white populations, both populations are more likely to be obese or overweight (even after controlling for SES) which causes leptin production earlier causing periods to happen much sooner than in populations who drink less bottled water and use other products with BPA in them. .
Going back to preeclampsia, it is a condition that pregnant women develop that’s characterized by hypertension (high blood pressure) and protein in the urine. It’s known that black women suffer from it the most. More interestingly, over the past ten years, rates of preeclampsia have been increasing in the black female population. As the researchers note in the article, BPA is correlated with preeclampsia. Blacks have a higher rate and chance of being diagnosed with hypertension as well. All of these differing variables coalesce into our current obesity epidemic. With blacks and “Hispanics” being more likely to be overweight/obese drink more bottled water, have a higher risk for hypertension, higher risk for preeclampsia and having earlier menarche, these help explain, in part, racial/ethnic differences in obesity.
These differences can be attributed to consumption of bottled water, i.e., consuming things with made with and packaged in plastic as well as canned foods. From my experience with Dominican and black New Yorkers, they tend to have horrible lifestyles, tend to drink tons of bottled water and also tend to be overweight or obese at a higher rate in comparison to the general population. This leads to biologic factors changing (i.e., earlier menarche in younger girls) in these young girls, leading to devastating effects on their body chemistry.
This study, yet again, proves another underlying factor for obesity in certain populations in the country. And what do you know? It’s the populations that already have the highest rate of obesity in the country. When it becomes definitive that BPA consumption by pregnant mothers does lead to underlying factors in obesity. To quote the researchers: “Endocrine disrupting chemicals like BPA may alter the baby’s metabolism and how fat cells are formed early in life.” This will be HUGE for our understanding of underlying causes to obesity! Moreover, if (when) this is fully corroborated, it can then be said that by mothers exposing their children in the womb to excess levels of BPA, there is a chance that they are “giving their own choice to make their children have a higher chance of being obese, as they know the dangers of BPA consumption during pregnancy and all of the negative variables associated with it.”
This is an extremely interesting and important study for our understanding of obesity. Since BPA consumption invitro is correlated with higher fat mass index in girls at age 7, and since those girls who tend to be more overweight and obese than other populations, we can then say that BPA has a hand in obesity in children, which then causes serum leptin to be released, causing way menarche in these populations. An increase in sexual maturation has been linked to the obesity epidemic, which began around 60 years ago. The cause of this is due to the demonization of the fat macro and carbohydrates, all the while it was reversed. This destroyed insulin sensitivity for many Americans, leading to a huge majority of our health problems today.
In conclusion, underlying factors for obesity keep appearing. Due to racial/ethnic differences in bottled water consumption (one of the most common BPA products in households), which the effects of BPA may alter how fat cells are formed in early life, this accounts for, in part, excess adiposity in differing populations. These underlying factors could help show where some of these racial/ethnic differences in obesity come from. Since the two populations in the study (black American and Dominican) both have high levels of adiposity, both drink a lot of bottled water and both have earlier menarche than do whites (who drink LESS bottled water), this shows that some (a lot?) of the variation in obesity between ethnic/racial groupings can be explained by these underlying factors.
** I have one problem with this study. They assessed fat mass index with bioelectrical impedance.The machine sends a light electrical current through the body and measures the degree of resistance to the flow of the current, which body fat can then be estimated. Problems with measuring body fat this way are as follows: it depends on how hydrated you are, whether you exercised that day, when you last ate, even whether your feet are calloused. Most importantly, they vary depending on the machine as well. Two differing machines will give two differing estimates. This is my only problem with the study. I would like if, in a follow-up study, they would use the DXA scan or hydrostatic weighing. These two techniques would be much better than using bioelectrical impedance, as the variables that prevent bioelectrical impedance from being a good way to measure body fat don’t exist with the DXA scan or hydrostatic weighing.
Racial differences in Blood Donation
1050 words
Racial differences in blood donations pose a big problem for minorities. This has to do with altruism, which as I have covered extensively here, has a genetic basis. This pathological altruism has whites give and donate more than other races. This is due to evolving in colder climates with harsher environments, which high intellect evolved so our ancestors could survive. Why do minorities, blacks specifically, donate blood less?
Shaz and Hillyer (2010) observed that minorities were underrepresented as donors in the U.S., and that the cause was a higher deferral rate. Deferral reasons include: “low hemoglobin, travel, abnormal blood pressure, pulse or temperature, inability to find vein, tattoo/piercing, infection or taking antibiotics, and not being in good health.” They state that blood donation rate for blacks was 25 to 50 percent of that of white individuals.
Blacks have lower levels of hemoglobin than whites. The Red Cross defers people with low levels of hemoglobin. I don’t really know about blacks traveling too much. Abnormal blood pressure could be low or high blood pressure. Your blood pressure is determined by the amount of blood your heart pumps and the amount of resistance in your arteries.The more blood your heart pumps while arteries are clogged, the higher your blood pressure will be. The more fat and cholesterol that build up on the inner walls of the arteries, which I covered the other day, is called atherosclerosis. Called “hypertension” by the medical community, blacks also have a higher rate of this disease as well. Blacks have more genes expressed for coronary artery calcium, which is a strong indicator of atherosclerosis burden. Cardiovascular disease, more specifically coronary heart disease (CHD) is the leading cause of death for all Americans of all ages and ethnic groups (smoking is a leading cause of this). Blacks suffer the highest percentage of deaths due to CHD. And finally, inability to find a vein is due in large part to 75.6 percent of the black community being obese in America (69.2 percent for men and 82 percent for women).
Another reason for deferral is that all though Sickle Cell Disease isn’t strictly a racial disease, blacks do have the highest rate of it. Those with Sickle Cell Trait (SCT) can donate blood, though those with Sickle Cell Disease cannot.
Infections and antibiotics as well as not being in good health is yet another reason why blacks get deferred. This is due in part to “down-low bruthas” who are more likely to have diseases, and therefore cannot donate blood or plasma. Since homosexuals have some of the highest rates of disease in the country, it’s no surprise that blacks would be leading the pack in that subgroup of the country as well. This is a huge reason why blacks get deferred so much. However, in December of last year, the FDA lifted its lifetime ban of gays donating blood. I shutter to think what the deferral rates of blacks will look like in a few years due to this. That is also why “not being in good health” along with “infection or antibiotics” are such big reasons for deferrals. Blacks have all of the things they defer for, yet of course, allegations of prejudice and racism come about and the government has to step in to change things again, endangering the citizens of the country.
To quote from this AmRen article:
It has long been known that blood transfusions and organ transplants work best between people of the same race. Until the Second World War, stocks of blood were routinely segregated by race for this reason. Classification by race was ended when it was discovered to be “racist,” but blood banks are reinstituting segregation.
The distribution of the common blood types is different from race to race, and some rare types are unique to certain races. Only blacks have U negative blood; only whites have Vel negative or Lan negative blood. Dr. W. Laurence Marsh of the New York Blood Center justifies racial classification: “It makes no sense to screen 100,000 whites for U negative when no U negative white person has ever been found.”
So there is a problem with interracial blood transfusion, and they work better with co-ethnics than non-co-ethnics.
The Central Blood Bank states this about ethnicity and blood donation:
Though compatibility is not based on race, genetically similar blood is best for patients who need repeated or large volumes of blood transfusions, or those who have produced red blood cell antibodies for various diseases and conditions like sickle cell, heart disease and kidney disease.
It says that “compatibility isn’t based on race” then says immediately after “genetically similar blood is best for patients who need repeated or large volumes of blood transfusions. . .” The fact that there are differences in blood-type rate by ethnicity, and that there is a shortage of those blood types for blacks and “Hispanics” in America.
There are varying frequencies in white blood types are found in ethnicities throughout the country, and these varying frequencies in blood type are another reason why interethnic blood transfusion cannot happen; because the differing ethnic groups vary in the different blood types, there will be a low chance of having a certain blood type if it’s rare.
Another reason why blacks donate blood less is due to fear of needles and low iron. Low iron is due to vitamin and mineral deficinecies in diet. Combined with all of the aformentioned variables, this is why blacks get deferred so much. They just don’t donate as much either.
The disparity in differences in blood donation also come down to differences in giving between the races. Whites were seen to be more altruistic than were minorities in the study. This same altruistic behavior leads to more blood donations, but it also leads to the cucking of Europe due to the increase in pathological altruism.
Racial differences in blood donation are due to a whole host of factors, mainly being SCD and other diseases as a barrier for donation, as well as differing blood type frequencies between ethnic/racial groups. Since blacks have higher frequencies of SCD, SCT, and SCA this is another cause for their deferral rate. Being highly sexually active leads to higher disease acquisition, which is another reason less blacks donate blood. Moreover, blacks’ want to donate will not increase either; racial differences in blood donation and problems will persist to the forseeable future.
In Defense of Jason Richwine
3900 words
I came across two articles today, one from The Atlantic and the other from judgybitch.com. Both have attacked Jason Richwine’s dissertation in which he calls for a change to the US immigration policy to turn away low IQ immigrants and only accept high IQ ones. I agree fully with this (if it’s completely controlled, of course). This would drop crime as well as save us more money in welfare and other government programs that low IQ peoples take.
By 2050, 9 out of 10 people in the US will be obese or overweight and by 2020 80 percent of US men will be obese or overweight. This is due, in part, to an influx of those with lower IQs from South of the Border. Jason Richwine’s argument for testing immigrants will, in turn, lower obesity rates in America.
Dr. James Thompson noted how continued mass immigration from the South of the Border would decrease IQ, this is a real and pressing issue. A country is only as good as its majority population and by allowing all of these low IQ people into the country, our country will transform into theirs, which is ironic since that’s the exact thing they’re running away from. You cannot run away from genetics. The overall ‘Hispanic’-white gap is 10.2 points or .72 SDs. That will lower the average IQ of the country even more, and in turn, give us all a lowered quality of life. The average IQ of Mexico is 88 (Lynn and Vanhanen, 2002) so by allowing unfettered mass immigration without checking average IQs to see if they’ll be of any use to us as a country will lead to eventual irreversible effects if this isn’t stopped soon.
The first article I’ll look at is the one from The Atlantic:
Let’s start with the fact that there is no such thing as a direct test of general mental ability. What IQ tests measure directly is the test-taker’s display of particular cognitive skills: size of vocabulary, degree of reading comprehension, facility with analogies, and so on. Any conclusions about general mental ability are inferences drawn from the test-taker’s relative mastery of those various skills.
IQ tests test g or the general intelligence factor which encompasses all mental abilities. I guess the author of this piece has never heard of Raven’s Progressive Matrices. It’s a ‘culture free’ IQ test where the test is based on pattern recognition. No bias there.
Even then, if they don’t speak English and speak Spanish, they can get tests in their native language which are not biased. Gottfredson (1994) and 51 other eminent intelligence researchers signed a 25 point statement in which one of the statements was:
Intelligence tests are not culturally biased against American blacks or other native-born, English-speaking peoples in the U.S. Rather, IQ scores predict equally accurately for all such Americans, regardless of race and social class. Individuals who do not understand English well can be given either a nonverbal test or one in their native language.
They will be given the nonverbal test (RPM, see below) or one in their native language, which still test the same underlying concept of the general intelligence factor.
They found that being raised by high-SES (socioeconomic status) parents led to an IQ boost of between 12 and 16 points – a huge improvement that testifies to the powerful influence that upbringing can have.
False. See below.
A study of twins by psychologist Eric Turkheimer and colleagues that similarly tracked parents’ education, occupation, and income yielded especially striking results. Specifically, they found that the “heritability” of IQ – the degree to which IQ variations can be explained by genes – varies dramatically by socioeconomic class. Heritability among high-SES (socioeconomic status) kids was 0.72; in other words, genetic factors accounted for 72 percent of the variations in IQ, while shared environment accounted for only 15 percent. For low-SES kids, on the other hand, the relative influence of genes and environment was inverted: Estimated heritability was only 0.10, while shared environment explained 58 percent of IQ variations.
Turkheimer was right that he did find gene x environment interactions that made genetic influences weaker and shared environment stronger for those from poorer homes in comparison to those from more affluent homes. Though most studies show no interaction effects, or interactions vary significantly.
Other studies have shown that heritabilities are the same both within as well as between white and black samples. That led Jensen to label this the ‘default hypothesis’. Researchers analyzed full and half siblings from the NLSY on three Peabody Achievement Tests. 161 black full siblings, 106 pairs of black half siblings, 314 pairs of full white siblings and 53 pairs of white half-siblings. with measures in math and reading. The best fitting model for all of the data was by which the sources of the sources of the differences between those within race and the differences between races were the same, at 50 percent genetic and environmental. The combined model (50/50) best explains it, whereas the culture-only and genetics-only models are inadequate.
IQ tests are good measures of innate intelligence–if all other factors are held steady.
This is wrong. IQ tests are fine all around the world. RPM is one of the best out there and correlates with g between .8 and .9.
But if IQ tests are being used to compare individuals of wildly different backgrounds, then the variable of innate intelligence is not being tested in isolation. Instead, the scores will reflect some impossible-to-sort-out combination of ability and differences in opportunities and motivations. Let’s take a look at why that might be the case.
Intelligence – g – is the same across every population in the world.
Comparisons of IQ scores across ethnic groups, cultures, countries, or time periods founder on this basic problem: The cognitive skills that IQ tests assess are not used or valued to the same extent in all times and places
This is why they get re-standardized.
Indeed, the widespread usefulness of these skills is emphatically not the norm in human history. After all, IQ tests put great stress on reading ability and vocabulary, yet writing was invented only about 6,000 years ago – rather late in the day given that anatomically modern humans have been around for over 100,000 years. And as recently as two hundred years ago, only about 15 percent of people could read or write at all.
Doesn’t matter. See Raven’s Progressive Matrices above. The general intelligence factor is the same in all populations around the world. There are ways to give intelligence tests, such as RPM, to those who don’t read or write.
More generally, IQ tests reward the possession of abstract theoretical knowledge and a facility for formal analytical rigor.
Abstract thought is linked with intelligence. Those with higher IQs are more analytical than those with lower IQs.
To grasp how culturally contingent our current conception of intelligence is, just imagine how well you might do on an IQ test devised by Amazonian hunter-gatherers or medieval European peasants.
I touched on this in my refutation of Robert Sternberg. The concept of g does not change over time. The more intelligent you are, the better chance you’ll have to survive in those places.
Such skills are used more intensively in the most advanced economies than they are in the rest of the world. And within advanced societies, they are put to much greater use by the managers and professionals of the socioeconomic elite than by everybody else. As a result, American kids generally will have better opportunities to develop these skills than kids in, say, Mexico or Guatemala. And in America, the children of college-educated parents will have much better opportunities than working-class kids.
Those skills are used much more in advanced economies because of higher average innate intelligence. The children of college-educated parents have much better opportunities than working-class kids because intelligence is strongly linked to socioeconomics status.
Among the strongest evidence that IQ tests are testing not just innate ability, but the extent to which that innate ability has been put to work developing specific skills, is the remarkable “Flynn effect”: In the United States and many other countries, raw IQ scores have been rising about three points a decade. This rise is far too rapid to have a genetic cause. The best explanation for what’s going on is that increasing social complexity is expanding the use of the cognitive skills in question – and thus improving the opportunities for honing those skills.
Let’s say Flynn is right. The average black now is as intelligent as the average white in 1945. That’s supposed to show that the race difference in IQ is environmentally caused because there hasn’t been that much genetic change in the white population and the IQ has allegedly gone up 15 points. So, you can have a 15 point difference created by just an environmental change, no one knows why. Some think better nutrition or malnourished brain, etc. That’s also a fallacy. Just because a change in one group over time is due to an environmental change, doesn’t mean, or even make it probable, that a difference between 2 groups at the same time is due to an environmental change. The Flynn Effect make’s that highly unlikely and here’s why.
The Flynn Effect, assuming it’s real, has been acting completely uniformly in every population. Any country you ask, the rate of increase is 3 per decade. That means it’s an environmental factor that affects whites and blacks the same way as well as the whole world. And as a result of this uniform environmental factor, you have a difference in IQ that’s being preserved. That would suggest that the response on the parts of blacks and whites is due to some non-environment factors, a genetic factor, which is making the difference in IQ remain constant as the Flynn Effect goes into effect.
What makes it even more unlikely, in the last 60 years, their environments have become very similar since segregation. These differences don’t exist now, they go to the same schools by court order, same TV shows, same movies, basically same environment for both, and yet, that increasing similarity in the environment, the Flynn Effect, the IQ gap has remained intact. Which means whatever counts for the gap is genetic and not environmental. The more and more similar the environment, the less and less of the difference can be due to the environment and the more and more it must be due to genes. So this 15 point gap surviving these changes in the environment, seems more and more likely to be genetic in origin.
So because this ‘Effect’ is the same across all populations and the gap didn’t close, that means it’s genetic. If the gap persisted even when IQs were rising 3 points per year, the B-W gap has still persisted, proving that it’s genetic.
That is why the Flynn Effect is irrelevant. This “Effect”, has been a slight upward trend in IQ, around 3 points per decade, which, in my opinion, has to do with the advent of better nutrition and an industrialized society. The rise in IQ started around 1880, almost perfectly coinciding with the industrial revolution in America. Along with a more industrialized society, it’s possible to give most citizens in the country good enough nutrition to where they are not iodine deficient (adding iodine to our salt boosted Americans IQs), as well as being deficient in zinc, iron, protein and certain B vitamins which the effects of not getting enough leads to the brain not growing to its full potential, which in turn leads to a lower IQ.
One more point on the Flynn Effect. The Flynn Effect does not occur on g, as it is not a Jensen Effect. Rushton defines Jensen Effect as follows:
Significant correlations occurring between g-factor loadings and other variables have been dubbed “The Jensen effect”.
…
Thus the secular increase in test scores (the “Lynn±Flynn effect”) is not a “Jensen effect” nor is this the first time the discriminating power of the Jensen effect has been shown.
The Flynn effect is acutely embarrassing to those who leap from IQ score differences to claims of genetic differences in intelligence.
Not at all, since it’s easily explainable by better nutrition since the beginning of the industrial revolution. It’s also not even on g so why this gets discussed is beyond me.
Specifically, it is based on the ahistorical and ethnocentric assumption of a fixed relationship between the development of certain cognitive skills and raw mental ability. In truth, the skills associated with intelligence have changed over time–and unevenly through social space–as society evolves.
The relationship exists and there is a strong correlation between cognitive skills and raw mental ability. More intelligent people have better functioning societies than less intelligent people. This is an objective fact.
But contrary to the counsel of despair from hereditarians like Richwine, those deficits aren’t hard-wired. Progress in reducing achievement gaps will certainly not be easy, but a full review of the IQ evidence shows that it is possible. And it will be aided by policies, like immigration reform, that encourage the full integration of Hispanics into the American economic and cultural mainstream.
Jason Richwine is correct. Progress in achievement gaps will not close, barring the continued dysgenesis that America is facing. Immigration reform will not change anything. They don’t want to assimilate; they want to come and leech off of our Welfare State. The denial of genetics and scholastic achievement won’t be able to be held for long. In this study in which Robert Plomin was one of the researchers, it was found that 60 percent of the difference between individual 16-year-old students in the UK could be attributed to genetic factors. We know that IQ is linked to academic achievement and since that’s heritable as well, we will soon see that race and ethnic differences in IQ and academic achievement are, without a shadow of a doubt, are real and do not exist because of any economic deprivation or some other kind of non-biologic factors.
For the second article, from judgybitch.com, in which she only says one correct thing in it and it’s:
Here’s a little pet theory of mine I’d like to throw out, just for the hell of it. I think humans prefer lighter skin and hair and eye colors because those tend to be the result of recessive genes. A man with darker tones who has a child with a woman of lighter tones will almost always see his genes expressed in the children. Dark tones tend to be dominant. The preference for lighter skin is a natural paternity test.
This is called sexual selection, which is natural selection which arises for selection of traits in the opposite sex. Selecting for certain traits which the opposite sex found appealing, for example, is how long hair got sexually selected for outside of Africa along with selection for hair, eye, and skin color. Selecting for these traits had them become more prevalent and they eventually stayed due to intense selection for them.
For example, Eurasian women got selected for beauty and Eurasian men who got selected for intelligence as men had to be more intelligent in order to hunt for food. Conversely, African women gathered and hunted for food and became slightly more intelligent than African men who became the more attractive sex (Fuerle, 2008).
But other than this she is wrong.
You know what IS linked very strongly to lower IQs?
Malnutrition.
http://www.sciencedaily.com/releases/2004/11/041117005027.htm
http://www.ncbi.nlm.nih.gov/pubmed/2628311
http://www.nature.com/pr/journal/v5/n11/abs/pr1971371a.html
The idea is not even the slightest bit controversial. Children who are starved, especially in the earliest years of life, perform very poorly on IQ tests compared to peers who received adequate nutrition. Like, really poorly. IQ’s down around 60 (100 is average).
Let’s look at this world hunger map, shall we?
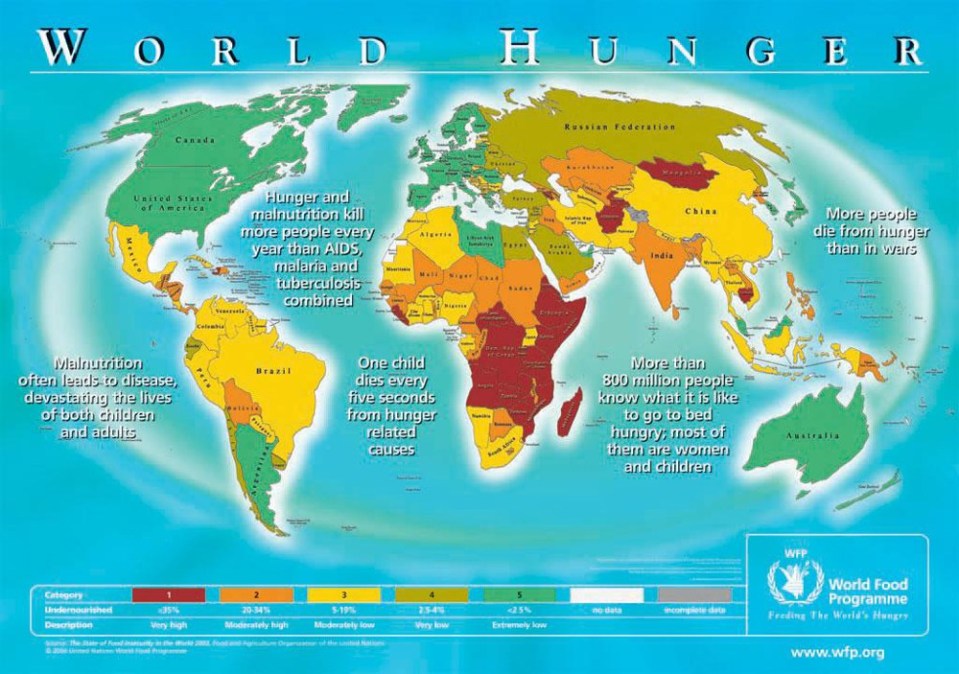
http://www.geographictravels.com/2008/07/world-hunger-map.html
Oh well now, would you look at that. Looks like it’s mostly black and Hispanic folks who are starving. And all those white folks are living life to the hilt, with full bellies and bright futures.
Must be a coincidence.
It’s not a coincidence. There is no coincidence that if you superimpose an IQ map over the world hunger map, that a super majority of the low IQ countries would have bad nutrition and be starving, whereas those higher IQ populations would have better nutrition and, therefore, higher IQs and lack of malnutrition and starvation. There are environmental factors involved in this, which I have gone through in my article IQ, Nutrition, Disease and Parasitic Load. Yes, those environmental variables decrease IQ; but in the case of Africa, if their full genotypic IQ were expressed in their phenotype, they would have an average IQ of 80, 9 points away from the lowest average European country which is Serbia at 89. They would then be able to have better functioning societies and not have to rely on outside aid. Though, their low IQs are the cause of evolution, those factors only cause about 10 points of difference (depending which of the variables I mentioned exist in those areas).
Let’s look at this map of food insecurity in the United States:
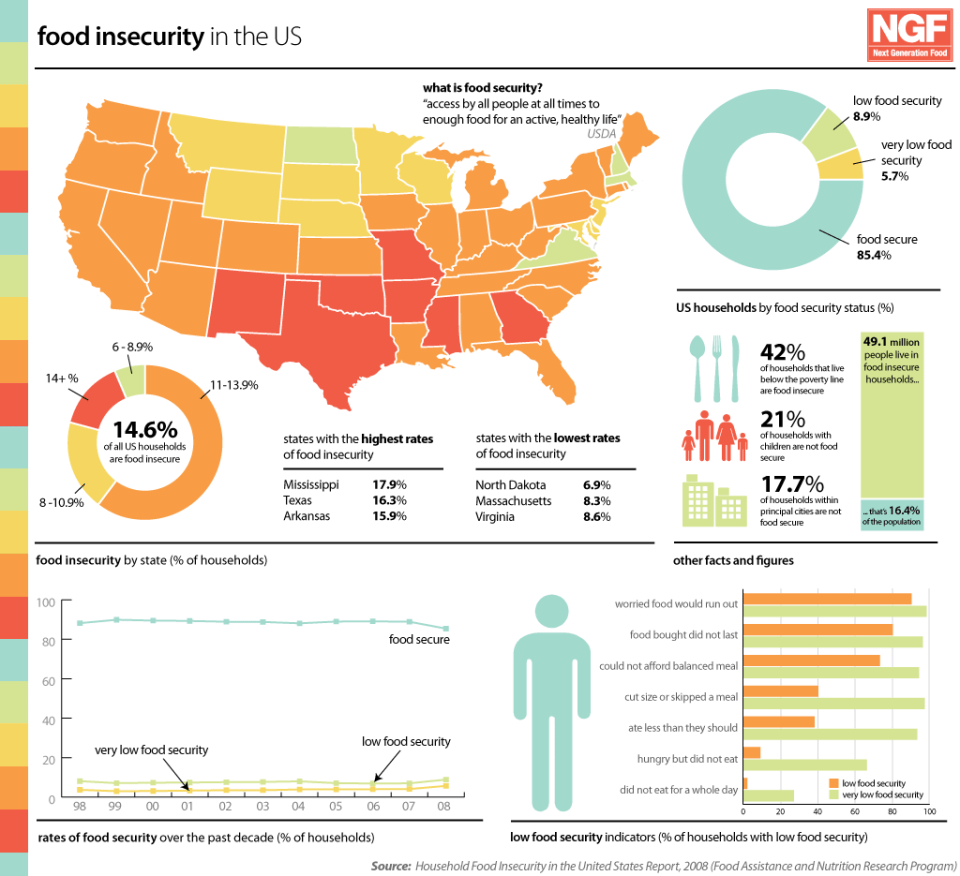
http://www.nextgenerationfood.com/news/food-insecurity-in-the-us/
Highest rates of food insecurity:
Mississippi
Texas
Arkansas
Lowest rates of food insecurity:
North Dakota
Massachusetts
Virginia
Gosh, I wonder where all the black and Hispanic people are? North Dakota, right?
According to the USDA, in a report titled Household Food Security in the United States in 2011, black and Hispanic families are more than twice as likely to experience food insecurity as white families (p. 11).
White 11.4% of families food insecure
Black 25.1%
Hispanic 26.2%
Gosh, I wonder where black and ‘Hispanic’ people are? Mississippi, Texas, and Arkansas right? What is the cause of the food insecurity? Lower intelligence. What is lower intelligence highly correlated with? Obesity.
If you keep in mind the fact that obesity (especially as the result of heavily processed, nutrient deficient junk foods) is also a form of malnutrition, it seems to me that there is an entirely different explanation for why certain racial groups might tend to perform lower on IQ tests.
Sure it is. A big cause for obesity is lowered intelligence (Kanazawa 2007). What he found was that those studies that concluded that obesity causes lowered intelligence only observed cross-sectional studies. Longitudinal studies that looked into the link between obesity and intelligence found that those who had low IQs since childhood then became obese later in life and that obesity does not lead to low IQ. The average IQ for an individual suffering from PWS is 65 (Butler, Lee and Whitman 2006, p. 13), so that is one reason they have a tendency to be obese. He states that those with IQs below 74 gained 5.19 BMI points, whereas those with IQs over above 126 gained 3.73 BMI points in 22 years, which is a statistically significant difference. Also noted, was that those at age 7 who had IQs above 125 had a 13.5 percent chance of being obese at age 51, whereas those with IQs below 74 at age 7 had a 31.9 percent chance of being obese. This clearly shows that those obese individuals who score low on IQ tests, more often than not, are obese because of their intelligence. The lack of ability to delay gratification is also correlated with low IQ (Mischel and Metzner, 1982).
Becoming obese is largely in part related to environmental factors, but there are correlates with obesity and genetic factors, as well as racial and ethnic differences in obesity, which are due, in part, to environmental as well as genetic factors. All of these factors fall back to a) lower intelligence, b) differing physiology and c) differing nutritional habits. Lower IQ is the main reason, though, for these differences which manifest itself as differences in scores of cognitive ability. Those with lower scores than have higher chances of having negative effects in life, such as low SES, higher chance of becoming obese and so on.
Correlation is not causation.
This is the liberals word phrase they use when they cannot contest data and know it so use the same old boring phrase. When you get the same result over and over using the scientific method, then it’s safe to say that the same results and conclusions that get brought up time and time again are real and cannot be explained away by the correlation does not mean causation line.
And furthermore, I haven’t read Richwine’s dissertation, nor do I plan to, so I don’t know if he offered any tentative explanations for his findings.
Didn’t even read it and is giving a critique of it. How does that work?
It looks to me like Richwine is a gigantic racist asshole, because he is using his findings to try and limit the opportunities for Hispanic people to come to the United States, because dumb spics.
Lower IQ people commit more crimes than do higher IQ people. This phenomenon is well-noted that those with lower intelligence commit crime, as the average IQ of a criminal in America, is 85, whereas the average IQ for a juvenile is 92. The average juvenile IQ is higher because more often than not, those who are habitual offenders in childhood become habitual offenders in adulthood, and at adulthood IQ drops from childhood where the environment was able to artificially boost their IQs.
What if I’m right? What if IQ differences are traceable to malnutrition? That would indicate a whole different set of interventions and policies than just turn them away.
You are part right, but that won’t put any big dent in any genetic/phenotypic IQ differences and still, mass immigration from South of the Border still wouldn’t be OK in the first place.
In shutting down the conversation about race and IQ, Harvard students are explicitly saying they don’t WANT to find a reason behind low performance on IQ tests amongst certain racial groups. They don’t CARE why some groups are not reaching their full human potential. They don’t give ONE SINGLE FUCK about anyone other than themselves. It could be as simple as making certain children have access to proper food and nutrition.
I at least give her credit for acknowledging the biological reality of race and the reality of IQ. But she thinks that malnutrition plays too big a part in the ethnic IQ gap than it does in reality.
As I have covered here before, people will do anything they can to deny the validity of IQ tests. However, their explanations cut it.
People who attempt to deny biological differences in intelligence because they strongly predict positive life outcomes will do anything to deny their validity. But that doesn’t change how strong a predictor they are in regards to predicting both positive and negative successes in life.
Those who attempt to deny any differences between races, like Chanda Chisala (I know you can see this Chanda, still waiting for a response to the criticism of your horrible article that “redneck genes” are the cause for the black-white IQ gap), who are wrong in their premises on the cause as well as how to fix the gap. They will do anything to attempt to explain away a gap which is, at least, 50 percent genetic in origin.
The attack on Jason Richwine is because, of course, he’s right. They don’t want to admit he is right so they do whatever they can to discredit his argument, by calling him a ‘racist’. But that doesn’t negate his data, and as seen above, any arguments against Richwine’s dissertation are unfounded.
Germany is going to begin IQ testing their immigrants, why can’t we?
Are There Genetic Causes for Obesity?
2500 words
We all know about the Healthy At Every Size Movement (HAES) and how they claim that genetics is the cause of them being overweight and or obese and that genetics is the cause that they cannot lose weight as well as other people. I’m not here today to defend that they are right and that’s why they can’t lose weight (because lets be honest, they have no idea what they’re talking about, nor can they reference any type of study that says it), nor am I here today to give any credence to the HAES movement. I’m here today to talk about genetic causes for obesity as well as causalities that people don’t talk about and believe that kcal in and kcal are the only factors in becoming obese (I have never, nor will I ever dispute that kcal in and out has been the biggest factor involving obesity, just there are underlying causes that people do not talk about, which is the a huge cause in keeping people obese). What people don’t understand is that there are underlying factors that no one talks about that lead to obesity.
When people say that there are no genetic underpinnings for obesity, they are speaking on a subject that they are extremely ignorant about. They always say “kcal in and out”. Right, which I have never disputed. Though, those same people cannot say a thing to the studies that I provide, because they cannot adapt to new information and just parrot the same things as if that disproves the studies that I link. Furthermore, obesity and diabetes (which there is a close relationship between the two), are both nowhere near close enough to being understood.
I have already covered here that ability to delay gratification has a genetic component, and that those with low ability to delay gratification, as noted in my post, had a higher chance of becoming obese than those with a better ability to delay gratification. Some people have said to me that the Marshmallow Experiment didn’t have anything to do with the ability to delay gratification, that it was something else entirely, but alas, the individual obviously said nothing more when I asked him to comment on the post so my readers can read the exchange.
You all know that I covered ethnicity and obesity, but I’m making this post to serve as a something to reference while in discussion with people, as well as educate people who don’t know about these studies.
As noted in my previous article on obesity, there are racial difference in obesity (that pretty much follow Rushton’s Rule). Of course there are socioeconomic factors that are involved there, but to say that there is no genetic component is intellectually dishonest. To believe that there are absolutely no genetic causes for obesity and that environmental factors means everything shows that that person has no idea what they are talking about.
According to a meta-study of twins and families, the heritability of BMI is between .75 and .82. This used mono and dizygotic twins, as well as having over 140 thousand participants. They observed 12 countries, all with differing racial/ethnic groups and the results were the same.
While in a discussion with someone, I got linked these studies: Obese toddlers have dramatically lowered IQ, Obese toddlers have dramatically lowered IQ 2 and Obesity lowers children’s IQ. This is hilarious. The causalities are completely reversed. I would love to hear the explanation for the physiological mechanism that has obesity lower IQ. Well, Satoshi Kanazawa tackled this in his study back in 2014, that low IQ leads to obesity, obesity doesn’t lead to low IQ.
A few of the highlights include:
- Cross-sectional studies conclude that obesity lowers IQ, whereas longitudinal studies conclude that those who become obese already have a low IQ since childhood
- Careful examination of longitudinal studies in Sweden, New Zealand and America clearly show that the casual direction goes from low IQ to obesity, not obesity to low IQ
- There is NO scientific evidence that shows that obesity leads to lowered IQ. There is, however, ample evidence, both in scientific theory as well as ample amounts of evidence that lower IQ people become obese
Individuals with IQs below 74 at 18 have BMI of 26.59 at 40, whereas those with IQs above 126 have BMI of 25.75 (P < 0.001). Similarly, there is a clear and monotonically negative association between intelligence at 18 and the BMI change from 18 to 40. Individuals with IQs below 74 gain 5.19 in BMI in 22 years, whereas those with IQs above 126 gain 3.73 (P < 0.001). Their conclusion remains identical even when they control for systolic and diastolic blood pressure, resting pulse rate, birth place, birth year, and education at conscription. Their results from a large population sample of Swedish men make it clear that it is adolescent intelligence that influences BMI in middle age, not the other way around
The fact of the matter is this: obesity does not lower IQ. Those with certain agendas would like you to believe that becoming obese drops IQ, whereas ample scientific data shows the opposite. Including this study which states that those in the cohort who became obese didn’t see a drop in IQ from childhood, instead, those individuals who became obese already had a lower IQ since childhood. You already know that I did not get a response to these studies. That’s because showing people that they’re wrong actually makes them believe their wrong beliefs more, especially if they have low self-confidence (how ironic).
There have been genes that have been found that are associated with binge eating. If a young adolescent has this particular variant on the FTO gene, they are 20 to 30 percent more likely to binge eat than those who don’t have the variant. This was observed in girls particularly, who were 30 percent more likely to binge eat if they had the variation.
Dr. Peter Atilla had a TED Talk on how obesity may be hiding an even more insidious problem. To quote from the transcript:
Yet when it came to a disease like diabetes that kills Americans eight times more frequently than melanoma, I never once questioned the conventional wisdom. I actually just assumed the pathologic sequence of events was settled science.
Three years later, I found out how wrong I was. But this time, I was the patient. Despite exercising three or four hours every single day, and following the food pyramid to the letter, I’d gained a lot of weight and developed something called metabolic syndrome. Some of you may have heard of this. I had become insulin-resistant.
Now, most researchers believe obesity is the cause of insulin resistance. Logically, then, if you want to treat insulin resistance, you get people to lose weight, right? You treat the obesity. But what if we have it backwards? What if obesity isn’t the cause of insulin resistance at all? In fact, what if it’s a symptom of a much deeper problem, the tip of a proverbial iceberg? I know it sounds crazy because we’re obviously in the midst of an obesity epidemic, but hear me out. What if obesity is a coping mechanism for a far more sinister problem going on underneath the cell? I’m not suggesting that obesity is benign, but what I am suggesting is it may be the lesser of two metabolic evils.
You can think of insulin resistance as the reduced capacity of our cells to partition fuel, as I alluded to a moment ago, taking those calories that we take in and burning some appropriately and storing some appropriately. When we become insulin-resistant, the homeostasis in that balance deviates from this state. So now, when insulin says to a cell, I want you to burn more energy than the cell considers safe, the cell, in effect, says, “No thanks, I’d actually rather store this energy.” And because fat cells are actually missing most of the complex cellular machinery found in other cells, it’s probably the safest place to store it. So for many of us, about 75 million Americans, the appropriate response to insulin resistance may actually be to store it as fat, not the reverse, getting insulin resistance in response to getting fat.
You can think of insulin as this master hormone that controls what our body does with the foods we eat,whether we burn it or store it. This is called fuel partitioning in the lingo. Now failure to produce enough insulin is incompatible with life. And insulin resistance, as its name suggests, is when your cells get increasingly resistant to the effect of insulin trying to do its job. Once you’re insulin-resistant, you’re on your way to getting diabetes, which is what happens when your pancreas can’t keep up with the resistance and make enough insulin.
But most important, I was left with these three burning questions that wouldn’t go away: How did this happen to me if I was supposedly doing everything right? If the conventional wisdom about nutrition had failed me, was it possible it was failing someone else? And underlying these questions, I became almost maniacally obsessed in trying to understand the real relationship between obesity and insulin resistance.
So what I’m suggesting is maybe we have the cause and effect wrong on obesity and insulin resistance.Maybe we should be asking ourselves, is it possible that insulin resistance causes weight gain and the diseases associated with obesity, at least in most people? What if being obese is just a metabolic response to something much more threatening, an underlying epidemic, the one we ought to be worried about?
Let’s look at some suggestive facts. We know that 30 million obese Americans in the United States don’t have insulin resistance. And by the way, they don’t appear to be at any greater risk of disease than lean people. Conversely, we know that six million lean people in the United States are insulin-resistant, and by the way, they appear to be at even greater risk for those metabolic diseases I mentioned a moment ago than their obese counterparts. Now I don’t know why, but it might be because, in their case, their cells haven’t actually figured out the right thing to do with that excess energy. So if you can be obese and not have insulin resistance, and you can be lean and have it, ******this suggests that obesity may just be a proxy for what’s going on.******
So what if we’re fighting the wrong war, fighting obesity rather than insulin resistance? Even worse, what if blaming the obese means we’re blaming the victims? What if some of our fundamental ideas about obesity are just wrong?
Personally, I can’t afford the luxury of arrogance anymore, let alone the luxury of certainty. I have my own ideas about what could be at the heart of this, but I’m wide open to others. Now, my hypothesis, because everybody always asks me, is this. If you ask yourself, what’s a cell trying to protect itself from when it becomes insulin resistant, the answer probably isn’t too much food. It’s more likely too much glucose: blood sugar. Now, we know that refined grains and starches elevate your blood sugar in the short run,and there’s even reason to believe that sugar may lead to insulin resistance directly. So if you put these physiological processes to work, I’d hypothesize that it might be our increased intake of refined grains, sugars and starches that’s driving this epidemic of obesity and diabetes, but through insulin resistance,you see, and not necessarily through just overeating and under-exercising.
The fact of the matter is this: we need to look at any and all causes to do with obesity. To fully understand this disease is to look at any and all factors involving it. To discard theories and make new ones, or just disregard what was looked at. People who say that we shouldn’t look at these types of things really have no idea what they’re talking about. To fully understand a problem, we need to look at any and all causes that may be underlying.
I’m currently writing a research paper on Prader-Willi’s Syndrome (which I will post here when I’m done with it), and as I was watching the documentary, a few things jumped out at me:
- They are infantile
- They clearly have a lack of ability to delay gratification
- Prader-Willi’s people have an IQ, on average of 70
- Due to being infantile, they have a lack of ability to delay gratification, so along with that, they have lower IQs which is correlated with lack of abstract thought
To say that these people “can control themselves” and they “just need to eat less” is dishonest, to say the least. Those people with disorders such as these really have no say in the matter.
In a follow-up to the Marshmallow Experiment, studies were done on those individuals they could still find 40 years later. What was found that those who lacked the ability to delay gratification in pre-school ended up becoming obese. We need to identify those children with low ability to delay gratification because it’s clear that those with the lack of ability to delay gratification end up becoming obese in adulthood.
This is a favorite of mine. People may say “Fat shaming is good!!! It leads to people thinking about what they’re doing and, in turn, they will lose weight!!!” How wrong that is. Present research indicates that in addition to poorer mental health outcomes, weight discrimination has implications for obesity. ******Rather than motivating people to lose weight, weight discrimination increases the risk for obesity.****** Why people think that making fun of people will lead to weight loss is beyond me.

Interestingly, a slightly different pattern emerged when the analyses were based on measured BMI. When the sample with measured weight and height was limited to participants who were overweight at baseline, the risk of obesity was a little stronger but essentially the same (OR = 2.18, 95% CI = 1.04–4.45). In contrast, when this sample was limited to normal weight participants at baseline, there was not enough data for the analysis: of the 14 participants in the normal weight category who reported weight discrimination, none became obese
Similar to weight gain, weight discrimination was associated with remaining obese over the period between the two assessments (see Table 1). That is, those who experienced discrimination based on their weight were over three times more likely to remain obese at follow-up, rather than drop below the obesity threshold, than those who did not experience such discrimination.
The evidence is clear: weight discrimination actually increases the problem that people actually laugh at and make fun of people for. How ironic is that?
In conclusion (I will add to this post as new research comes out), to say that there are no underlying causes of obesity is intellectually dishonest. There are clear underlying causes to this obesity epidemic, which we need to look at any and all of these causes to fully understand obesity better (which we are nowhere close to understanding this problem).
Ethnicity and Obesity Rates
1400 words
Figured I would take some time to talk about some Racial-Ethnic Disparities in obesity, and for as of right now (while the populations still show differentiation, it will be way different for all ethnic groups in 20 years with 9 out of 10 people being obese or overweight, and I would assume it would show the same levels of it in all populations), the ethnic-racial differences in the pattern as they apply to HBD.
To quote from the Food, Research and Action Clinic, which just did an overview of studies from the last year on the percentage, as well as racial-ethnic disparities on obesity:
Recent national data show that 82.0 percent of Black women and 77.2 percent of Hispanic women are overweight or obese compared to 63.2 percent of White women (Ogden et al., 2014).
Women as a whole are more likely to carry more fat mass than men, especially in their hips and around their waste, as estrogen distributes fat more around hips and the lower body, as it’s better for childbearing.
In addition, over half of Black women are obese (versus 37.1 percent of Black men and 32.8 percent of White women) (Ogden et al., 2014). Extreme obesity continues to be higher among women (8.3 percent) than men (4.4 percent), especially among Black women who have more than double the rates of extreme obesity as White and Hispanic women (16.4 percent versus 7.4 percent and 7.6 percent) (Ogden et al., 2014).
Black women have a higher rate of super obesity (over 40 percent BMI) due to EBT and other programs where they are able to buy high fat, high carb foods, which obviously leads to more weight gain. Double the fact that they are women and genetically predisposed to carry more fat than men, and you have your answer.
There is also a genetic component, which I will get in to later.
Rates of overweight or obesity are higher for Hispanic men (78.6 percent) compared to Black men (69.2 percent) and White men (71.4 percent) (Ogden et al., 2014).
Definite genetics at play here, with Hispanic men having a higher rate than black or Hispanic men. Studies show that Hispanics have fat-hoarding genes left over from their ancestors, genes that were required to live through cycles of feast and famine, which obviously have deleterious effects today. (Type 2 Diabetes goes hand in hand with obesity, which I will cover in a future post.)
This also goes to people who say that there are no genetic causalities for obesity, sure kcal in and kcal out are king, but it’s ignorant to think that there are no genetic causes for obesity.
There is a gene that is associated with waist circumference, as well as insulin resistance. Asian Americans have that, which also is a cause for obesity. Also, that same MCR4 sequence has been linked to binge eating.
Now to talk about some genes associated with obesity in African Americans.
In a study published back in 2013, researchers were looking for obesity genes in African Americans. The study, which involved more than 70,000 men and women of African descent, they were able to identify 3 SNPs that were associated with obesity and BMI in the sample population. What was also found, was that those same genetic sequences also heighten rates of obesity in peoples with no African ancestry, all of the genetic variants associated with obesity were also found in European populations. The same genes found in African populations did the same in European populations, and vice versa.
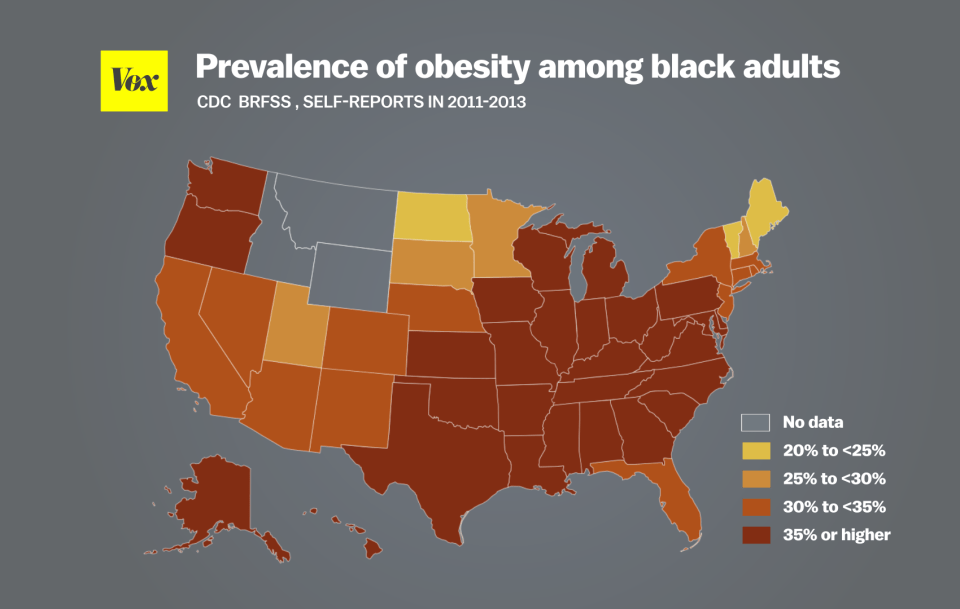
The map shown above shows obesity rates among black adults. Of course, where blacks are most prevalent, the southeast shows higher concentrations of obesity, of course, environmental factors are at play here (with ‘soul food’ being super high in fat and carbs, which make you hungry sooner).

This map shows the obesity rate of whites in America. Notice how most of the concentration of obese whites is in the southeast of America, which correlates with the lower IQ average of those states as seen in the map of IQ by State.
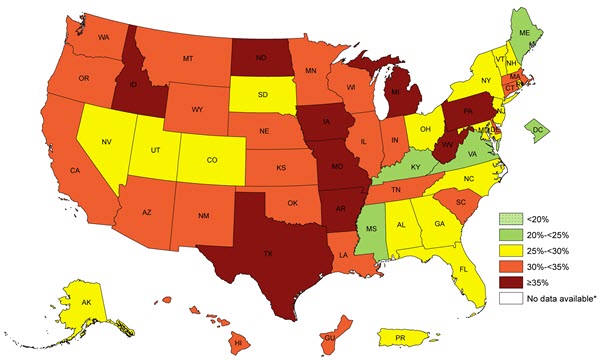
The above map shows obesity rates for Hispanics in America, again, matching up to where the majority of Hispanics in America are, furthering the causality of low IQ (see map).
Notice how there is no Asian obesity map? That’s because of their higher average IQ. Asian countries have some of the lowest prevalence of obesity and being overweight worldwide. Though, that is changing with a more ‘Americanized’ Asia, us bringing our shit lifestyle habits to other countries will increase the overall prevalence of obesity in the world, as well as America.
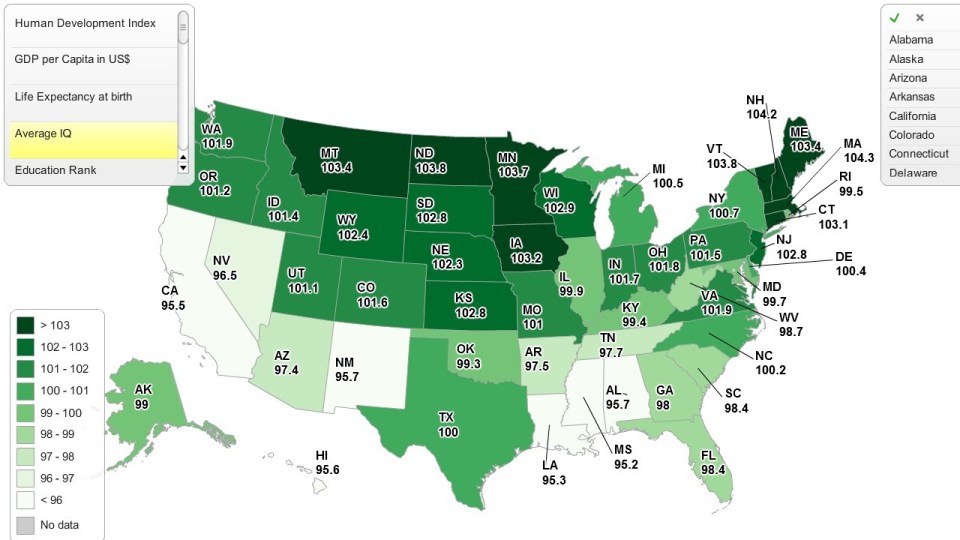
You can see the average IQ scores by State that it roughly matches up with all 3 maps. It’s not a coincidence. Lower IQ people don’t grasp what they are doing to their bodies by eating so much, leading to higher rates of obesity. I have already touched on how high fat diets slow microglia, which eats neuron connections in the brain, which is, yet again, another cause for lower IQ in obese/overweight people.
On top of some genetic reasons for obesity and predisposing populations to obesity, there are also environmental effects which cause differing levels in the populations. Socioeconomic status has a say as well (which is one of the only times this is applicable).
With differing levels of government assistance in groups, the more people who get government assistance are, for the most part, on the left side of the Bell Curve, which in turn means that they have a higher chance of being obese or overweight, due to low intellect. Low intelligence is correlated with abstract thought, so the low IQ person won’t be able to see what they are doing to their bodies in the now as well as into the future. That is the relationship between IQ and obesity.
Kanazawa also found, looking at a nationally representative sample of white Britons, (n=10,000), that IQ measured in childhood predicts obesity by age 51. (I will make a longer post on IQ and obesity in the future.)
Also, in a study that came out last month, when diets make us overweight/obese, it prompts normally active cells in our brain called ‘microglia’ to stop moving around so much and actually consume pathways to our neurons, which of course can sap intellect.
Percent of population on Food Stamps by Race:
White: 8.6%
Black: 43.8%
Hispanic: 17%
As you can see here, blacks have the highest rate of receiving food stamps in the country. The above quote is taken from the link.
It doesn’t follow the obesity trends of 67.3% for whites, 75.6% for blacks, and 77.9% for Hispanics, genetic factors take care of the rest for Hispanics to show their numbers in the obesity statistics. Obviously, we are being bombarded with tons of ads a day, telling us to eat all of this unhealthy food, and who is more likely to be home and not at work? Blacks and Hispanics. So that propaganda from the TV effects them more, to eat this or drink that, and they give in, due to their low IQ (which I have linked 2 Kanazawa studies to show reasons why).
In a meta-analysis of 140,525 people, they found the heritability of BMI was .75 to .82. So we can see that heritability of BMI is pretty large.
The causes for race/ethnic differences in obesity are partly genetic and partly environmental (socioeconomic), one would reason, in equal environments, that we would see Hispanics take the top spot, with blacks following behind and finally whites.
The greater your IQ, the lower your weight. Researchers found that people with a BMI of 20 or less were able to recall 56 percent of words in a vocabulary test while those with a BMI over 30 could only recall 44 percent. This directly goes hand in hand with my other link about microglia.
In this study, the cohort members who became obese had low IQ, as expected. Obese cohort members showed no excess decline in IQ, they instead had lower IQ since childhood. Further proving the low IQ/obesity correlation.
By 2020, 75 percent of Americans will be obese or overweight and by 2020, 80 percent of men are going to be overweight or obese. Now, the cause of these trends going up are due to more illegal/legal immigration from the south of the border. Though, without that, we would still be on our way to being a super obese country, because of the dysgenic effects in all populations, which cause a drop in IQ, which causes a gain in weight. Not to mention the propaganda that gets put to kids to want to eat sugary, unhealthy things.
