
Home » Posts tagged 'Race' (Page 3)
Tag Archives: Race
You Don’t Need Genes to Delineate Race
2100 words
Most race deniers say that race isn’t real because, as Lewontin (1972) and Rosenberg (2002) state, the within-group variation is larger than the between-group variation. Though, you can circumvent this claim by not even looking at genes/allele frequencies between races, you can show that race is real by looking at morphology, phenotype and geographic ancestry. This is one of Michael Hardimon’s race categories, the minimalist concept of race. This concept does not entail anything that we cannot physically ‘see’ with our eyes (e.g., mental and psychological traits are off the table). Using these concepts laid out by Hardimon can and does prove that race is real and useful without even arguing about any potential mental and psychological differences between human races.
Morphology
Morphology is one of the most simple tells for racial classification. Just by looking at average morphology between the races we can use attempt to use this data point as a premise in the argument that races exist.
East Asians are shorter with shorter limbs and have an endomorphic somatype. This is due to evolving in cold climate, as a smaller body and less surface area can be warmer much quicker than a larger body. This is a great example of Allen’s rule: that animals in colder climates will be smaller than animals in warmer climates. Using average morphology, of course, can show how the population in question evolved and where they evolved.
Regarding Europeans, they have an endomorphic somatype as well. This, again, is due to where they evolved. Morphology can tell us a lot about the evolution of a species. Though, East Asians and Europeans have similar morphologies due to evolving in similar climates. Like East Asians, Europeans have a wider pelvis in comparison to Africans, so this is yet another morphological variable we can use to show that race exists.
Finally, the largest group is ‘Africans’ who have the largest phenotypic and genetic diversity on earth. Generally, you can say that they’re tall, have long limbs and a short torso, which is due to evolving in the tropics. Furthermore, and perhaps most important, Africans have narrower pelves than East Asians and Europeans. This character is one of the most important regarding the reality of race because it’s one of the most noticeable, and we do notice in when it comes to sports competition because that certain type of morphology is conducive to athletic success. (Also read my recent article on strength and race and my article on somatype and race for more information on morphologic racial differences.)
Phenotype
Morphology is a part of the phenotype too, obviously, but there is a reason why it’s separated. As is true with morphology, different characters evolved due to cultural evolution (whether or not they adopted farming early) or evolution through natural selection, drift and mutation. Though, of course, favorable mutations in a certain environment will be passed on and eventually become a part of the characteristics of the population in question.
East Asians have the epicanthic fold, which probably evolved to protect the eye from the elements and UV rays on the Mongolian steppes. They also have softer features than Europeans and Africans, but this is not due to lower testosterone as is popularly stated. (Amusingly enough, there is a paper that stated that East Asians have Down Syndrome-like qualities due to their epicanthic folds to bring up one reason.) Even then, what some races find attractive or not can show how and why certain facial phenotypes evolved. To quote Gau et al (2018):
Compared with White women, East Asian women prefer a small, delicate and less robust face, lower position of double eyelid, more obtuse nasofrontal angle, rounder nose tip, smaller tip projection and slightly more protruded mandibular profile.
And they conclude:
The average faces are different from the attractive faces, while attractive faces differ according to race. In other words, the average facial and aesthetic criteria are different. We should use the attractive faces of a race to study that races aesthetic criteria.
We can use studies such as this to discern different facial phenotypes, which, again, proves that race exists.
The climate one’s ancestors evolved in dictates nose shape. In areas where it is extremely dry and also has a lot of heat, a larger mucous area is required to moisten inspired (inhaled) air, which is why a more flat and narrow nose is needed.
Zaidi et al (2017) write:
We find that width of the nares is correlated with temperature and absolute humidity, but not with relative humidity. We conclude that some aspects of nose shape may have indeed been driven by local adaptation to climate.
Though climate, of course, isn’t the only reason for differences in nose shape; sexual selection plays a part too, as seen in the above citation on facial preferences in East Asian and European women.
There are also differences in hirsutism between the races. Racial differences exist regarding upper lip hair, along with within-race differences (Javorsky et al, 2014). The self-reported races of African American, East Asian, Asian Indian, and ‘Hispanic’ predicted facial hair differences in women, but not how light their skin was. The women were from Los Angeles, USA; Rome, Italy; Akita, Japan; and London, England. Indian women had more hair than any other race, while European women had the least. Regarding within-race variation, Italian women had more hair on their upper lip than American and British women. Skin lightness was related to hair on the upper lip. (Also read my article The Evolution of Human Skin Variation for more information on racial differences in skin color.)
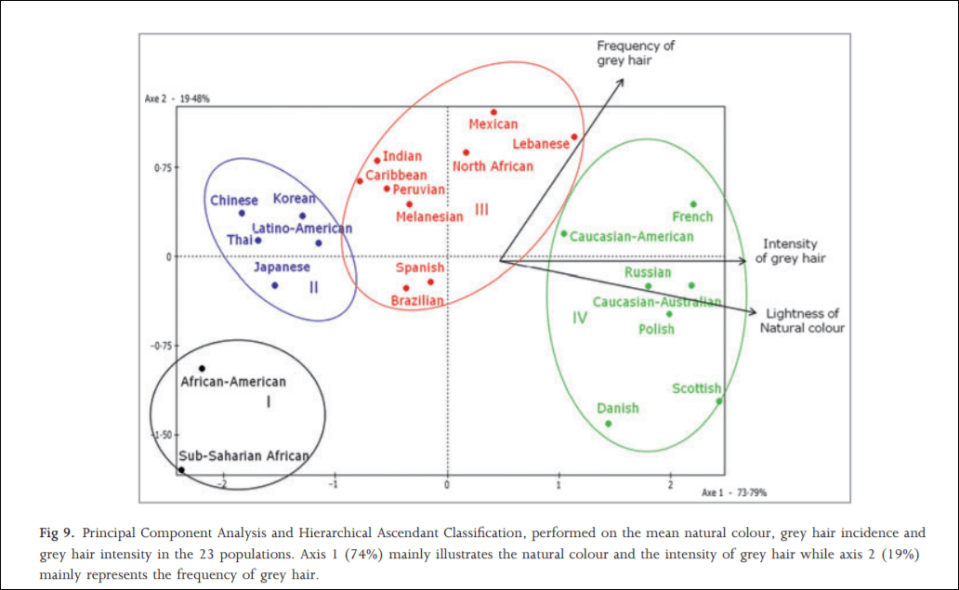
In 2012, an interesting study was carried out on hair greying on a sample population of a large number of the world’s ethnies titled Greying of the human hair: a worldwide survey, revisiting the ‘50’ rule of thumb. The objective of the study was to test the ’50-50-50′ rule; that at age 50, 50 percent of the population has at least 50 percent of their hair grey. Africans and Asians showed fewer grey hairs than whites who showed the most. The results imply that hair greyness varies by ethnicity/geographic origin, which is perfect for the argument laid out in this article. The global range for people over 50 with 50 percent or more of their hair grey was between 6 and 23 percent, far lower than what was originally hypothesized (Panhard, Lozano, and Loussouarn, 2012). They write on page 870:
With regard to the intensity of hair greying, the lowest values were found among African and Asian groups, especially Thai and Chinese, whereas the highest values were in subjects with the blondest hair (Polish, Scottish, Russian, Danish, CaucasianAustralian and French).
…
Altogether, these analyses clearly illustrate that the lowest incidences and intensities of grey hair are found in populations of the darkest hair whereas the highest intensities are found in populations with the lightest hair tones.
Actual hair diversity is much more concentrated in Europeans, however (Frost, 2005). (See Peter Frost’s article Why Do Europeans Have So Many Hair and Eye Colors?) It is largely due to sexual selection, with a few climatic factors thrown in. Dark hair, on the other hand, is a dominant trait, which is found all over the world.
Zhuang et al (2010) found significant differences in facial morphology between the races, writing:
African-Americans have statistically shorter, wider, and shallower noses than Caucasians. Hispanic workers have 14 facial features that are significantly larger than Caucasians, while their nose protrusion, height, and head length are significantly shorter. The other ethnic group was composed primarily of Asian subjects and has statistically different dimensions from Caucasians for 16 anthropometric values.
…
Statistically significant differences in facial anthropometric dimensions (P < 0.05) were noted between males and females, all racial/ethnic groups, and the subjects who were at least 45 years old when compared to workers between 18 and 29 years of age.
Blacks had statistically significant differences in lip and face length when compared to whites (whites had shorted lips than blacks who had longer lips than whites).
Brain size and cranial morphology, too, differs by geographic ancestry which is directly related to the climate where that population evolved (Beals, Smith, and Dodd, 1984). Most every trait that humans have—on average of course—differs by geographic location and the cause of this is evolution in these locations along with being a geographically isolated breeding population.
Geographic ancestry
The final piece to this argument is using where one’s recent ancestors came from. There are five major populations from a few geographic locales: Oceania, the Americas (‘Native Americans), Europe, Africa and East Asia. These geographic locales have peoples that evolved there and underwent different selective pressures due to their environment and their bodies evolved to better suit their environment, and so racial differences in morphology and phenotype occurred so the peoples could survive better in that location. No one part of this argument is more important than any other, though geographic ancestry is the final piece of the puzzle that brings everything together. Because race is correlated with morphology and phenotype, the geographic ancestry dictates what these characteristics look like.
Conclusion
Thus, this is the basic argument:
P1: Differing populations have differing phenotypes, including (but not limited to) facial structure, hair type/color, lip structure, skull size, brain size etc.
P2: Differing populations have differing morphology which, along with this population’s phenotype, evolved in response to climatic demands along with sexual selection.
P3: This population must originate from a distinct geographic location.
C: If all three of the above premises are true, then race—in the minimalist sense—exists and is biologically real.
This argument is extremely simple, and along with the papers cited above in support of the three premises and the ultimate conclusion, it will be extremely hard for race deniers to counter. We can say that P1 is logically sound because geographically isolated populations differ in the above-mentioned criteria. We can say that P2 is logically sound since differing populations have differing morphology (as I have discussed numerous times which leads to racial differences in sporting competition) such as differing trunk lengths, leg lengths, arm lengths and heights which are largely due to evolution in differing climates. We can say that P3 is logically sound because the populations that would satisfy P1 and P2 do come from geographically distinct locations; that is, they have a peculiar ancestry that they only share.
This concept of minimalist race from Michael Hardimon is (his) the racialist concept of race “stripped down to its barest bones” (Hardimon, 2017: 3). The minimalist concept of race, then, does not discuss any differences between populations that cannot be directly discerned with the naked eye. (Note: You can also use the above arguments/data laid out for the populationist concept of race, which, according to Hardimon (2017: 3) is: “A nonracialist (nonessentialist, nonhierarchical) candidate scientific concept that characterizes races as groups of populations belonging to biological lines of descent, distinguished by patterns of phenotypic differences, that trace back to geographically separated and extrinsically reproductively isolated founder populations.)
Minimalist race is biologically sound, grounded in genetics (though I have argued here that you don’t need genetics to define race), and is grounded in biology. Minimalist race is defined as characteristics of the group, not of the individual. Minimalist race are biologically real. Minimalist races exist because, as shown with the data presented in this article, phenotypic and morphologic traits are unevenly distributed throughout the world which then correlates with geographic ancestry. It cannot get any more simpler than that: race exists because differences in phenotype and morphology exist which then corresponds with geographic ancestry.
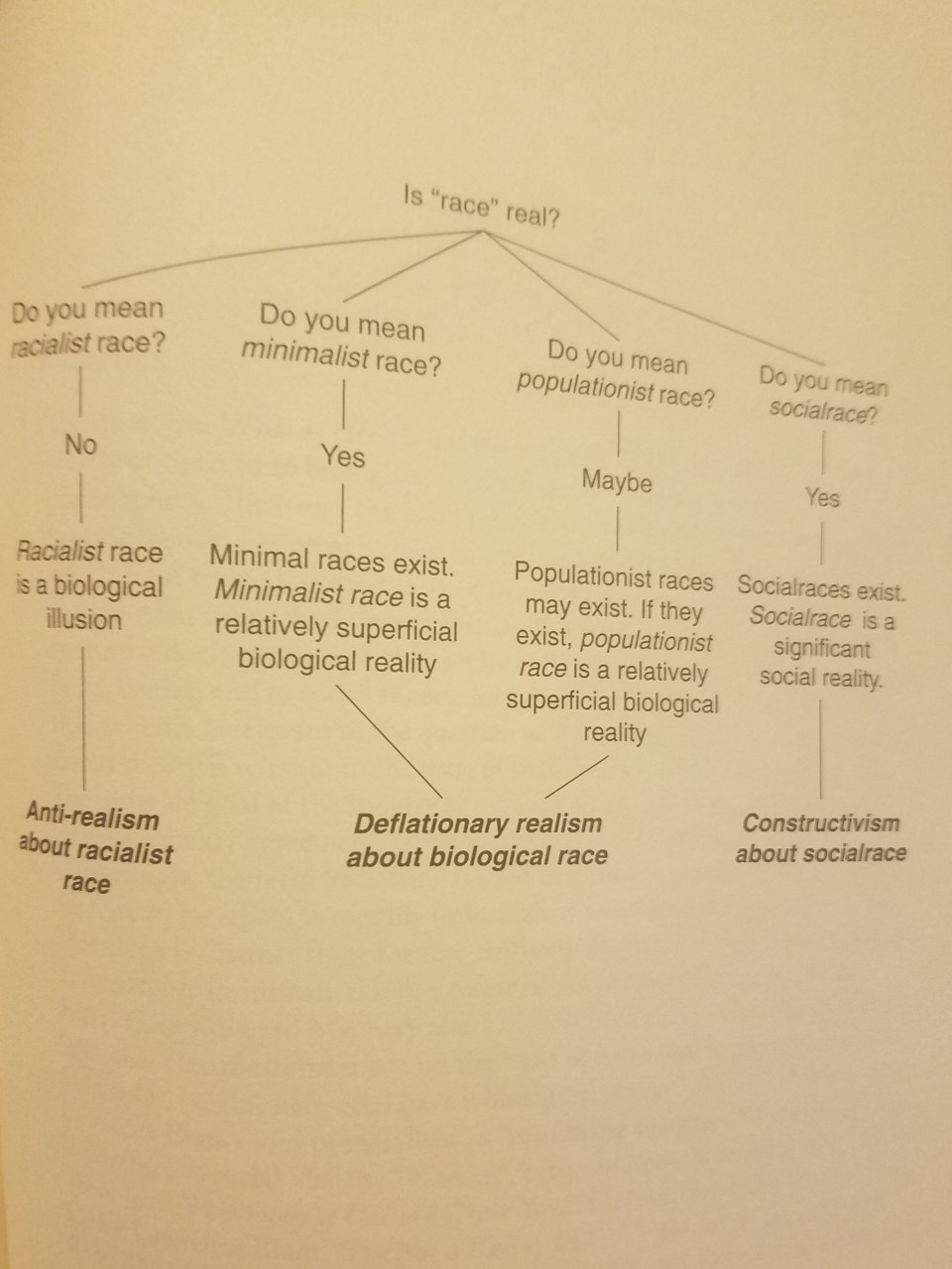
From Hardimon (2017: 177)\
No sane or logical person would deny the existence of race based on the criteria laid out in this article. We can also make another leap in logic and state that since minimalist races exist and are biologically real then geographic ancestry should be a guide when dealing with medicine and different minimalist races.
It is clear that race exists in the minimal sense; you do not need genes to show that race is real, nor that race has any utility in a medical context. This is important for race deniers to understand: genes are irrelevant when talking about the reality of race; you only need to just use your eyes and you’ll see that certain morphologies and phenotypes are distributed across geographic locations. It is also very easy to get someone to admit that races exist in this minimalist-biological sense. No one denies the existence of Africans, Europeans, ‘Native’ Indians, East Asians and Pacific Islanders. These populations differ in morphology and other physical characters which are unevenly distributed by geographic ancestry, so, therefore: minimialist races exist and are a biological reality.
Blood Pressure, Stress, and the Social Environment: On Black-White Differences in Blood Pressure
1800 words
Blood pressure (BP) is a physiological variable. Therefore since it is a physiological variable then it can be affected by environmental and social changes. How do racial differences come into play here, for instance? Since blacks face more (perceived) discrimination, then they should, on average, have higher BP levels than whites. This is what we find—but the effect is mostly seen in low-income blacks. How do psychosocial factors come into play here in the black-white BP gap?
BP is regulated by cardiac output, vascular resistance of blood flow, blood volume, arterial stiffness, and, of course, the individual’s emotional state which can decrease or increase BP. Neural mechanisms also exist which regulate BP (Chopra, Baby, and Jacob, 2011). Knowing how and why BP increases or decreases will have us better understand the social contexts of increased BP in low SES blacks.
BP is a complex physiological trait. It can go up and down due to what occurs in the immediate environment. Values of 120/80 mmHg are cited as ‘average’ values, but we have no idea what an ‘average’ BP is. Nevertheless—like most/all physiological variables—there is a wide range of what is considered ‘normal’. Due to the variance in human physiological systems, what is ‘normal’ for one individual is not ‘normal’ for another. Variation in BP (like, say, 120 SBP (systolic blood pressure) to 140 SBP) is ‘normal’. I believe even around 110 for SBP is within that range. For DPB (diastolic blood pressure) between 75 and 90 is within normal diurnal fluctuations due to activity/eating/etc (Taylor, Wilt, and Welch, 2011). BP, like testosterone, is one of those tricky variables to measure and so must be measured upon waking to see if there are any problems. So even for a trait like BP, there seems to be a ‘normal range’.
About 33 percent of blacks have hypertension (HTN) (Peters, Arojan, and Flack, 2006). Urban blacks are more likely to have higher BP levels than whites, but “At present, there is no complete explanation for these differences and further research is required” (Lindhorst et al, 2007). Low SES is correlated with higher levels of BP in black Americans—especially those with darker skin—but not Africans in Africa (Fuchs, 2011), suggesting that this is an American phenomenon that needs to be addressed. One good explanation, in my view, is the social environment. Physiological traits are extremely malleable due to the need to be able to ‘change gears’ in an instant, for instance to either fight or flight. Though, in our modernized world, these responses—mostly—have no need and so (due to our supposed civilized behavior), one’s BP rises due to social stress and other environmental factors and it is due to the urban environment.
What is the cause of high BP in blacks?
One explanation that has been given to explain higher rates of BP in blacks when compared to whites is discrimination. However, studies show mixed evidence on whether or not so-called discrimination raises BP (Couto, Goto, and Bastos, 2012). The same American effect (American blacks having higher BP than American whites) is seen even in the UK London area (Agyemang and Bhopal, 2003). This, yet again, is more evidence that the social environment drives these differences—again, regardless of whether or not any of the discrimination is real or imagined. Say most of it were imagined: it’d be irrelevant because the imagined discrimination leads to very real physiological outcomes in BP.
The country of birth also has an effect on BP. In one study, it was noted that Africans had significantly higher BP when compared to Asians (which is identical/lower) and native French living in France (Bahous et al, 2015). Ethnic differences in BP increase due to similar sodium intake is lower than what is usually cited (Graudal and Jurgens, 2015). However, other authors have pointed out that basing conclusions off of observational studies have problems, like the estimation of sodium intake being inaccurate since it’s a one-time measure; (Gunn et al, 2013; Cobb et al, 2014)
There is also evidence—along with pathways—that show how certain social activities work to lower stress and BP, including participation at church (Livingstone, Devine, and Moore, 1991). Black Americans can make other lifestyle changes in order to decrease BP, such as exercise and other lifestyle interventions. Redman, Baer, and Hicks state that “gene-environment interactions, job-related stress, racism, and other psychosocial factors to racial/ethnic disparities” need to be explored as causes for higher rates of HTN in blacks compared to whites. And with the knowledge of how all physiological systems work in terms of stress and other factors, should be explored as causes for this disparity.
Grim et al (1990) state that factors that influence high BP in blacks compared to whites are inherited and that is the major source of variation between these populations. However, the other mounting social/physiological evidence deserves an explanation; that is not inherited, and what we know about how our physiology responds to stress and discrimination—whether real or imagined—are extremely important and lead to extremely real, and important, outcomes in these populations. It is also argued that since blacks en route to America during the slave trade died from salt-depletive diseases, that blacks with a higher genetic propensity to absorb salt survived and this is why blacks have a higher propensity to absorb salt and are more ‘salt-sensitive’, which also could explain higher rates of HTN in American blacks compared to their cousins in Africa (Wilson and Grim, 1991). However, Curtin (1992) disputes this because “There is no evidence that diet or the resulting patterns of disease and demography among slaves in the American South were significantly different from those of other poor southerners”.
However, in regards to the social environment, Williams (1992) drives one of the best arguments I have encountered in this literature so far, stating that while genetic factors play a small part in regards to the BP gap between blacks and whites, social factors are arguably more important than genetic ones (and with our homeodynamic physiology, this does make sense). Dressler (1990) for instance, argues that skin color is a proxy for both social class and discrimination and these factors explain a large amount of the variation. Psychosocial variables can also explain heightened BP (Marmot, 1985; Cuffee et al, 2014). Yan et al (2003) also note how “time urgency/impatience” and “hostility” “were associated with a dose-response increase in the long-term risk of hypertension.” Henry (1988) also argues that calcium, obesity and genetic factors cannot be the aetiology of HTN in blacks, while also proposing that high sodium intakes are due to psychosocial stress (Williams, 1992: 136).
Obesity also leads to hypertension (Re, 2009) while blacks are more likely to be obese than whites, however, black American men with more African ancestry are less likely to be obese (Klimentidis et al, 2016). This would imply that the greater amount of African ancestry in American blacks both protects against obesity and along with it HTN. Williams (1992) makes a convincing argument that environmental and social factors are the cause for the black-white BP gap. And while genetic factors are important, no doubt, environmental and social factors are arguably more important to this debate.
Kulkarni et al (1998) show that increased stress leads to subsequent BP elevations which, over time, will lead to HTN. In a 2009 meta-analysis, Gasparin et al show how “individuals who had stronger responses to stressor tasks were 21% more likely to develop blood pressure increase when compared to those with less strong responses.”
Further, in support for the ‘perceived stress’ hypothesis in regards to blacks ‘perceiving’ stress and discrimination, “stress denial in combination with abdominal obesity, alcohol consumption, and smoking may be proxy for a high stress level” (Suter et al, 1997). Carroll et al (2001) also show how there are is “modest support for the hypothesis that heightened blood pressure reactions to mental stress contribute to the development of high blood pressure.” Sparrenberger et al (2009) also did a systematic review of observational studies, finding that “Acute stress is probably not a risk factor for hypertension. Chronic stress and particularly the non-adaptive response to stress are more likely causes of sustained elevation of blood pressure.”
Lastly, Langford (1981) shows that when SES is controlled for, the black-white BP disparity vanishes, implying that social and environmental—not genetic—factors are the cause for elevated HTN levels in black Americans. Sweet et al (2007) showed that for lighter-skinned blacks, as SES rose BP decreased while for darker-skinned blacks BP increased as SES did while implicating factors like ‘racism’ as the ultimate causes. This is solid evidence that both skin color and SES are predictors of higher prevalence of BP in black populations, and since other studies show that this is not noticed in higher class blacks, nor is this noticed in blacks in Africa, then the main causes of this disparity are social and environmental in nature.
(Non, Gravlee, and Mulligan, 2012). Their study suggests that educating black Americans on the dangers and preventative measures of high BP will reduce BP disparities between the races. This is in-line with Williams (1992) in that the social environment is the cause for the higher rates of BP. One hypothesis explored to explain why this effect with education was greater in blacks than whites was that BP-related factors, such as stress, poverty and racial discrimination (remember, even if no racial discrimination occurs, any so-called discrimination is in the eye of the beholder so that will contribute to a rise in physiologic variables) and maybe social isolation may be causes for this phenomenon. Future studies also must show how higher education causes lower BP, or if it only serves as other markers for the social environment. Nevertheless, this is an important study in our understanding of how and why the races differ in BP and it will go far to increase our understanding of this malady. This is a very convincing argument that education and not genetic ancestry cause disparities in BP between blacks and whites.
WebMD states that, of course, both environmental and genetic factors are at play in regards to black’s increased propensity for acquiring HTN. Fuchs (2011) also states that “They [environmental and behavioral factors] could act directly or by triggering mechanisms of blood pressure increase that are dormant in blacks living in Africa” and explain why black Americans have higher rates of BP than Africans in Africa. Further, race and ethnicity are independent predictors of HTN (Holmes et al, 2013).
Conclusion
Blacks and whites do differ in BP, and its aetiology is both complex and hard to untangle Genetic factors probably don’t account for a lot of this variance since Africans in Africa have low levels of BP compared to their black American cousins. Numerous lines of evidence shows that social and environmental factors are the cause, and so to change this, all people—especially blacks—should be educated on how to change these problems in our society. Whether discrimination is real or imagined, the effects of it lead to real physiological outcomes that then lead to increased health disparities between these populations.
MAOA, Race, and Crime: A Simple Relationship?
2400 words
When I first got into HBD back in 2012, one of the first things I came across—along with the research on racial IQs from Rushton, Lynn, Jensen et al—was that the races differed in a gene called MAOA-L, which has a frequency in Caucasians at .1 percent (Beaver et al, 2013), 54 percent in Chinese people (Lu et al, 2013; 56 percent in Maoris (Lea and Chambers 2007) while about 60-65 percent of Japanese people have the low-frequency version of this gene (Way and Lieberman, 2007).
So if these ethnies have a higher rate of this polymorphism and it is true that this gene causes crime, then the Chinese and Japanese should have the highest rates of crime in the world, since even apparently the effect of MAOA and violence and antisocial behavior is seen even without child abuse (Ficks and Waldman, 2014). Except East Asian countries have lower rates of crime (Rushton, 1995; Rushton and Whytney, 2002). Though, Japan’s low crime rate is relatively recent, and when compared with other countries on certain measures “Japan fares the same or worse when compared to other nations” (Barberet 2009, 198). This goes against a lot of HBD theory, and I will save that for another day. (Japan has a 99 percent prosecution rate, which could be due to low prosecutorial budgets; Ramseyer and Rasmusen, 2001. I will cover this in the future.)
The media fervor—as usual—gave the MAOA gene the nickname “the warrior gene“, which is extremely simplistic (I will have much more to say on ‘genes for’ any trait towards the end of the article). I will show how this is a very simplistic view.
The MAOA gene was first discovered in 1993 in a Dutch family who had a history of extreme violence going as far back as the 1890s. Since the discovery of this gene, it has been invoked as an ultimate cause of crime. However, as some hereditarians do note, MAOA only ’causes’ violence if one has a specific MAOA genotype and if they have been abused as a child (Caspi et al, 2002; Cohen et al, 2006; Beaver et al, 2009; Ferguson et al, 2011; Cicchetti, Rogosch, Thibodeau, 2012;). People have invoked these gene variants as ultimate causes of crime—that is, people who have the low-expressing MAOA variants are more likely to commit more crime—but the relationship is not so simple.
Maoris are more four times more likely to have the low-expressing gene variant than Europeans, the same holding for African Americans and Europeans (Lea and Chambers, 2007).
There is, however, a protective effect that protects whites (and not non-whites in certain cases) against antisocial behavior/violent attitudes if one has a certain genotype (Widom and Brzustowicz, 2006), though the authors write on page 688: “For non-whites, the effect of child abuse and neglect on the juvenile VASB was not significant (beta .08, SE .11, t 1.19, ns), whereas the effect of child maltreatment on lifetime VASB composite approached significance (beta .13, SE .12, t 1.86, p .06). For non-whites (see Figure 2), neither gene (MAOA) environment (child abuse and neglect) interaction was significant: juvenile VASB (beta .06, SE .28, t .67, ns) and lifetime VASB (beta .01, SE .29, t .14, ns).” So as you can see, there are mixed results. Whites seem to be protected against the effect of antisocial behavior and violence but only if they have a certain genotype (which implies that if they have the other genotype, then if abused they will show violent and antisocial behavior). So, we can see that the relationship between MAOA and criminal behavior is not as simple as some would make it out to be.
MAOA, like other genetic variants, of course, has been linked to numerous other traits. Steven J. Heine, author of the book DNA is Not Destiny: The Remarkable and Completely Misunderstood Relationship Between You and Your Genes:
However, any labels like “the warrior gene” are highly problematic because they suggest that the this gene is specifically associated with violence. It’s not, just as alleles from other genes do not only have one outcome. Pleiotropy is the term for how a single genetic variant can influence multiple different phenotypes. MAOA is highly pleiotropic: the traits and conditions potientially connected to the MAOA gene invlude Alzheimer’s. anoerxia, autism, body mass index, bone mineral density, chronic fatigue syndrome, depression, extraversion, hypertension, individualism, insomnia, intelligence, memory, neuroticism, obesity, openness to experience, persistence, restless leg syndrome, schizophrenia, social phobia, sudden infant death syndrome, time perception and voting behavior. (59) Perhaps it would be more fitting to call MAOA “the everything but the kitchen sink gene. (Heine, 2017: 195)
Something that I have not seen brought up when discussions of race, crime, and MAOA come up is that Japanese people have the highest chance—even higher than blacks, Maoris, and whites—to have the low repeat MAOA variant (Way and Lieberman) yet have lower rates of crime. So MAOA cannot possibly be a ‘main cause’ of crime. It is way more complex than that. “However intuitively satisfying it may be to explain cultural differences in violence in terms of genes“, Heine writes, “as of yet there is no direct evidence for this” (Heine, 2017: 196).
Numerous people have used ‘their genes’ in an attempt to get out of criminal acts that they have committed. A judge even knocked off one year off of a murder’s sentence since he found the evidence for the MAOA gene’s link to violence “particularly compelling.” I find it “particularly ridiculous” that the man got less time in jail than someone who ‘had a choice’ in his actions to murder someone. Doesn’t it seem ridiculous to you that someone gets less time in jail than someone else, all because he may have the ‘crime/warrior gene’?
Aspinwall, Brown, and Tabery (2012) showed that when evidence of a ‘biomechanic’ cause of violence/psychopathy was shown to the judges (n=191), that they reduced their sentences by almost one year if they were reading a story in which the accused was found to have the low-repeat MAOA allele (13.93 to 12.83 years). So, as you can see, this can sway judges’ perception into giving one a lighter sentence since they believe that the evidence shows that one ‘can not control themselves’, which results in the judge giving assailants lighter sentences because ‘it’s in their genes’.
Further, people would be more lenient on sentences for criminals who are found to have these ‘criminal genes’ than those who were found to not have them (Cheung and Heine, 2015). Monterosso, Royzman, and Schwartz (2010) also write: “Physiologically explained behavior was more likely to be characterized as “automatic,” and willpower and character were less likely to be cited as relevant to the behavior. Physiological explanations of undesirable behavior may mitigate blame by inviting nonteleological causal attributions.” So, clearly, most college students would give a lighter sentence if the individual in question were found to have ‘criminal genes’. But, if these genes really did ’cause’ crime, shouldn’t they be given heavier sentences to keep them on the inside more so those with the ‘non-criminal genes’ don’t have to suffer from the ‘genetically induced’ crime?
Heine (2017: 198-199) also writes:
But is someone really less any responsible for their actions if his or her genes are implicated? A problem with this argument is that we would be hard-pressed to find any actions that we engage in where our genes are not involved—our behaviors do not occur in any gene-free zones. Or, consider this: there actually is a particular genetic variant that, if you possess it, makes you about 40 times more likely to engage in same-sex homicides than those who possess a different variant. (66) It’s known as the Y chromosome—that is, people who possess it are biologically male. Given this, should we infer that Y chromosomes cause murders, and thus give a reduced sentence to anyone who is the carrier of such a chromosome because he is really not responsible for his actions? The philosopher Stephen Morse calls the tendency to excuse a crime because of a biological basis the “fundamental psycholegal error.” (67) The problem with this tendency is that it involves separating yout genes from yourself. Saying “my genes made me do it” doesn’t make sense because there is no “I” that is independent of your genetic makeup. But curiously, once genes are implicaed, people see, to feel that the accused is no longer fully in control of his or her actions.
Further, in the case of a child pornographer, one named Gary Cossey, the court said:
The court predicted that some fifty years from now Cossey’s offense conduct would likely be discovered to be caused by “a gene you were born with. And it’s not a gene you can get rid of.” The court expressed its belief that although Cossey was in therapy, it “can only lead, in my view, to a sincere effort on your part to control, but you can’t get rid of it. You are what you’re born with. And that’s the only explanation for what I see here.”
However, this judge punished Cossey more severely due to the ‘possibility’ that scientists may find ‘genes for’ child pornography use in 50 years. Cossey was then given another, unbiased judge, and was given a ‘more lenient’ sentence than the genetic determinist judge did.
Sean Last over at The Alternative Hypothesis is also a big believer in this so-called MAOA-race difference that explains racial differences in crime. However, as reviewed above (and as he writes), MAOA can be called the “everything but the kitchen sink gene” (Heine, 2017: 195), as I will touch on briefly below, to attribute ’causes’ to genes is not the right way to look at them. It’s not so easy to say that since one ‘has the warrior gene’ that they’d automatically be violent. Last cites a study saying that even those who have the MAOA allele who were not abused showed higher rates of violent behavior (Ficks and Waldman, 2014). They write (pg. 429):
The frequency of the ‘‘risk’’ allele in nonclinical samples of European ancestry ranges from 0.3 to 0.4, although the frequency of this allele in individuals of Asian and African ancestry appears to be substantially higher (*0.6 in both groups; Sabol et al. 1998).
So, why don’t Asians have higher rates of crime—along with blacks—if MAOA on its own causes violent and antisocial behavior? Next I know that someone would claim that “AHA! TESTOSTERONE ALSO MEDIATES THIS RELATIONSHIP!!” However, as I’ve talked about countless times (until I’m blue in the face), blacks do not have/have lower levels of testosterone than whites (Richards et al, 1992; Gapstur et al, 2002; Rohrmann et al, 2007; Mazur, 2009; Lopez et al, 2013; Hu et al, 2014; Richard et al, 2014). Though young black males have higher levels of testosterone due to the environment (honor culture) (Mazur, 2016). So that canard cannot be trotted out.
All in all, these simplistic and reductionist approaches to ‘figuring out’ the ’causes’ of crime do not make any sense. To point at one gene and say that this is ‘the cause’ of that do not make sense.
One last point on ‘genes as causes’ for behavior. This is something that deserves a piece of its own, but I will just provide a quote from Eva Jablonska and Marion Lamb’s book Evolution in Four Dimensions: Genetic, Epigenetic, Behavioral, and Symbolic Variation in the History of Life (Jablonska and Lamb, 2014: 17; read chapter one of the book here; I have the nook version so the page number may be different):
Although many psychiatrists, biochemists, and other scientists who are not geneticists (yet express themselves with remarkable facility on genetic issues) still use the language of genes as simple causal agents, and promise their audience rapid solutions to all sorts of problems, they are no more than propagandists whose knowledge or motives must be suspect. The geneticists themselves now think and talk (most of the time) in terms of genetic networks composed of tens or hundreds of genes and gene products, which interact with each other and together affect the development of a particular trait. They recognize that whether or not a trait (a sexual preference, for example) develops does not depend, in the majority of cases, on a difference in a single gene. It involves interactions among many genes, many proteins and other types of molecule, and the environment in which an individual develops.
So to say that those who have low-functioning MAOA variants have an ‘excuse’ as to why they commit crime is incorrect. I know that most people know this, but when you read some people’s writings on things like this it’s like they think that these singular genes/polymorphisms/etc cause these things on their own. In actuality, you need to look at how the whole system interacts with these things, and not reduce whole complex physiological systems to a sum of its parts. This is why implicating singular genes/polymorphisms as explanations for racial differences in crime does not make sense (as can be seen with the Japanese example).
To reduce behaviors simply to gene X and not look at the whole system does not make any sense. There are no ‘genes for’ anything, except a few Mendelian diseases (Ropers, 2010). Stating that certain genes ’cause’ X, as I have shown does not make sense and, wrongly, in my opinion, gives criminals less of a sentencing since judges find stuff like this ‘very compelling’. If that’s the case, why implicate any murderer? ‘Their genes made them do it’, right? Though, things are not that simple to implicate one gene as a cause for crime or any other complex behavior; in this sense—like for most things to do with the human body—holism makes way more sense and not reductionism. We need to look at how these genes that are ‘implicated’ in criminal behavior interact with the whole system. Only then can we understand the causes of criminal behavior. Looking at singular genes impedes us from figuring out the true underlying reasons why people commit crime.
Remember: we can’t blame “warrior genes” for violent crime. If someone does have a ‘genetic predisposition to crime’ from the MAOA gene, then wouldn’t it make more sense to give them more time? Though, the relationship is not so simple as I have covered. So to close, there is no ‘simple relationship’ between race, crime and MAOA. Not in the way that other hereditarians would like you to believe. Because if this relationship were so simple, then East Asians (Chinese, Japanese) would have the highest rates of crime, and they do not.
No, Black Women Do Not Have Higher Testosterone than White Women (And More On Hereditarian Claims on Racial Testosterone Differences)
1850 words
It has been over a year since I wrote the article Black Women and Testosterone, and I really regret it. Yes, I did believe that black women had higher levels of testosterone than white women due to one flimsy study and another article on pregnant black women. I then wised up to the truth about testosterone and aggression/crime/race/sex and revised the articles (like I have done with r/K selection theory). However, after I revised my views on the supposed differences in testosterone between black men/white men and black women/white women, people still cite the article, disregarding the disclaimer at the top of the article. I quoted Mazur (2016), who writes (emphasis mine):
The pattern [high testosterone] is not seen among teenage boys or among females.
…
There is no indication of inordinately high T among young black women with low education.
…
Honor cultures are cast as male affairs, but with T data in hand for both sexes, it is worth exploring whether or not a similar pattern exists among women. Mean T was calculated as a function of age for the four combinations of race and education used in Table 1 but now for women. All plots show T declining with age, from about 35 ng/dL in the 20–29 age group to about 20 ng/dL among women 60 years and older. The four plots essentially overlap without discernible differences among them. Given the high skew of T among adult females, both raw and ln-transformed values were analyzed with similar results. There is no indication of inordinately high T among young black women with low education.
…
In the present study, at least, the sexes differ because the very high T seen among young black men with low education does not occur among young black women with low education.
This is very clear… Mazur (2016) analyzed the NHANES 2011-2012 data and this is what he found. I understand that most HBD bloggers do believe this, well, like a lot of their strong assertions (which I have rebutted myself), they’re wrong. They don’t get it. They do not understand the hormone.
The reason why I’m finally writing this (which is long overdue) is that I saw a referral from this website today: https://www.minds.com/RedPillTV who writes about the aforementioned black women and testosterone article:
It is known that blacks have the highest levels of testosterone out of the major races of humanity. However, what’s not known is that black women have higher rates than white women. The same evolutionary factors that make it possible for black men to have high testosterone make it possible for women as well.
https://notpoliticallycorrect.me/2016/09/06/black-women-and-testosterone/
…..No. It seems that people just scroll on by the disclaimer at the top that is bolded and italicized and just go to the (now defunct) article and attempt to prove their assertion that black women have higher testosterone than white women with an article that I have stated myself I no longer believe and have provided the rationale/data for the position. This shows that people have their own biases and no matter what the author writes about their views that have changed due to good arguments/data, they will still attempt to use the article to prove their assertion.
I’ve written at length that testosterone does not cause 1) aggression, 2) crime and 3) prostate cancer. People are scared of testosterone mostly due to the media fervor of any story that may have a hint of ‘toxic masculinity’. They (most alt-righters) are scared of it because of Lynn/Rushton/Templer/Kanazawa bullshit on the hormone. Richard Lynn doesn’t know what he’s talking about on testosterone. No, Europeans did not need lower levels of aggression in the cold; Africans didn’t need higher levels of aggression (relative to Europeans) to survive in the tropics. The theory that supposed differential testosterone differences between the races are “the physiological basis in males of the racial differences in sexual drive which form the core of the different r/K reproduction strategies documented by J.P. Rushton” (Lynn, 1990: 1203). The races, on average, do not differ in testosterone as I have extensively documented. So hereditarians like Lynn and others need to look for other reasons to explain blacks’ higher rate of sexual activity.
Rushton’s views on the testosterone and supposed r/K continuum have been summarily rebutted by me. These psychologists’ views on the hormone (that they don’t understand the production of nor do they understand the true reality of the differences between the races) are why people are afraid of testosterone. No, testosterone is not some ‘master switch’ as Rushton (1999) asserts. Rushton asserts that racial differences in temperament are mediated by the hormone testosterone. He further dives into this assertion stating “Testosterone level correlates with temperament, self-concept, aggression, altruism, crime, and sexuality, in women as well as in men (Harris, Rushton, Hampson, & Jackson, 1996). It may ‘correlate’ with aggression and crime, but as I have documented, they do not cause either.
The aggression/testosterone correlation is only .08 (Archer, Graham-Kevan, and Davies, 2005). Furthermore, the diurnal variation in testosterone does not directly correlate to when testosterone levels are highest in the day (at 8 am and drop thereafter), with adults peaking in crime at 10 pm and kids at 3 pm, with rises at 8 pm and 12 pm (not surprisingly, kids go in to school around 8 am, go to recess at 12 and leave at 3).

(Source: The Office of Juvenile Justice and Delinquency Prevention (OJJDP))
If you’ve read as much Rushton as I have, you’ll notice that he begins to sound like a broken record when talking about certain things. One of the most telling is Rushton’s repeated assertions that blacks average 3-19 percent higher testosterone than whites. The 3 percent number comes from Ellis and Nyborg (1992) and the 19 percent number comes from Ross et al (1986) (which Rushton should know that after adjustments for confounding, it decreased to 13 percent). These are the only studies that hereditarians ever cite for these claims that blacks average higher testosterone than whites. That seems a bit fishy to me. Cite a 30-year-old study along with a 25-year-old study (with such huge variation from Rushton and those who cite him for this matter—3-19 percent!!) as ‘proof’ that blacks average such higher levels of testosterone in comparison to whites.
Ross et al (1986) is one of the most important studies to rebut for this hereditarian claim that testosterone causes all of these maladies in black American populations. Ross et al (1986) propose that higher levels of the hormone lead to the higher rates of prostate cancer in black American populations. However, meta-analyses do not show this (Zagars et al, 1998; Sridhar et al, 2010).
Rushton et al’s assertions—largely—lie on this supposed testosterone difference between the races and how it supposedly leads to higher rates of crime, prostate cancer, aggression, and violence. However, the truth of the matter is, this is all just hereditarian bullshit. Larger analyses—as I have extensively documented—do not show this trend. And even accepting the claim that blacks have, say, 19 percent higher levels of testosterone than whites, it still would not explain the supposed prostate cancer rates between the races (Stattin et al, 2003; Michaud, Billups, and Partin, 2015). Even if blacks had 19 percent higher testosterone than whites, it would not explain higher levels of crime nor aggression due to such a hilariously low correlation of .08 (Archer, Graham-Kevan, and Davies, 2005).
Finally, I have a few words for Michael Hart and his (albeit sparse) claims on testosterone in his 2007 book Understanding Human History.
Hart (2007) writes:
(Many of these differences in sexual behavior may be a consequence of the fact that
blacks, on average, have higher levels of testosterone than whites.7) (pg. 127)
And….. footnote number 7 is…. surprisingly (not): 7) Ross, R., et al. (1986). Not going to waste my time on this one, again. I’ve pointed out numerous flaws in the study. (I will eventually review the whole thing.)
It seems unlikely, though, that the higher testosterone level in blacks — which is largely genetic in origin — has no effect on their sexual behavior (pg. 128; emphasis mine)
This is bullshit. People see the moderately high heritability of testosterone (.60; Harris, Vernon, and Boomsma, 1998) and jump right to the “It’s genetics!!!” canard without even understanding its production in the body (it is a cholesterol-based hormone which is indirectly controlled by DNA, there are no ‘genes for’ testosterone). Here are the steps: 1) DNA codes for mRNA; 2) mRNA codes for the synthesis of an enzyme in the cytoplasm; 3) luteinizing hormone stimulates the production of another messenger in the cell when testosterone is needed; 4) this second messenger activates the enzyme; 5) the enzyme then converts cholesterol to testosterone
I have documented numerous lines of evidence showing that testosterone is extremely sensitive to environmental factors (Mazur and Booth, 1998; Mazur, 2016), and due to the homeodynamic physiology we have acquired due to ever-changing environments (Richardson, 2017), this allows our hormones to up- or down-regulate depending on what occurs in the environment. The quote from Hart is bullshit; he doesn’t know what he’s talking about.
For females in Siberia, the disadvantages of failing to find a man who would
provide for her and her children during their childhood were much greater than they were in tropical climates, and females who were not careful to do so were much less likely to pass on their genes. Furthermore, because females in harsh climates were so demanding on this point, males who seemed unlikely to provide the needed assistance found it hard to find mates. In other words, there was a marked sexual selection against such males. Such selection could result, for example, in the peoples living in northerly climates gradually evolving lower levels of testosterone than the peoples living in subSaharan Africa. (pg. 131)
This is a bullshit just-so story. Africans in Africa have lower levels of testosterone than Western men (Campbell, O’Rourke, and Lipson, 2003; Lucas and Campbell, and Ellison, 2004; Campbell, Gray, and Ellison, 2006).
Note also that a difference in testosterone level frequently affects not
only the sexual behavior of a young male, but also his aggressiveness.
No it does not (Archer, Graham-Kevan, and Davies, 2005).
Thankfully, that’s all he wrote about testosterone. There is so much bullshit out there. Though, people who like and seek out the truth will learn that there are no racial differences and that testosterone does not cause crime/aggression/prostate cancer and that it’s just hereditarian bullshit.
The evidence I have amassed and the arguments I have given point to a few things: 1) the races do not differ in testosterone/there is a small negligible difference; 2) testosterone does not cause crime; 3) testosterone does not cause aggression; 4) black women do not have higher levels of testosterone than white women; 5) high levels of testosterone do not cause prostate cancer; and 6) even allowing a 19 percent black/white difference will not have hereditarian claims hold true.
So for anyone who comes across my old articles on testosterone and sex/race, do a bit more reading of my newer material here to see my new viewpoints/arguments. DO NOT cite these articles as proof for your claims of higher levels of black men/women. DO cite the old articles ALONG WITH the new ones to show how and why my views changed along with the studies I have cited that changed my view. (Actually understanding the production of testosterone in the body was a huge factor too, which I talk about in Why Testosterone Does Not Cause Crime.)
The “N” Word
1300 words
Numerous academics have been looked at as pariahs for uttering this word. This word has a pretty long history offending people. The word I’m talking about is natural. This “N” word—especially today—is extremely divisive in today’s society. If you say that something is ‘natural‘, are you taking away any accomplishments that one has done, all because it’s ‘natural‘?
Take what I’ve been writing about for the past three weeks: athletics. If you say that one is a “natural” at athletic competition, are you taking away the hard work it took for that specific athlete to accomplish his goal? No way. You’re acknowledging that that specific individual has something special that sets him apart from the average person. That’s not to say that hard work, determination, and confidence don’t matter; on the contrary. They DO matter. However, like I said with the Kalenjin Kenyan distance runners (who do have anatomical/physiologic advantages in regards to sprinting): you can take someone with elite genetics who has done elite training and put him up against someone who has subpar genetics (in terms of the athletic event) with elite training—the same training as the athlete with elite genetics—and the athlete with elite genetics/muscle fibers/physiology will constantly blow away the individual who is less genetically gifted.
People readily admit that certain races excel at certain physical activities whereas other races don’t fare as well. As I’ve extensively covered (and provided more than enough evidence/arguments for), the races differ in the number of muscle fibers which cause higher rates of obesity in blacks; this causes strength differences which then correlate with mortality. Finally, somatype is extremely important when speaking about athletics. Blacks have a mesomorphic somatype, which, along with their fiber typing and physiologic differences on average compared to whites, cause blacks to dominate most sporting events. However, when you say that certain races are “naturally more intelligent than others“, people all of a sudden have a bone to pick.
This “N” word when it comes to athletics is perfectly fine to use in our vocabulary, yet when we begin talking about intelligence differences—between races and individuals—all of a sudden we think that everyone is the same and that all brains are made the same. We believe that, although humans evolved genetically isolated for thousands of years and have incurred anatomic/physiologic differences, that one organ—the brain—is somehow exempt from the forces of natural selection. I can think of no traits that WON’T get selected for/against, and so I can think of no reason why the brain wouldn’t be under different selective pressures in Siberia/Northern Europe/the Americas/Africa/PNG/Australia.
However, as far as I can tell, we have not found any alleles that differ between populations. It was proposed in 2005 that the genes ASPM and Microcephalin influenced brain growth (Evans et al, 2005; Mekel-Brobov et al, 2005). However, two years later, Rushton, Vernon and Ann Bons (2007) showed that there was no evidence that Microcephalin and ASPM were associated with general mental ability (GMA), head circumference or altruism. Peter Frost cites Woodley et al, (2014) showing that the correlation between microcephalin and IQ is .79, whereas the correlation with ASPM and IQ was .254. Woodley et al (2014) also show there is a correlation between Disability Adjusted Life Years (DALY) and Microcephalin. The reasoning is that Microcephalin may improve the body’s immune response to viral infections, enabling humans to live in larger societies and thus get selected for higher IQ. Since the allele seems to give better disease resistance, then, over time, selection for higher intelligence can be selected for since fewer people are dying from disease due to increased resistance.
Nevertheless, the debate is still out on this allele. However, the data does look good in that we may have found certain polymorphisms that differ between populations which may explain some racial differences in intelligence. (For more information on IQ alleles, see Race and IQ: the Case for Genes).
Now, we are beginning to have some good evidence pile up showing that there are population differences in these alleles, and that they do predict intelligence. Racial differences in intelligence aren’t accepted by mainstream science and the public at large (obviously) like physiologic/anatomic differences are between human populations. Populations are split for thousands of years. They evolve different anatomy/physiology based on the environment. So, then, why wouldn’t psychological differences appear between the races of Man, when other, physical changes occurred from the OoA migration? It literally makes no sense.
People readily admit that athleticism is largely “natural“, yet when someone says that differences in intelligence are largely due to genes they get shouted down and called a ‘racist’, as if that adds anything to the dialogue. People readily admit that individuals/races are “naturally” leaner/stronger/faster/have quicker reflexes. But if one just even hints at thinking about “natural” differences between populations when it comes to general mental ability, they will be shouted down and their careers will be ruined.
Why? Why are people so scared of the “N” word? Because people want to believe that what they do or do not accomplish comes down to them as an individual and only them. They don’t want to think about the complex interaction between genes x environment and how that shapes an individual’s life path. They only think about environment, and not any possible genetic factors. Certain people—mostly social science majors—deny that evolution had ANY impact on human behavior. The “N” word, especially in today’s society, is a completely divisive word. State that you hold hereditarian views (in terms of mental ability) in regards to differences between populations and athletic events and no one will bat an eye.
“Didn’t you see Usain Bolt blow away the competition and set a new world record in the 100m dash at 9.58 seconds?!”
“He’s naturally good, he was born a gifted athlete.”
No one will bat an eye if you say this. This is where the tables will be flipped if you say:
“Don’t you know that differences in intelligence are largely genetic in nature and no matter how much you ‘train the brain’ you’ll stay at that intelligence level?”
“Man, that’s racist. That shouldn’t be looked at. We are all the same and equal. Except when it comes to certain athletic events, then we are not equal and some populations have natural predispositions that help them win. Evolution stopped at the neck 100kya; the only parts of the body under selective pressure over the past 100kya is below the neck!”
People who say this need to explain exactly what shields the brain from selection pressures. Man originated in Africa, the descendants of the soon-to-be coalesced races spent tens of thousands of years in differing environments. You need to do different things to survive in different environments. Just as the races differ physically, they differ mentally as well. Evolution did not stop at the neck. Significant changes in the brain have occurred in the past 10,000 years. There was a trade-off with agriculture, in that it was responsible for the population explosion which was responsible for mutations that affect intelligence and thus get selected for.
The “N” word is not a scary word. It is, in fact, it’s just common sense. People need to realize that by accepting genetic explanations for black domination in sports, that they would then, logically, have to accept racial differences in intelligence. It makes no sense to accept evolutionary theories (even if you don’t know it) in regards to athletics and not accept the same evolutionary theories for racial differences in the brain. There are real differences between populations, in both anatomy/physiology and our mental faculties and brain organization. If you accept one, you have to accept the other.
Guns, Germs, and Steel: A Refutation
Of course the allegations of “racism” arise, as usual when in discussions of racial differences in intelligence and level of civilizational achievement. Rushton also says:
Racial differences in brain size and IQ map very closely to the same cultural histories Diamond explains. Although Diamond dismisses such research as "loathsome", he fails to tell his readers what, if anything, might be scientifically wrong with any of it. One hundred years of research has established that East Asians and Europeans average higher IQs than do Africans. East Asians, measured in North America and in Pacific Rim countries, typically average IQs in the range of 101 to 111. Caucasoid populations in North America, Europe, and Australasia typically average IQs from 85 to 115 with an overall mean of 100. African populations living south of the Sahara, in North America, in the Caribbean, and in Britain typically have mean IQs from 70 to 90.Racial differences in brain size and IQ map very closely to the same cultural histories Diamond explains. Although Diamond dismisses such research as "loathsome", he fails to tell his readers what, if anything, might be scientifically wrong with any of it. One hundred years of research has established that East Asians and Europeans average higher IQs than do Africans. East Asians, measured in North America and in Pacific Rim countries, typically average IQs in the range of 101 to 111. Caucasoid populations in North America, Europe, and Australasia typically average IQs from 85 to 115 with an overall mean of 100. African populations living south of the Sahara, in North America, in the Caribbean, and in Britain typically have mean IQs from 70 to 90.
Ethnic Differences in Sleep, Obesity, and Metabolic Syndromes
2300 words
Ethnic differences in the prevalence of obesity occur, majorly in part due to differences in the rates of metabolic syndrome (which is actually a few variables including high blood pressure, high blood sugar which leads to insulin resistance, excess visceral fat around the waist which is the ‘skinny fat‘ phenomenon, and abnormal blood pressure levels) and obesity. Ethnic differences in these variables do, in part, show how the three ethnies differ in rates of obesity. I will discuss the differences between each ethny in regards to metabolic syndrome and sleep and how it leads to the differences in ethnic obesity rates.
Sleep Differences
There is a ‘missing hour of sleep‘ when comparing blacks and whites. On average, blacks get 6.05 hours of sleep while whites get 6.85 hours of sleep. Of course, the same old racism argument comes up, which, if one ‘percieves’ discrimination, I wouldn’t doubt that it would have an effect on sleep due to a rise in cortisol, which affects sleep due to the raised levels making you restless and not able to fall asleep. Insulin levels then rise due to the rise in cortisol, which is the cause of obesity.
Some studies may try to say that racism and other forms of discrimination are a factor, without even thinking of genetic factors. Another study that Frost cites says that duration of deep sleep and duration of stage 2 (light sleep) is correlated correlated in African Americans with perceived discrimination. The authors defined ‘perceived discrimination’ as the extent to which one believes that their ethnic group have been discriminated against by society. Still even when controlling for discrimination, there were still marked differences between blacks and whites and how long they slept.
Frost then talks about how sleep patterns are heritable and cites studies done on Africans in Africa. One study found that there was an hour sleep difference between Ghanaians and Norwegians on the week days and between a quarter to half hour less on weekends. He shows another study showing that Nigerian college students sleep 6.2 hours a day while getting 70-minute naps in the afternoon.
Frost concludes that the African sleep patterns is normal on Africa. Africans are more active during the cooler times of the day and sleep during the bitter periods. Frost says those who evolved in more northerly climes are particularly adapted to a certain sleep pattern with the same holding true for Africans.
However, these sleep patterns in first world countries have negative effects on metabolism and rates of obesity.
Here are some more studies showing that blacks sleep less than whites:
The sleep of African Americans: a comparative review: The researchers found that blacks take longer to fall asleep than whites, report poorer sleep quality, have more light and less deep sleep, and nap more often and longer. This is a huge recipe for risk factors for obesity, and it shows in their demographics.
Unfair Treatment is associated with Poor Sleep in African American and Caucasian Adults: Pittsburgh SleepSCORE Project: This is one of the studies spoken about above that show that discrimination leads to less sleep. Though, it holds for both black and white adults. The researchers conclude:
Taken together, the confluence of perceived unfair treatment as a chronic stressor and poor sleep and the interplay between the two may have critical roles in long-term health problems.
African Genetic Ancestry is Associated with Sleep Depth in Older African Americans: The researchers hypothesized that “racial differences in sleep phenotypes would show an association with objectively measured individual genetic ancestry in AAs.” They conclude that the slow wave sleep may have genetic underpinnings.
Mexican Americans sleep less than do Mexican immigrants. US-born Mexicans are 40 percent more likely to be short sleepers. This is attenuated by environmental factors such as smoking and stress, which shorten the duration of sleep (smoking decreases the Body Set Weight, whereas cortisol along with insulin in tandem increase it).
Also, in this study by Roane et al (2014) looked at the link between sleep disturbances and stress in Mexican Americans (average age 55) and non-‘Hispanic’ whites (average age 66). Mexicans reported higher levels of sleep disturbance (25 percent) compared to whites (17 percent). They conclude that disturbed sleep was positively correlated with depression.
So both blacks and Mexicans sleep less than whites. These differences in sleep between these three ethnies also affect the prevalence of obesity in these populations.
Obesity and Sleep
It’s long been known that poor sleep habits make people fat. This is due to the effects of insulin and cortisol. Increased insulin comes before increased cortisol–increased insulin is the cause for obesity. Sleeping less is linked to obesity. Since, as described above, the three ethnies differ in sleep patterns, the same also holds true for obesity rates (Ogden at al, 2014). The trends are as follows: 67.3% for whites, 75.6% for blacks, and 77.9% for Hispanics. Though, sleep is only one factor involved with obesity.
Getting adequate sleep is extremely important. Not doing so can lead to a myriad of negative health implications:
Sleep is an important modulator of neuroendocrine function and glucose metabolism and sleep loss has been shown to result in metabolic and endocrine alterations, including decreased glucose tolerance, decreased insulin sensitivity, increased evening concentrations of cortisol, increased levels of ghrelin, decreased levels of leptin, and increased hunger and appetite. Recent epidemiological and laboratory evidence confirm previous findings of an association between sleep loss and increased risk of obesity.
So a lack of sleep leads to an increase in ghrelin levels, decreased levels of leptin (the same effects as caloric restriction over time), increased appetite and hunger, increased evening cortisol (which insulin spikes then follow), decreased insulin sensitivity (the cortisol brings it back up and most people are insulin resistant independent of diet), decreased glucose tolerance, etc. We can see that these ethnic differences in sleep, which are partly genetic in nature, can and would have great effects on metabolism, contributing to the ethnic differences in obesity rates.
And from Harvard:
For example, in the Nurses’ Health Study, researchers followed roughly 60,000 women for 16 years, asking them about their weight, sleep habits, diet, and other aspects of their lifestyle. (2) At the start of the study, all of the women were healthy, and none were obese; 16 years later,women who slept 5 hours or less per night had a 15 percent higher risk of becoming obese, compared to women who slept 7 hours per night. Short sleepers also had 30 percent higher risk of gaining 30 pounds over the course of the study, compared to women who got 7 hours of sleep per night.
Damn!! This, pretty much, mirrors the black-white difference. I’d love to see a racial breakdown of this cohort and will keep an eye out for one, but in the meantime, those who were short sleepers had a 30 percent higher risk of gaining 30 pounds over the course of the study in comparison to women who got 7 hours of sleep per night. Blacks are the most likely group to be overweight and obese in the US, and this data from the Nurses Health Study (which tons of data can be drawn from this study) shows one reason why, however the driver is cortisol > insulin > processed carbs > increased insulin > insulin resistance > increased insulin > vicious cycle > obesity. These differences in sleep almost perfectly mirror the ethnic differences in obesity.
There are several possible ways that sleep deprivation could increase the chances of becoming obese. (1) Sleep-deprived people may be too tired to exercise, decreasing the “calories burned” side of the weight-change equation. Or people who don’t get enough sleep may take in more calories than those who do, simply because they are awake longer and have more opportunities to eat; lack of sleep also disrupts the balance of key hormones that control appetite, so sleep-deprived people may be hungrier than those who get enough rest each night.
Ah the old ‘exercise to increase the Calories Out part of the equation’. however, Calories Out does not stay constant. This also rebuts the ‘Eat Less and Move More’ CICO (Calories In/Calories Out) model of obesity, showing that because it doesn’t take insulin into account, it’s doomed to fail.
Speaking of insulin, it’s about time I focused on metabolic syndrome.
Metabolic Syndrome
As I discussed in a previous post, Race, Obesity, Poverty, and IQ, metabolic differences exist between race/ethnicity. ‘Hispanics’ metabolize carbohydrates differently, blacks have a lower fiber intake (increased fiber protects against obesity, another correlate) while whites have a more high fat diet. Contrary to popular belief, dietary fat doesn’t make you fat as it’s the macro that spikes your insulin the least.
Diaz et al (2005) showed that minority populations are more likely to be affected by diabetes mellitus which may be due to less healthy diets and/or genetic factors. Using the National Health and Nutrition Survey for 1999-2000, they analyzed overweight, healthy adults, calculating dietary intake variables and insulin sensitivity by ethnicity. They characterized insulin resistance with fasted insulin, as those who are more likely to become insulin resistant have higher fasted insulin levels (levels taken after waking, with the subject being told not to eat the night before as to get a better reading of fasted insulin levels). Non-‘Hispanic’ whites had higher energy and fat intake while ‘Hispanics’ had higher carb intake with blacks having lower fiber intake. Blacks and ‘Hispanics’ were more likely to have lower insulin sensitivity. However, ‘Hispanics’ were more likely to have lower insulin sensitivity even after controlling for diet, showing that metabolic differences exist between ethnicities that affect carbohydrate metabolism which leads to higher rates of diabetes in those populations.
In ‘Hispanics’, several loci were discovered that play a role in hepatic (relating to the liver) fat content. Along with showing that ‘Hispanics’ have lower insulin (which due to low insulin, blood glucose builds up in the blood stream leading to diabetes) and showing that they metabolize glucose in the liver differently due to differing loci leading to more cases of fatty liver, this shows how and why ‘Hispanics’ have higher rates of Type II Diabetes Mellitus (TIIDM).
Since TIIDM affects Mexican Americans more, better measures to address their differences in carbohydrate metabolism need to be taken. Racial and ethnic differences in TIIDM are as follows:
7.6% of non-Hispanic whites
9.0% of Asian Americans
12.8% of Hispanics
13.2% of non-Hispanic blacks
15.9% of American Indians/Alaskan Natives
Whites eat a higher fat diet, which means a decrease in carbs. Asians eat white rice which spikes blood glucose eliciting a high insulin response leading to TIIDM, ‘Hispanics’, non-‘Hispanic’ blacks, and Indians and Alaskan Natives (I wish they separated Indians and Alaskan Natives as I’m almost positive that Alaskan natives have a lower rate) all eat high carb, low fat, low protein diets. Carbohydrates are a main staple, and since they spike insulin the most, they are the cause for obesity and TIIDM rates in these populations.
Turning my attention over to metabolic syndrome and blacks and whites, we can see that black women with PCOS have an increased risk for cardiovascular disease and metabolic syndrome in comparison to white women with PCOS. The researchers say that after controlling for age and body mass index (BMI) “black women with PCOS had a significantly increased prevalence of low high-density lipoprotein and high glucose. The general CVD risk was significantly increased in black adults with PCOS.” Though, a longitudinal study needs to be carried out to assess the independent impact of race and PCOS with CVD (Cardiovascular Disease).
Blacks have a higher chance to be diagnosed with metabolic syndrome since they are also at increased risk to have elevated blood pressure (hypertension), become obese, and be diabetic. This is due to their diet, which is due to their low IQ (obesity is correlated with intelligence), and different metabolism in comparison to whites.
There are also metabolic differences between race and sex. Fat oxidation is lower in black than white men and in African American men/women and white men/women, they have a lower metabolic rate!!! 24-hour energy expenditure is lower in black women in comparison to white women, whereas physical activity energy expenditure (PAEE) is the same as whites. Contrasted with women, black men had higher PAEE than white men. The authors conclude:
In conclusion, this comparative study of 24-h energy metabolism in African Americans and whites with use of a respiratory chamber not only confirms the previous findings from ventilated-hood studies of a lower resting metabolic rate, but also suggests a lower 24EE in African American women than in white women. Although only marginal ethnic differences in metabolic rate were found in men, African American men seem to have a lower rate of fat oxidation than do white men. The underlying mechanisms for these sex differences and the significance of these findings with respect to the development and maintenance of obesity remains to be investigated in longitudinal studies.
Metabolic Syndrome and Obesity
Are Australoids and Pacific Islanders Negroid? A Reply to PumpkinPerson
1600 words
I’ve been in a few discussion with PumpkinPerson on phenotype and if the similar phenotype found in Australoids and Pacific Islanders meant they were Negroid. However, just because two *dissimilar groups* look *phenotypically similar*, that doesn’t mean that they are *genotypically similar*. Afrocentrists have also latched on to this ridiculous theory, saying that blacks are ‘all over the world, displaced by whites yada yada yada’. Today, I’ll show that just because those two groups look similar to Africans doesn’t mean that they are similar on the genotype.
PP wrote an article last week, The importance of leaving Africa, which I will be quoting from for the remainder of this article.
The root of this debate is not so much genuine scientific disagreement, but ethnic genetic interests. The black Afrocentrists believe it’s good for black people to be seen as part of this larger, global black community, thus dispelling the claim that blacks only left Africa in chains. For leaving Africa was one of the milestones that separates humans from our closest living relatives (chimpanzees), so the claim that blacks never left Africa is seen as racist indeed.
I agree here that Ethnic Genetic Interests is the main driver of the dispute.
But if the mere leaving of Africa did indeed screen for IQ, why do the Australoids score even lower on IQ tests than sub-Saharan Africans do, and have somewhat smaller brains
Because the environment is similar it would select for similar phenotypes, but just because the environment is extremely similar doesn’t mean that no genetic change occurred in the 70 ky that Australoids left Africa in.
By contrast, the non-black HBDers think it elevates their racial status to promote the idea that their ancestors did something that blacks couldn’t accomplish: leaving Africa.
Well, as I’ve covered here last year (time flys), those who left Africa had specific alleles, the DRD7 and DRD4 alleles, which are absent from SSA populations. This ‘wanderlust’, due to the DRD7 allele, is the *cause* of the migration OoA. It has nothing to do with being more intelligent than those who stayed, it has to do with the genetic mutation that arose from a common ancestor around the time of the OoA migration. The cause of the migration does come down to genetic differences in the founder population (s), but not intelligence differences.
Two notes on the DRD4 allele: populations with a history of migration have a higher chance of having the allele in comparison to sedentary populations. And: a correlation of .85 was found between km traveled and the rate of DRDR4 allele frequency distributions. These alleles are more prevalent in South America, which is not surprising since they had to travel the furthest.
PP then starts talking about why Australoids have lower IQs, saying:
With agriculture/civilization, the dark caucasoids traveled the World, spreading their high IQ mutation to every corner of the globe except those that are most isolated. So the mean genetic IQ of the entire World increased by 13 points, with the exception of places that were too hard to get to, such as Australia and Papua New Guineas, the Congo rain forest, the Southern tip of Africa, and the Americas. Since most of sub-Saharan Africa got the genes, they suddenly leaped from having lower IQs than the Austaloids, to being smarter (only the bushmen and pygmies, who like the Australoids, were too isolated to get the genes, remained behind the Australoids).
This is a great hypothesis. It makes a lot of sense. The ‘Dark Caucasoids’ as PP calls them, better known as Anatolian/Neolithic Farmers could have had a higher chance for more high IQ mutations due to the fact that they could farm and thus have a higher population giving more of a chance for higher IQs.
The downfall for the dark caucasoids was spreading these genes to whites and East Asians. Because of cold winters, East Asians and whites were smarter than pre-mutation dark caucasoids, and now with these mutations, they were smarter once again.
I’m confused here. What we call whites today did not exist that far back in the past. Europeans are an amalgamation of four different ancient populations, basically are an amalgamation of ‘Dark Caucasoids’. Is he also saying that the Neolithic Farmers were more intelligent than East Asians?
Eurasians didn’t become a distinct breeding group until the end of the last Glacial Maximum. This is why there is ‘genetic similarity’ to modern-day Europeans with some old, 10k year plus peoples in the Americas. Because the two groups didn’t split into distinct populations, they show a similar genotype. This is what proponents of the Solutrean Hypothesis need to get through their heads. (I recently got into a nice discussion over at The Alternative Hypothesis, scroll down for comments. I’m going to make a more comprehensive post on the SH in the near future as I have come across even better data on it.)
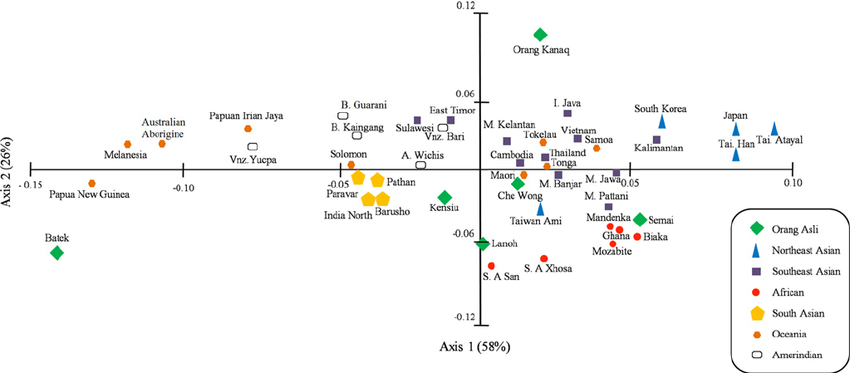
We can see from this PCA graph (from Zainel Abidin et al) that Australoids don’t even cluster in the vicinity of Africans. They are on the complete other side of the graph, showing how great of a genetic distance there is between these two populations. You can see the other Oceanic peoples (the orange dots, who Afrocentrists and others say are Negroid, Abos, Papuans, Melanesians, etc) are also clustered away from Africans. PCA graphs show that the three populations are not genetically similar and that phenotype, sometimes, isn’t enough to show who belongs to what racial grouping. PCA analysis refutes peoples ‘feelz’ on what they believe with their eyes. Even with this data, their ‘feelz’ still overrides the truth and they still believe lies.
While on this subject of similar phenotype not meaning one population is racially the same as another, people use this same fallacious reasoning for ‘white-looking’ peoples in the ME.
Quoting Razib Khan:
The final issue is that a lot of the phenotypes that we racially code are recent. This probably explains why groups like the Kalash and Nuristanis can look more like Europeans than South Asians, but they’re genetically more like South Asians.
What does any of this have to do with non-scientific things? I don’t really know. My interest in population structure is intellectual, not personal. But a certain type of person should probably stop talking about how white people have been in Europe for 40,000 years. First, the ancestors of modern Europeans 40,000 years ago were almost all residing outside of Europe. An assertion that holds until 15,000 years ago. And most would still be resident outside of Europe 8,000 years ago as depending on how you count/calculate. *** And, perhaps more importantly, the typical phenotype of Northern Europeans probably really coalesced only around ~5,000 years ago. ***
How can there be such phenotypic similarity in two populations separated by thousands of miles?
Easy. The Kalash and other ME ‘white-looking’ populations have ancient Siberian ancestry. As shown in my linked article, modern-day Europeans have a great deal of Siberian ancestry, mostly from the true Aryans, the Yamnaya peoples.
And in the comments Razib was asked:
“Could I bother you to list the top three theories/positions that you see falling into this unsupportable category?”
To which he responded:
“that phylogeny and phenotype track closely. just because you can’t tell the physical difference between two pops (e.g., solomon islanders and sub-saharan africans) they must be phylogenetically close. this is not the case.”
Pretty much seals the deal.
Just because populations look similar on the outside doesn’t mean they are genetically similar. As shown from Razib’s post, the phenotypes that we code are relatively recent, which is why there are some populations separated by thousands of miles yet look extremely similar.
Bonus:
This was said in the comments:
I can’t really tell about the genetics since I don’t have the scientific background, but my impression is a lot of those white identity guys have an extremely mythologised view of the past. This seems to be true even of the smarter ones; e.g. I recently read a bit of Richard Spencer’s twitter account (out of interest in the alt right phenomenon) and he throws out such totally retarded comments as “Europe has always been unified, even before Christianity” (totally ignoring what is known about the ancient Greeks’ intimate links to the Near East, the Greeks’ and Romans’ unflattering view of the northern barbarians, the emergence of Latin Christendom in the middle ages and the fairly late rise of the concept of Europe etc.) or “Europe is a nation”. There seems to be little awareness of the complexities of historical change because everything is reduced to some supposedly unchanging racial essence reaching back into the mists of prehistoric times. Now I’m pretty far right and “racist” myself, but a lot of this really seems pretty stupid…like myth-making for identity politics.
i knew the pre-WN richard spencer (we lost touch after his ideological changes ~2010). he’s smart. i have a hard time believing he doesn’t know the latest research, which was evening starting to be evident back then. so i think it’s myth-making.
p.s. a friend of mine sent me a link to a richard spencer interview with kevin macdonald last year i think, pointing to a specific segment of the podcast talking about ancient genetics. kevin was telling richard how europeans 40,000 years ago were white, and those are the ancestors of europeans. that’s wrong.
Europeans 40kya were not white those in the area at that time are *not* the ancestors of today’s Europeans.
Both Afrocentrists and Nordicists need to keep up with the new information that’s constantly coming out. Because what they say in regards to genetics and/or anything else is mostly wrong.
Japan’s Population Decline and r/K Selection Theory
Edit, 7/18/17: r/K selection theory has been rebutted.
r/K Selection Theory: A Response to Rushton
E.O. Wilson on Rushton’s r/K Theory and More on Endemic Disease
r/K Selection Theory: A Response to Anonymous Conservative
r/K Selection Theory: A Response to Truth-Justice
r/K theory doesn’t apply to humans and if it did, Mongoloids would be r and Africans would be K. Cold with is an agent of r selection while endemic disease is an agent of K selection. Rushton used a debunked “continuum” for the basis for his theory and completely changed r and K. However it’s wrong. Rushton was wrong. Anonymous Conservative is wrong. Anyone who uses those two in reference to r/K is wrong by proxy since r/K is a debunked paradigm.
Japan has had a population crisis for a few years. Japan’s fertility rate was 1.4 in 2014. To have enough children to keep the population stable, the Total Fertility Rate (TFR) needs to be 2.1. As a country industrializes and becomes more prosperous, the TFR drops as higher IQ follows better nutrition. As a nation industrializes and becomes more complex, the attention of the populace shifts from one of having children and a family to one of success and intellectualism. As this occurs, the birth rate drops because the more intelligent a population is, the more likely it is for them to pursue higher education or monetary achievement. Clearly, the main reason Japan has concerns with their TFR is due to their high intelligence.
The Japan Times reported yesterday that almost half of single young men and women were virgins. A survey of Japanese men and women aged 18-34 found that 70 percent of unmarried men and 60 percent of unmarried women were not in a relationship. Also discovered, 42 percent of the men and 42.4 percent of the women admitted to being virgins. The survey was taken before in 2010, with 36.2 percent of men and 38.7 percent of women admitting to being virgins.
These surveys have been carried out every 5 years since 1987. Then, the rate of men who said they had no partner was 48.6 percent and for women it was 39.5 percent. The survey, which was conducted last June and accounted for 8,754 single people and 6,598 married couples across Japan, also found that 90 percent of the respondents wanted to get married “sometime in the future”, but for some people, this turns out to be a mistake. Moreover, 30 percent of the 2,760 men and 26 percent of the 2,570 women polled said they were not currently looking for a relationship. The increase in singles was most noted in the 20s, when women are the most fertile. The Prime Minister of Japan, Shinzo Abe also said he wants to increase the birthrate from 1.4 to 1.8 by 2025.
Lastly, the study found that the number of children for couples marries for 15 to 19 years was 1.94, a record low. This study did not ask questions about same-sex partners, but what we are concerned about is the TFR and how it’s driven by evolution, so this is a non-factor.
Japan’s population is dramatically shrinking. In 2010, they had a population of 128 million but by their 2015 census, they had a population of 127 million. This is due to the increase in virgins and an aging population. Why is this happening?
This is, of course, driven by r/K Selection Theory. Rushton thought of r/K Selection Theory, also known as Differential K theory, in 1985 with a paper titled Differential K Theory: The Sociobiology of Individual and Group Differences. Organisms can be r-selected, K-selected or somewhere in between. Humans as a species are K-selected, but some human races and ethnies are more K-selected than others.
Africans are r-selected, meaning that they have many children while not investing too much time in their offspring. They evolved to be r-selected to offset the high mortality rate due to the harshness of Sub-Saharan Africa. Due to this, black girls have an earlier menarche (period) so they can reproduce more to a) offset the high mortality rate and b) have a chance to reproduce more due to the high mortality rate. This is driven by disease, malnutrition, and parasitic load, which also drop IQ and contribute to the high birth rate since lower IQ populations have more children.
Caucasians are in the middle of r and K, and have fewer children and put more energy into caring for each one. This goes back to evolving in the Ice Age where cooperation and altruism were needed. More attention to children was needed for Eurasians evolving back then due to the harsh conditions of the Ice Age. So, a higher IQ evolved, and along with the higher IQ came a bigger brain. The bigger brains of Eurasians led to children being born earlier, and a bigger brain allowed for better care for the children along with numerous other positive variables to help survive in the harsh weather. Moreover, genes from Neanderthals are responsible for a 1 percent decrease in historic fitness (biological fitness) in Eurasian populations.
Orientals (Japanese, Chinese, Koreans) are further K than Caucasians are. This is reflected in brain size, where more K-selected populations have bigger brains, thus they can think further into the future and maximize care for their children. The opposite holds true for blacks. This is reflected in modern-day, first-world life where blacks have too many children to care for on their own accord and whites and Orientals have fewer children and put more investment into their children .
It’s not only Japan that’s having this problem with birthrates. It’s all of the West and East Asia. Higher IQ societies do have a longer life expectancy, while lower IQ societies have a lower one. Then, as described above, the lower IQ populations have more children to offset the mortality rate.
Japan’s birthrate concerns are due largely in part to genetic factors. This is currently occurring in all high IQ populations. Those populations have a large elderly population, with the young demographic quickly shrinking. Seeing this gradient throughout the world with IQ and fertility rates, we can make some general conclusions:
- Low IQ populations have more children while high IQ populations have less children.
- High IQ populations are more likely to have a large subset of virgins, as seen with this article. Lower IQ populations lose their virginity earlier.
This can be seen with the CLASH (CLimate, Aggression and Self-control in Humans) model (Van Lange, Rinderu, and Bushmen 2016). According the the CIA World Fact book 2014, in countries closer to the equator, the average age of first birth for a female was 20 years of age (the countries were the Gaza strip, Liberia, Bangladesh, Kenya, Mali, Tanzania, Uganda and various other middle African countries). Conversely, for countries further away from the equator, the average age of first birth was 28 years of age (Japan, Canada, and most European countries). Those populations that evolved in warmer climates where the changes in season are minimal with unpredictable harshness tend to enact faster life history strategies than those in colder climates.
Moreover, a slower life history strategy (K-selection), under a predictable environment would be better to enhance inclusive fitness. There is a growing body of evidence that predictable environments promote K-selection “in terms of lower mortality, morbidity, delayed reproduction, and a higher contribution towards one’s social capital.” This can be seen with the trends in Western and East Asian countries.
The trend that Japan is facing can be reversed with incentives for reproduction. However, the more intelligent a society is, the fewer children it will have due to evolutionary pressures. Is there a happy medium between IQ and fertility rates, where the population isn’t too dumb and the fertility rates aren’t too low? I’ll explore that in the future.
Black Women and Testosterone
1350 words
(Note: Testosterone differences between the rates are negligible, not high enough to account for differences in prostate cancer mortality. Black males have 2.5 to 4.9 times higher testosterone than white males (see Richard et al, 2014) and my article on the cause for the difference in prostate cancer mortality. The difference in testosterone between the races is not too high, as is commonly believed. Old studies with small ns get cited, when bigger, more robust analyses show the opposite, with a smaller difference. A difference that cannot be attributed to racial differences in prostate cancer.)
(Note 2, 6/23/17: This post is getting a ton of traffic so I need to clarify some things.
Here is a quote from Mazur (2016):
The pattern [high testosterone] is not seen among teenage boys or among females.
…
There is no indication of inordinately high T among young black women with low education.
I cringed pretty hard reading the comments below; I was just like PumpkinPerson arguing something that is not true. However, I am more then capable of admitting that I am wrong with suffcient evidence. Read the most recent posts on testosterone on this blog for more information. End Edit)
The ENA Theory: On Testosterone and Aggressive Behavior by Race/Ethnicity
Why Testosterone Does Not Cause Crime
Testosterone and Aggressive Behavior
Race, Testosterone, and Prostate Cancer
Race, Testosterone, and Honor Culture
It is known that blacks have the highest levels of testosterone out of the major races of humanity. However, what’s not known is that black women have higher rates than white women. The same evolutionary factors that make it possible for black men to have high testosterone make it possible for women as well.
Most people don’t know this, but vitamin D isn’t really a vitamin; it’s a steroid hormone. Higher levels of testosterone occur due to increased exposure to the sun. Of course, the Middle East gets more sunlight than does Europe, so their levels of testosterone will be higher due to increased vitamin D, which in turn increases testosterone, causing more acts of aggression. Vitamin D supplementation could possibly (we know it does) raise testosterone levels. Of course, this is the case, seeing as vitamin D comes from the sun, and the more sun you get, the more Vitamin D you get, which increases testosterone levels. Those populations closer to the equator get more vitamin D from the sun’s rays, and thusly have higher levels of testosterone, on average.
Black women are more androgynous (personal observation, you can’t tell if they’re a man or woman from further away), and are more prone to get in to shouting matches/fights with other men or women. This is the high testosterone at work. Those with higher levels of test are more aggressive and have a more manly look as a result.
Moreover, the higher natural levels of testosterone found in black women are directly responsible for the reason why black men have higher levels of testosterone. Since circulating hormones matter for a woman’s child invitro, it would stand to reason that since black babes are in a woman with higher natural levels of testosterone, that this would pass on to the babe. This is exactly what is observed. One study showed that black women had 50 percent higher testosterone than white women in early pregnancy!! Ross, the head researcher of the study, speculates that “this increased hormonal exposure in utero might reset the so-called “gonadostat feed-back loop,” which regulates testosterone secretion, to a higher level.” With what we know about hormones and babes in the womb, this is a viable hypothesis.
Finally, Satoshi Kanazawa noted in this study that black women were not seen as attractive as women from other races. He says women, on average, are more attractive than men: EXCEPT BLACK WOMEN. The data shows black women as not being statistically different from the average, and far less attractive than whites, Asians, and Native American women.
The cause is higher testosterone. Kanazawa says that the cause for this is due to the mean BMI of black women being 28.5 among black women and 26.1 among non-black women. Though he says that’s not the reason why black women are less physically attractive. Black women have lower levels of intellect net of BMI. Even the racial differences in intelligence don’t account for these differences. Black women are STILL less physically attractive, net of BMI and intelligence. Kanazawa says: “Net of intelligence, black men are significantly more physically attractive than nonblack men.”
Why is that? To be blunt, black women look more like men than women due to their higher levels of testosterone. The amount of crying all throughout the Internet after Kanazawa published his paper says it all: Racist!! Sexist!! Except, they couldn’t respond to the data so of course, as is usually the case with racial/sex differences, bury it, forget about it and proclaim the one who said these uncomfortable truths is a “racist”. Kanazawa ends up concluding that testosterone differences are the only cause for these differences. With blacks having the highest testosterone out of all the races, black women obviously have higher rates of testosterone than white women. Those women with higher levels of testosterone have more masculine features, therefore making them less attractive.
My personal answer as to why black women are less attractive is due to testosterone obviously. But, we as humans can subconsciously detect things such as this. Since high levels of testosterone are correlated with numerous variables that then become masculinzied in black women, this is one very huge reason in my opinion.
Lewis (2010) says in his study Who is the fairest of them all? Race, attractiveness and skin color sexual dimorphism:
Previous research has suggested that perceived attractiveness and personality are affected by the race such that White faces are more attractive but less masculine than Black faces. Such studies, however, have been based on very small stimulus sets. The current study investigated perceived attractiveness and personality for 600 Black, White and mixed-race faces. Many of the investigated personality traits were correlated with race when rated by White participants. Attractiveness specifically was greater for Black male faces than White male faces and among mixed-race faces. Blackness correlated with increased attractiveness. A reverse pattern was found for female faces with Whiteness being associated with attractiveness. The results are discussed in terms of the sexual dimorphism demonstrated in skin color.

2650 words
I first heard of Guns, Germs, and Steel (GGS) a few years ago while in a discussion about racial differences and their causes. The person linked me to the Wikipedia page on GGS. I then looked into it and it seemed to be an OK hypothesis. However, after reading the book myself and then reading critiques he got on it, it’s clear that Jared Diamond was attempting to pick and choose what to put into the book to come to the conclusions he already has come to. There are some interesting tidbits in the books, my favorite being only 14 beasts of burden have been tamed for human use out of 148 large wild creatures that can be tamed. Other than that, he spins facts and data from hereditarians to suit his own agenda.
Jared Diamond started wondering about the reasons for human inequalities after his New Guinean friend, Yali, asked Diamond why Westerners had so much more “cargo” (material possessions) than the New Guineans. Diamond then set forth to find out why human inequality existed. Diamond attempts to say that immediate environment and only environment is the cause of racial inequalities. However, what Diamond fails to say is that genetic isolation over thousands of years is the cause of racial differences in intelligence, muscle fiber typings, crime differences, age of first period, sleep, obesity and metabolic differences, racial/sex differences in testosterone, differences in climate which, over tens of thousands of years cause distinct phenotypic/genotypic differences, child rearing and age of first birth, slow and fast life history (r/K selection), etc. He also fails to bring up brain size differences between races/ethnicities. All of these factors are responsible for racial/ethnic inequalities.
Diamond’s main thesis in GGS is that human inequalities all boil down to amount of resources in the land and how they are able to be used with the geography of the area. He never brings up brain size as it pertains to modern-day humans, EXCEPT in regards to New Guineans and how they are more intelligent than Europeans: (Diamond, 1997: 20, 36, 38, 40, 159, 198, 260):
This is laughable. To say that a tropical people, pretty much isolated from the rest of the world is more intelligent than Europeans is not true at all. Just as Robert Sternberg’s Triarchic Theory of Intelligence fails to explain away racial/ethnic differences in intelligence, so does Diamond’s. Jared Diamond clearly, by his own admission, wants to prove that these differences between humans only come down to immediate environment and are not genetic in nature. The fact that Diamond says that New Guineans are “probably superior to Westerners” … “escaping the devastating developmental damages under which most children in industrialized societies now grow up” shows how biased he is with this whole entire book. IQ tests are great predictors of g, general intelligence, and Westerners clearly are superior in terms of intelligence in comparison to New Guineans. Yea, you can’t build a shelter like they can and you look stupid to them because you can’t do what they can in their society. Duh, of course. The fact that he uses that as any type of evidence or revelation that New Guineans are smarter than Westerners is a wrong and 100 percent ideologically driven statement.
Rushton had some nice words for Diamond on brain size, intelligence: